
Introduction
The first successful human-to-human heart transplantation was performed by Dr. Christiaan Barnard in 1967 [1]. According to United Network for Organ Sharing (UNOS) reports, 3408 heart transplants had been performed in the US by August 31, 2019. Professor Mohammad Hosssein Mandegar performed the first heart transplant in Iran in July 1993 at Shariati Hospital. As of May 2019, 213 more heart transplants have been performed at this center.
Heart transplant is the final treatment option for patients with end-stage heart failure, which could be the result of cardiomyopathies, heart valve or coronary artery diseases, pulmonary hypertension, ventricular arrhythmia, amyloidosis and congenital heart defects [2, 3]. Other risk factors associated with heart failure may include diabetes [4], HIV [5], myocarditis [6], hyperthyroidism, hypothyroidism [7] and hemochromatosis [8]. Despite the fact that heart transplantation is considered the ultimate therapeutic option for patients with end-stage heart failure, there are several risks associated with this procedure including surgery-related complications (infection, bleeding, stroke, generation of blood clots and heart attack) as well as post-operative complications including organ rejection, transplant coronary artery disease and immunosuppressant-derived side effects (infection, malignancies, diabetes, kidney disease and osteoporosis) [9]. However, organ rejection remains the major cause of mortality and patient’s readmission after heart transplant. The International Society for Heart and Lung Transplantation (ISHLT) has established a standardized grading system for detecting cardiac rejection. This grading system consist of four major grades: Grade 0 represents no rejection, Grade I represents mild rejection, Grade II represents moderate rejection and Grade III represents severe rejection [10].
Aim
In the present study 50 patients received a heart transplant and were assessed for underlying diseases, risk factors, and transplantation outcome and mortality rate during a 5-year follow-up.
Material and methods
The study was approved by the institutional review board of Mashhad University of Medical Sciences and written informed consent forms were obtained from all patients. The present retrospective study was conducted at Imam Reza Hospital in Mashhad. 50 heart transplant candidates with end stage heart disease who received heart transplantation from June 2012 to October 2017 were included in this study. The first and second endomyocardial biopsies (EMB) were obtained 10 and 30 days after surgery. Histopathological evaluation of collected samples for detecting organ rejection was performed based on ISHLT guidelines.
Immunosuppression protocol
All patients received 3-drug immunosuppression according to our protocol. We used rabbit antithymocyte globulins for induction therapy. Azathioprine (GlaxoSmithKline) (4 mg/kg) was administered 1 hour before the operation and solumedrol (1000 mg) was infused upon release of the aortic cross-clamp. Rabbit antithymocyte globulin (1.5–2.5 mg/kg/day) was continued for 5 days after transplantation. Oral cyclosporine (Novartis, New Jersey) was started within 5 days or after renal functional recovery at dosages adjusted based on renal function and drug levels, which were maintained at trough values of 300–500 ng/ml during the first 3 post-transplantation months and 200–300 ng/ml at 1 year thereafter. Azathioprine (1–2 mg/kg/day) was prescribed after transplantation at dosages adjusted to maintain a white blood cell count of 4000–6000/mm3. Prednisone (0.5 mg/kg/day) initiated on postoperative day 2 was gradually reduced to 0.2 mg/kg/day by the first month. Tacrolimus (FK-506) (Fujisawa, Japan) and mycophenolate mofetil (Cellcept) (Roche, Segrate, Italy) were used in cases of recurrent rejection or severe adverse reactions to cyclosporine or azathioprine, respectively. Since 2004, mycophenolate mofetil has been substituted for azathioprine as primary immunosuppression. To minimize nephrotoxicity, the cyclosporine dose was reduced to sustain a level of 250–350 ng/ml during the first 3 months after transplantation and 150–250 ng/ml at 1 year after transplantation.
Rejection survey and biopsy protocol
All patients were followed up 10 day after heart transparent, at Imam Reza Hospital. Patients in the scheduled biopsy group underwent a scheduled endomyocardial biopsy 10 days after heart transplantation in the ICU, and 1, 2, 4, 8 months and one year after heart transplantation. During the follow-up period, 10 days after heart transplantation in the ICU, and 1, 2, 4, 8 months endomyocardial biopsies followed for 1 year, then they were performed yearly with coronary artery evaluations. Rejection was defined as a biopsy-proven pathological finding or clinical event leading to specific immunosuppressive intervention.
