
Pulmonary tuberculosis, a disease with varied clinical and radiological expression, can sometimes take on a pseudotumoral form, mimicking the features of bronchopulmonary cancer. This unusual presentation poses diagnostic problems, as it can simulate both the clinical and radiological features of a malignant pathology. We present a case of primary lung tuberculous infection after removal of a huge osteosarcoma of the shoulder. To our knowledge there is no similar case in the literature.
We present the case of a 22-year-old patient diagnosed with osteosarcoma of the left shoulder. In the initial staging, including thoraco-abdominal computed tomography and bone scintigraphy (Figure 1), concerns about a possible pulmonary metastasis were raised. Following two cycles of neoadjuvant chemotherapy, amputation of the left shoulder was performed, followed by additional chemotherapy sessions. However, during follow-up [18F]fluorodeoxyglucose positron emission tomography (18FDG PET) imaging, the presence of nodules, predominantly located particularly on the right side, suggested evolution of metastatic lesions. Opinions diverged during the multidisciplinary team meeting. Some believed these were metastases, questioning the necessity of nodule resection for histopathological studies, while others argued for the justification of this intervention, considering the possibility of other diagnoses, such as metastases from another primary source or a different pathology. Computed tomography (CT)-guided biopsy of nodules was inconclusive and induced right pneumothorax, treated by chest drainage (Figure 2), Ultimately, the decision was made to proceed with the atypical resection of some nodules via uniportal video-assisted thoracic surgery (VATS). The post-operative course was uneventful. The results of pathology were surprising, revealing pulmonary tuberculosis rather than metastasis (Figure 3). Six months of anti-tuberculous treatment allowed complete resolution of nodules even on the left side. The follow-up to date has shown no recurrence.