Patients’ medical records were created including measurements of age, sex, height and weight, physical examination (patient’s underlying disease, blood type, pre-operative diet, stomach, liver and kidney conditions, psychological state and dental health) and paraclinical findings (including PUMP time and ischemia times). Early and late postoperative complications, mortality and cause of death of all the patients who participated in the follow-up program were also included in the study. Patients who did not attend follow-up appointments were contacted via phone call.
Results
Table I represents epidemiologic measurements of patients’ age, weight and height. The average age, weight and height of patients who underwent heart transplantation as the receiver were 34.9, 60.4 kg and 164 m, respectively. The average age, weight and height of patients who underwent heart transplantation as the donor were 28.3, 95 kg and 166 m, respectively (Table I). The frequency of state of organ capacity in the patients operated on were 5 (10%) urgent and 43 (86%) elective list.
Table I
Patients’ demographic status
| Parameter | Age [years] | Weight [kg] | Height [cm] | |
|---|---|---|---|---|
| Receiver: | ||||
| Minimum | 4.00 | 14.00 | 96.00 | |
| Maximum | 61.00 | 100.00 | 185.00 | |
| Mean | 34.9600 | 60.4082 | 164.1 | |
| Donor: | ||||
| Minimum | 11 | 44 | 97.00 | |
| Maximum | 47 | 30 | 190 | |
| Mean | 28.3 | 95 | 166 | |
Distribution of sex in receivers was 31 (62%) male and 19 (38%) female; in donors it was 40 (80%) male and 9 (18%) female (Table II).
Evaluating patients’ underlying diseases prior to surgery revealed that dilated cardiomyopathy (DCM) was the most common underlying disease with prevalence of 28 (56%) followed by ischemic cardiomyopathy (ICM) with prevalence of 6 (12%), while diabetes with prevalence of 2 (4%), and valvular cardiomyopathy (VCM), arrhythmogenic right ventricular cardiomyopathy (ARVC), mitral valve replacement (MVR), and restrictive cardiomyopathy (RCM) with prevalence of 1 (2%) were also observed. Eight patients in this study did not have any underlying disease (Tables II, III, Figure 1).
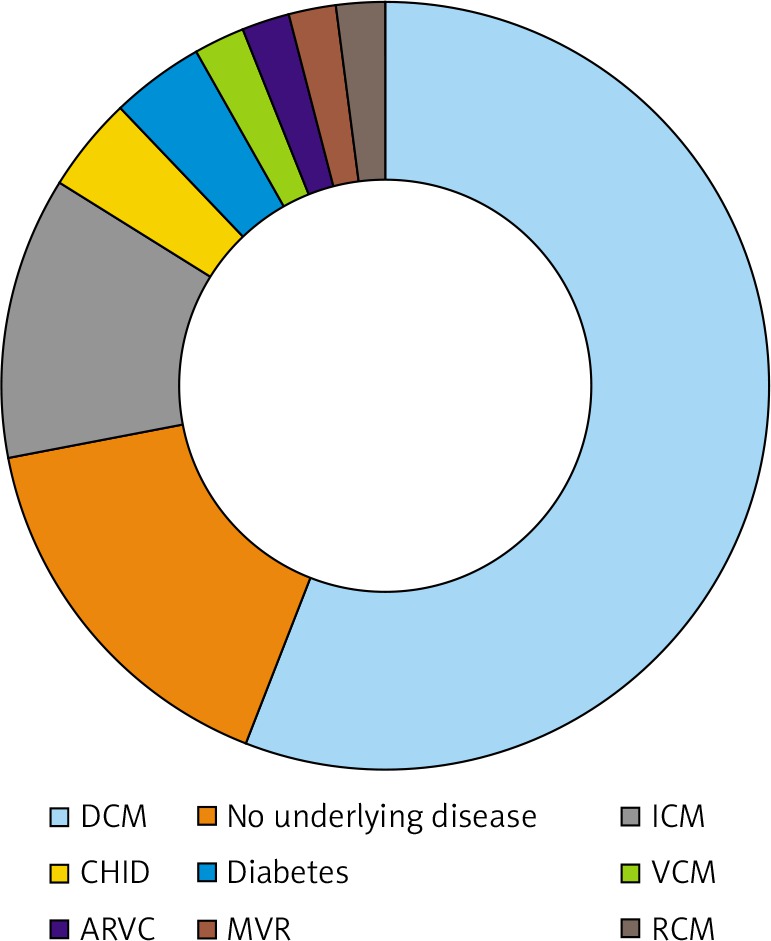
Table III
Distribution of different underlying diseases in patients
| Underlying disease | Frequency | Percentage |
|---|---|---|
| DCM | 28 | 56 |
| No underlying disease | 8 | 16 |
| ICM | 6 | 12 |
| CHID | 2 | 4 |
| Diabetes | 2 | 4 |
| VCM | 1 | 2 |
| ARVC | 1 | 2 |
| MVR | 1 | 2 |
| RCM | 1 | 2 |
| Total | 50 | 100 |
Blood type determination of patients showed that A+ was the most frequent blood group type with prevalence of 32%, followed by B+ (26%), O+ (22%) and AB+ (10%), while AB–, A–, B– and O– were the rarest blood group types with prevalence of 2%.
Twenty-one (42%) out of 50 patients were under treatment for weight loss or gain, 3 (6%) were receiving medication for liver disease, 10 (20%) had kidney disease, 16 (32%) had dental decay and 5 (10%) were under treatment for stomach disease. Echocardiographic assessment of patients before and after heart transplant showed significant improvements (42.55%) in ejection fraction (EF) (Table IV, Figure 2).
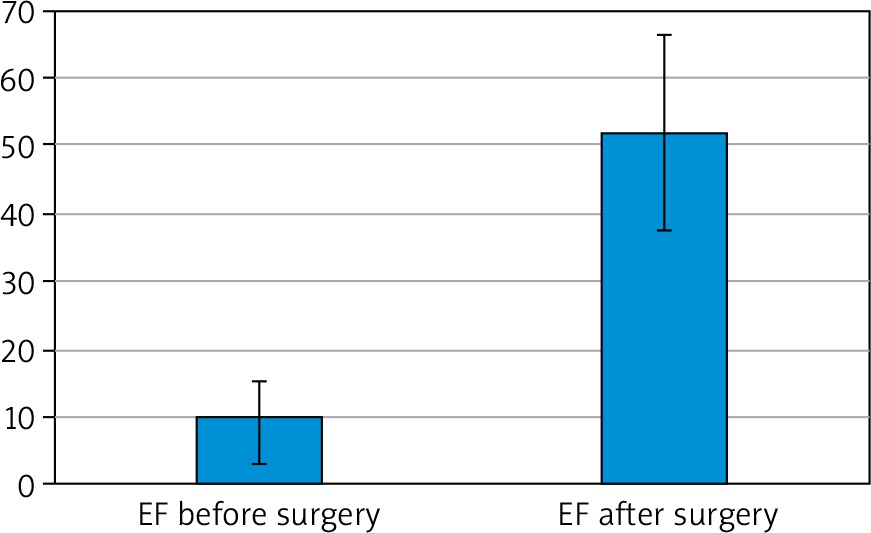
Table IV
Patients’ EF before and after heart transplant
| EF | Mean ± SD | P-value |
|---|---|---|
| Before surgery | 9.59 ±6.15 | 0.0001 |
| After surgery | 52.14 ±14.5 |
Table IV represents extubation times (minimum 3 and maximum 408 hours), duration of admission to the ward (minimum 0 and maximum 17 days) and ICU (minimum 1 and maximum 51 days) (Table V).
Table V
Extubation times and hospitalization duration
| Parameter | Minimum | Maximum |
|---|---|---|
| Extubation time [hours] | 3 | 408 |
| ICU admission duration [days] | 1 | 51 |
| Ward admission duration [days] | 3 | 17 |
Biopsy results showed 6 patients with moderate rejection (grade II), 11 patients with mild rejection (grade I) while 33 patients had no acute rejection (grade 0) (Table VI, Figure 3).