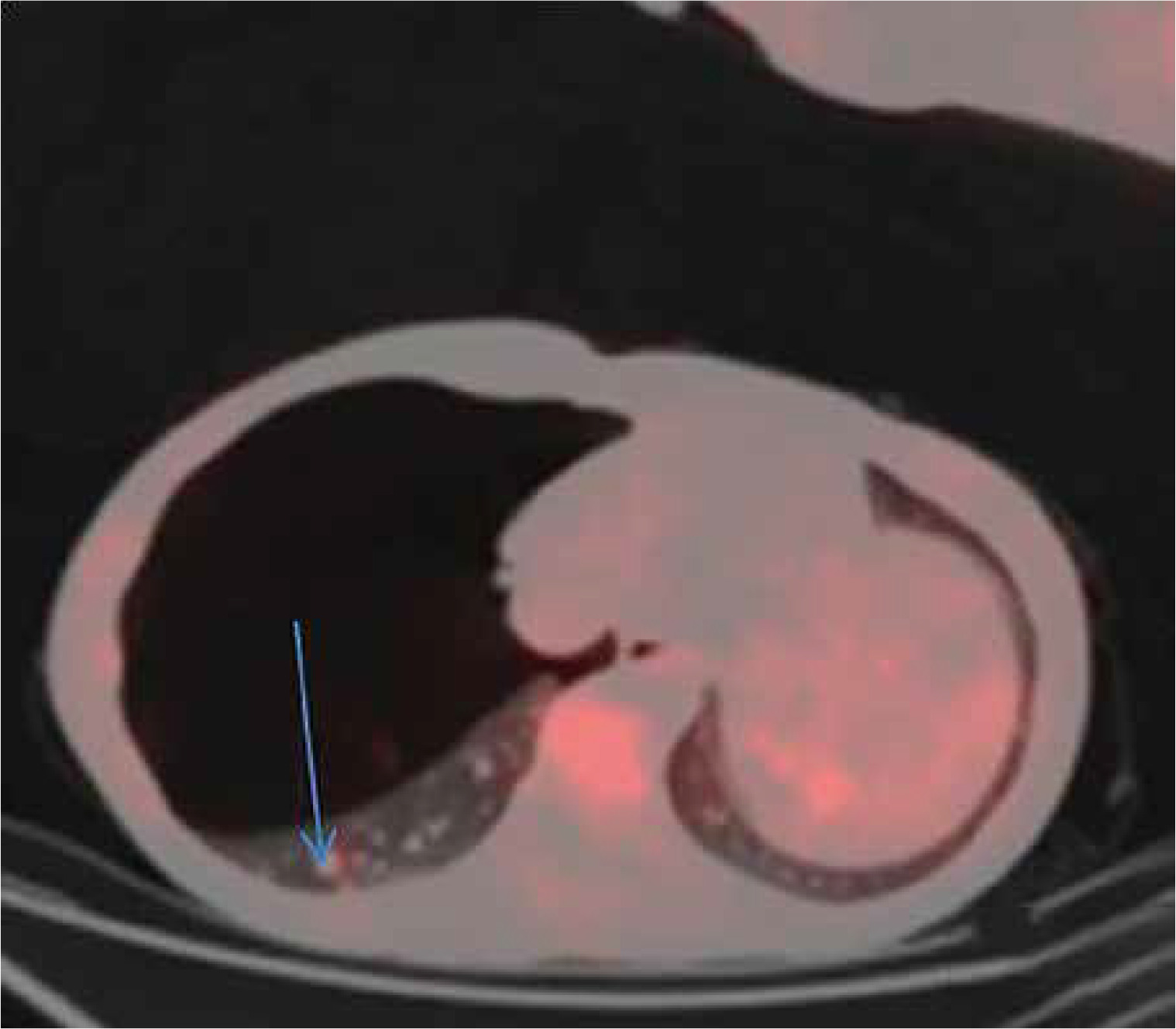
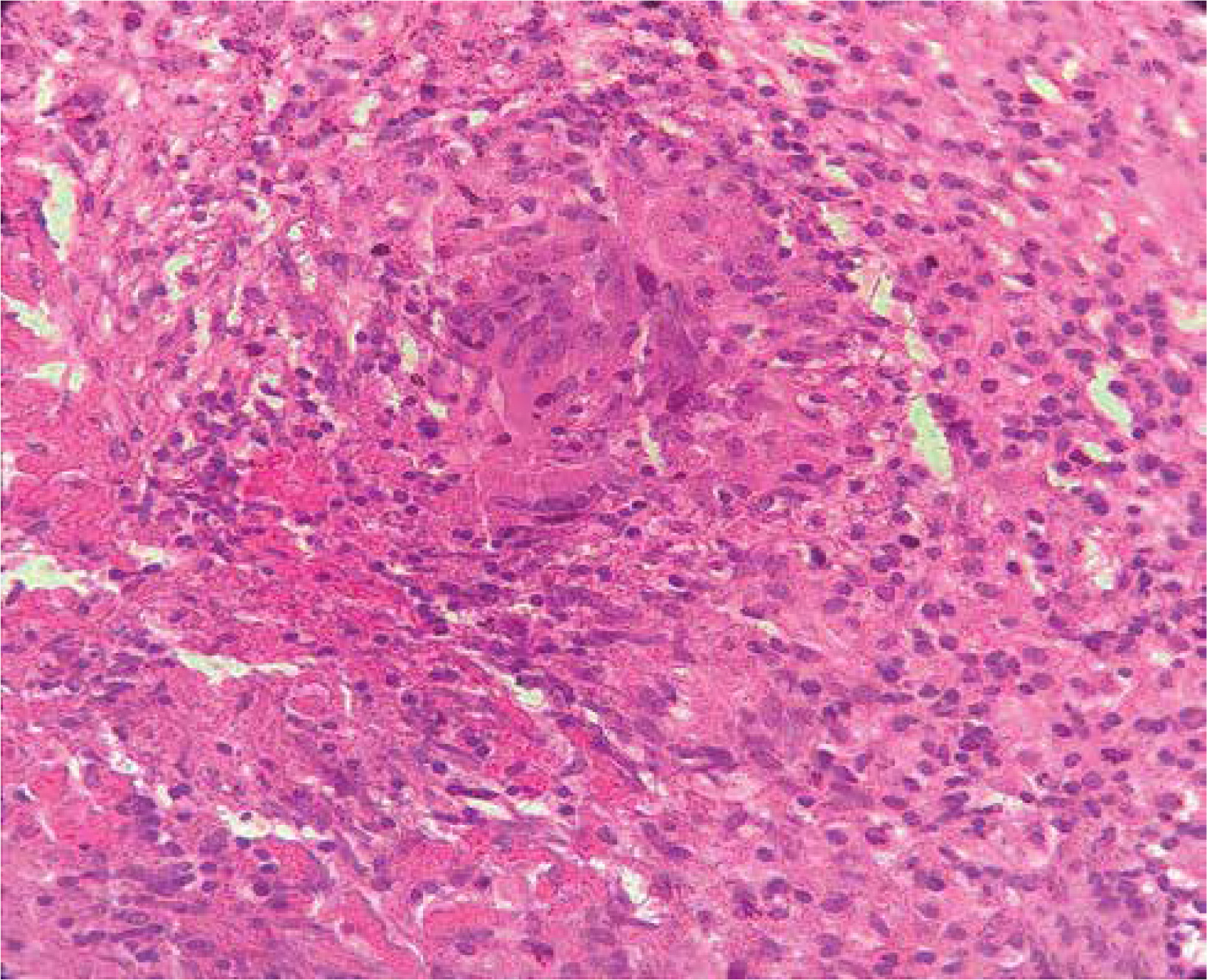
Figure 3
Pathological view: inflammatory reaction consisting of epithelioid and giant cell granulomas with incipient caseous necrosis
Tuberculosis, caused by infection with the tubercle bacillus, can affect any organ, with pulmonary tuberculosis accounting for just over 50% of cases. It is a global public health issue, particularly in our country, Morocco, which is among the countries with moderate tuberculosis incidence. The incidence estimated by the WHO in 2021 is 35,000 cases, corresponding to an incidence rate of 94 per 100,000 inhabitants [1]. The pseudo-tumoral bronchopulmonary tuberculosis is a specific presentation in immunocompetent subjects, appearing as a bronchial or pulmonary lesion suggestive of neoplastic pathology [2]. This similarity to neoplastic pathology confounds clinicians, making the positive diagnosis challenging and often requiring invasive diagnostic means, as conventional methods are usually inconclusive, further complicating patient management and delaying treatment initiation. The objective of this article is to raise awareness among clinicians regarding this particular presentation of tuberculosis. Although uncommon, it should be considered, especially in the presence of a compatible radiological aspect, particularly in highly endemic regions.
The divergence of opinions during the multidisciplinary meeting underlined the complexity of therapeutic decisions. Some questioned the need for nodule resection, advocating a more conservative approach, believing it to be a metastasis after all. Others, however, advocated surgical intervention, exploring multiple potential diagnoses. The unexpected results of the resection, revealing