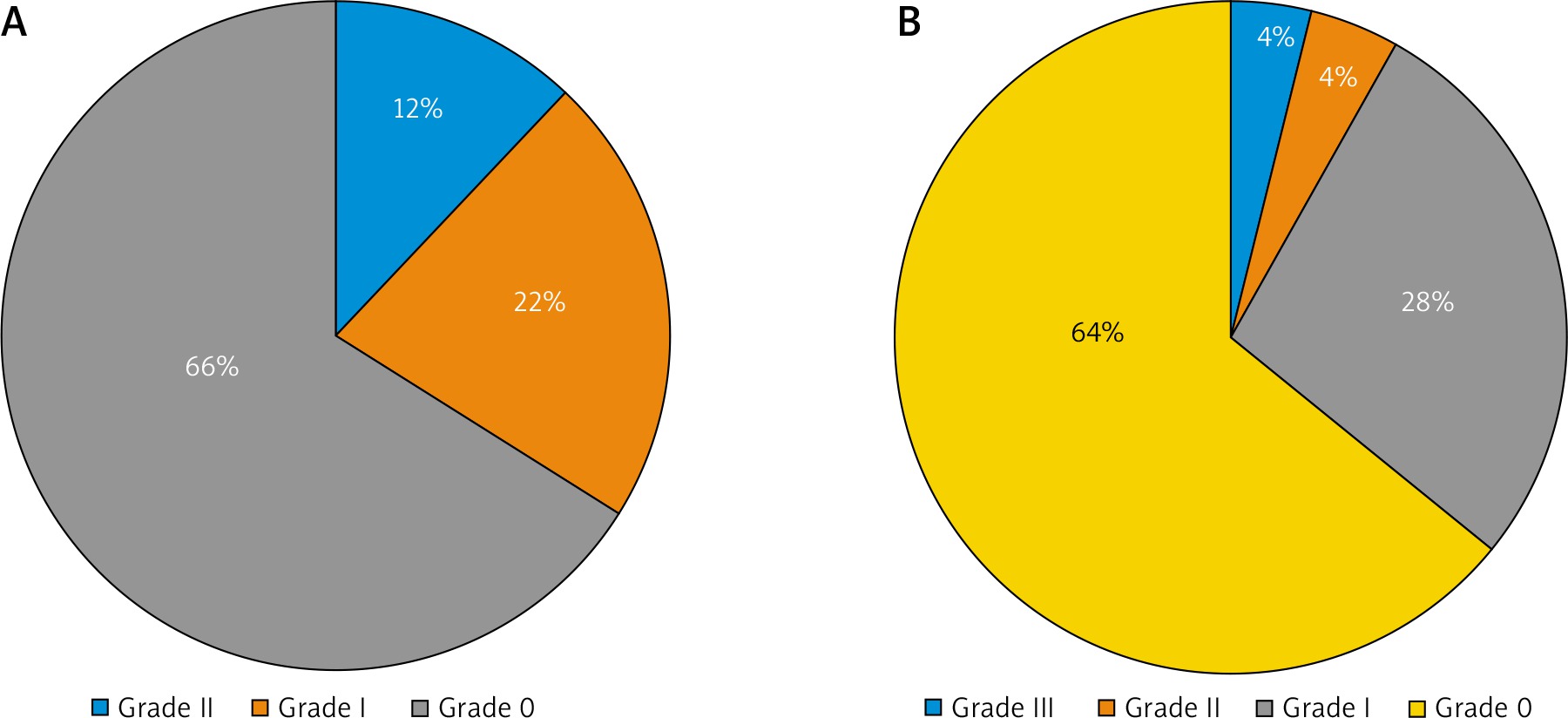
Table VI
Assessment of EMBs following heart transplantation
| Variable | 10 days after surgery | 30 days after surgery | ||
|---|---|---|---|---|
| Frequency | Percentage | Frequency | Percentage | |
| Grade III | 0 | 0 | 2 | 4 |
| Grade II | 6 | 12 | 2 | 4 |
| Grade I | 11 | 22 | 14 | 28 |
| Grade 0 | 33 | 66 | 32 | 64 |
| Total | 50 | 100 | 50 | 100 |
Of 50 heart transplants patients, the number of those who survived was 33 (66%), and of those who died was 17 (34%).
Ischemic times greater than 4 hours have been associated with increased mortality and greater than 6 hours have been considered prohibitive. In our study mean ± SD ischemia time was 57.02 ±15.6 minutes; minimum and maximum were 46 and 551 minutes.
Mean ± SD pump time was 79.3 ±28.6 minutes; minimum and maximum were 46 and 221 minutes.
The follow-up program after heart transplantation showed that 33 (66%) patients survived while 17 (34%) died within 5 years following the surgery (minimum 0, maximum 2160 days with the average of 364.8 days). Causes of death are presented in Table VII.
Discussion
Heart failure can be defined as myocardial inability to provide enough blood flow to other organs in the body including the brain, lungs and kidneys. Heart failure (HF) in chronic kidney disease (CKD) is increasing, and it is necessary to develop optimal strategies for its detection, prevention, diagnosis, and management [11]. Heart failure can be the result of acute or chronic conditions caused by structural or functional abnormalities or a sudden overload. The main clinical hallmarks of heart failure are reduced heart contractility and subsequent pathological remodeling [12]. Cardiomyopathies subtypes include hypertrophic cardiomyopathy (HCM), ischemic cardiomyopathy (ICM), dilated cardiomyopathy (DCM), arrhythmogenic cardiomyopathy and left ventricular (LV) cardiomyopathy [13]. DCM is defined by enlargement and low contractility of the left ventricle (LV) in the absence of ischemic, congenital, valvular conditions or hypertension and is considered a major risk factor for heart failure [14]. ICM is described as the co-presence of heart failure and coronary artery disease [15, 16]. In general, 54% and 45% of patients undergoing heart transplant are suffering from DCM and ICM, respectively [17]. In this regard, we also observed that DCM and ICM were the most common underlying diseases in our transplant patients. A previous study on underlying diseases of patients on the waiting list prior to heart transplantation revealed that patients with RCM, CHID, VCM and HCM are at higher risk of mortality awaiting heart transplant [18]. This report confirms our findings on low prevalence of patients with underlying RCM, CHID, VCM and HCM. Diabetes was another underlying disease which was detected in our patients. It is well accepted that diabetic patients are at higher risk of heart failure due to myocardial damage caused by ischemic or thrombotic conditions [19–22].
EF as an indicator of cardiac function, is an important element in evaluating heart transplantation outcome. A left ventricular ejection fraction of less than 40% is associated with heart failure. The average EF of our patients after heart transplantation reached normal ranges, which shows significant improvement in patient’s quality of life.
A recent UNOS-based study defined the prolonged length of stay (PLOS) in the hospital for patients undergoing heart transplantation as more than 25 days. Patient’s length of stay (LOS) in hospital after heart transplantation depends on different clinical and non-clinical variables. Major risk factors include poor functional status, preoperative mechanical ventilation and extracorporeal membrane oxygenation, renal failure and donor-recipient sex mismatch [23]. Longer LOS correlates with higher mortality and morbidity rates; hopefully the average LOS in our patients was lower than 25 days.
Although heart transplant is considered the gold standard approach for end-stage heart failure patients, organ rejection remains the major challenge in this procedure’s outcome. Donor organ rejection is the result of the recipient’s cellular or humoral immune responses to transplanted heart and may occur as hyper acute (immediate and intraoperative organ rejection), acute (first week up to three months) and chronic (over many years following transplantation) rejection. EMB is one of the most commonly used approaches for diagnosis of acute rejection in patients receiving a heart transplant [24]. Based on our findings, the low incidence of severe acute rejection (4% of patients) within 1 month following heart transplant demonstrates the effectiveness of our immunosuppressive therapy protocol. In the cases of increased mild rejection occurrence (grade I), the patient’s immunosuppressive regimen was re-assessed accordingly. However, due to the limited number of biopsy samplings (10 and 30 days post-operation) in our study, chronic and transient incidents of organ rejection may not have been detected in patients.
A good survival rate of 66% was observed in 5 years following heart transplant in our patients. Main mortality causes in our patients were arrhythmia, intra-operative hemorrhage, hypoglycemic shock and infection. Infection and arrhythmia were the most common causes of mortality. Infection is one of the most frequent causes of mortality in transplant patients, which is mainly due to consumption of immunosuppressive drugs [25–28]. Immunosuppressive therapy of transplant patients is a double-edged sword, in which insufficient administration of suppressant drugs may lead to early organ rejection, while on the other hand, high levels of these drugs can result in infection and malignancies. Two of our patients died from addiction and overdose and one patient died from refusing to take medications following heart transplant, which demonstrates the importance of patient education prior and after heart transplant.
Conclusions
Despite great advances in heart transplant strategies, major challenges remain to be addressed related to patient care, which can significantly affect the therapeutic outcomes. Patient education is an important determinant with a great impact on patient’s survival after receiving the new heart. It is essential that a comprehensive patient education program be established by health care providers prior and after heart transplant, which can clearly describe the importance of patient’s self-care after receiving a new heart and that life-long self-care is as important as the heart transplant itself in the patient’s prognosis. This program should include information regarding the urgency of appropriate drug consumption, attending scheduled checkups and daily repercussions for patients who underwent heart transplantation. Moreover, it is necessary to increase the number and availability of post-transplant health care centers to improve the quality of follow-up programs and patient accessibility.