pulmonary tuberculosis, underline the importance of not underestimating the variability of clinical presentations. This unexpected revelation inevitably influenced the patient’s subsequent management, underlining the importance of remaining open to different diagnoses, even when the situation seems clear-cut. The lessons learned from this case go beyond the specific management of pulmonary nodules in patients with osteosarcoma, highlighting the importance of collaborative decision-making, where every member of the multidisciplinary team contributes to resolving diagnostic dilemmas.
Immunosuppression resulting from treatment with certain types of cytotoxic, anti-cancer chemotherapeutic agents may predispose cancer patients to develop active or latent TB infection, particularly in hematological malignancies. Cases have been described for many types of solid tumor and hematological malignancies which cause leucopenia [3, 4]. Cancer-associated immunosuppression may also be exacerbated by other factors such as immunosenescence, malnourishment and cigarette smoking [4, 5]. The association of this infection with lung cancer and smoking is well recognized, while associations of pulmonary TB with non-pulmonary malignancies, including Hodgkin’s lymphoma, malignant melanoma (in males), as well as several other types of cancer, have also been described [5–7] but the association of tuberculosis and osteosarcoma is exceptional. To our knowledge, there is no similar case in the literature.
In conclusion, this complex case of pseudotumor pulmonary tuberculosis, initially masked by a clinical presentation resembling metastasis, highlights the diagnostic challenges clinicians may face, particularly in highly endemic regions such as Morocco. The importance of considering tuberculosis within the spectrum of differential diagnoses, even in the presence of atypical clinical presentations, is crucial.









