
Introduction
Surface 12-lead electrocardiography (ECG) is commonly used in cardiology practice. Besides being a guide in diagnosis and treatment, it is low in cost, noninvasive, and easy to apply. QRS duration (QRSd) is an ECG parameter and shows left and right ventricular depolarization time [1]. The QRSd differs in healthy individuals, and > 120 ms is referred to as wide QRS (wQRS), while ≤ 120 ms is considered as narrow QRS (nQRS) [2]. Many factors affect the duration of QRS, such as left ventricular hypertrophy or dilatation, His-Purkinje conduction defect, left or right bundle branch block, intramyocardial conduction defect, and antiarrhythmic drug use. One of the crucial factors associated with QRS prolongation (↑ QRS) is left ventricular systolic dysfunction [2, 3].
QRS prolongation causes poor cardiovascular outcomes [2, 4–7]. In the left bundle branch block (LBBB), a mortality increase is prominent, but cardiac resynchronization therapy is effective by shortening the QRSd [8, 9]. QRS prolongation is a poor prognostic marker in patients undergoing coronary artery bypass surgery (CABG), as in other cardiovascular diseases [10–12].
In community-based studies, it has been shown that a QRS duration > 110 ms is associated with increased sudden cardiac death, and in those with a fractional shortening below the average value, each increase of 10 ms is an independent predictor of sudden cardiac death [13]. Even in patients with narrow QRS, intermediate QRS prolongation (QRS 90–110 ms) is associated with poor cardiovascular outcomes [14, 15].
Aim
In the current study, we examined the relationship between QRS duration and long-term survival in patients with narrow QRS, who underwent isolated CABG.
Material and methods
The study is a retrospective cohort study. A total of 211 consecutive patients who were admitted to our cardiology clinic between January 2008 and August 2010 and underwent an isolated CABG operation were included in the research. We followed the patients for an average of 110.6 ±16.8 months and identified all-cause mortality as an endpoint. Patients’ death information was obtained from the official national population registration system, and the clinical data were provided through a medical record system. We performed the study under the principles stated in the Declaration of Helsinki. The local ethics committee approved the protocol.
We recorded the patients’ baseline characteristics, laboratory, echocardiographic and ultrasonographic parameters from the routine preoperative assessments. The EuroSCORE calculation was performed using the original score calculation tool available at http://www.euroscore.org/calc.html. We defined preoperative myocardial infarction and chronic obstructive pulmonary disease according to guidelines [16, 17]. Carotid stenosis was evaluated with preoperative carotid Doppler ultrasonography. Body mass index (BMI) was calculated by the weight/height2 formula. The treatment of the patients was arranged according to the coronary artery disease guidelines before the CABG operation.
Preoperative QRSd > 120 ms was defined as wide QRS, and patients with wide QRS were excluded; preoperative QRSd < 120 ms was defined as narrow QRS, and patients with narrow QRS were included in the study. We planned to examine the effect of QRSd on mortality.
Patients with acute or chronic renal failure, history of CABG, or any other cardiovascular surgery, chronic liver disease, malignancy, QRSd > 120 ms, and other than sinus rhythm were excluded from the study. Hospital deaths and patients with unavailable data were not included in the analysis.
Standard transthoracic and Doppler echocardiographic examinations were performed using a 3.25-MHz transthoracic transducer connected to a Vivid 5 System (GE Vingmed Ultrasound AS, Horten, Norway). Two cardiologists, blinded to patients’ data, performed the echocardiography. Left ventricular ejection fraction (LVEF) was calculated with the Simpson method, and other echocardiographic parameters were evaluated according to the American Society of Echocardiography guidelines [18].
Electrocardiography recordings were taken at 50 mm/s and 10 mV/mm amplitude by placing the leads in the standard position. Two expert cardiologists, blinded to patients’ data, evaluated the ECG records, and calculated the most extended QRSd in the leads [19–21].
Statistical analysis
Continuous variables were presented as mean values (standard deviation (SD)) or medians with ranges, and the categorical variables were expressed as percentages. The variables were compared using a 2-tailed Student’s t-test for the continuous variables of a normal distribution or the Mann-Whitney U test for non-normal distribution. The c2 test was used for the categorical variables. The effects of the various variables on all-cause mortality were calculated by univariate Cox regression analysis. In these analyses, the variables with unadjusted p < 0.1 were identified as confounding factors and included in the multivariate regression analyses to determine the independent predictors of all-cause mortality. Factors included in EuroSCORE (age, carotid stenosis, LVEF) were not included in the multivariate analysis. Factors with p < 0.05 in the univariate analysis (EuroSCORE, QRSd, number of coronary arteries with > 50% stenosis, fasting glucose level) were included in the multivariate Cox regression analysis, and the stepwise forward method was used. All the analyses were carried out using SPSS version 16 (SPSS, Inc., Chicago, Illinois).
Results
A total of 211 patients (173 men, 38 women) were followed up to 9.2 ±1.6 years, and 57 (27%) patients died after discharge from the hospital (Table I). When the survivors and non-survivors were compared the mean age (66.4 ±9.2 vs. 59.4 ±8.9 years; p < 0.001), EuroSCORE (4.5 ±2.1 vs. 2.76 ±1.6; p < 0.001), severe carotid stenosis (8 (14.3%) vs. 5 (3.3%); p = 0.007), and number of coronary arteries with stenosis (2.63 ±0.69 vs. 2.45 ±0.68; p = 0.017), were lower; furthermore, QRSd (94.7 ±9.9, 89.1 ±9.7 ms; p < 0.001) and duration of bypass (64.1 ±22.5 vs. 58.3 ±23.2 min; p = 0.047) were shorter in the survivor group. Left ventricular ejection fraction (46.6 ±12.9%, 53.7 ±13.1%; p < 0.001) and hemoglobin levels (13.1 ±1.5, 13.5 ±1.27 g/dl; p = 0.048) were higher in the survival group. Paradoxically, diabetes (19 (33.3%) vs. 75 (48.7%); p = 0.032), insulin/oral antidiabetic usage (16 (28.1%) vs. 70 (45.5%); p = 0.016), and fasting glucose levels (115.9 ±37.5 vs. 138.6 ±63.5 mg/dl; p = 0.016) were higher in the survival group.
Table I
Comparison of demographic data
[i] ACE – angiotensin converting enzyme inhibitor, ARB – angiotensin renin inhibitor, CAD – coronary artery disease, CCB – calcium channel blocker, COPD – chronic obstructive pulmonary disease, HDL – high-density lipoprotein, LIMA – left internal mammary artery, LMCA – left main coronary artery, LVEF – left ventricular ejection fraction, MI – myocardial infarction, NSTEMI – non-ST elevation myocardial infarction, OAD – oral anti-diabetic, WBC – white blood cells.
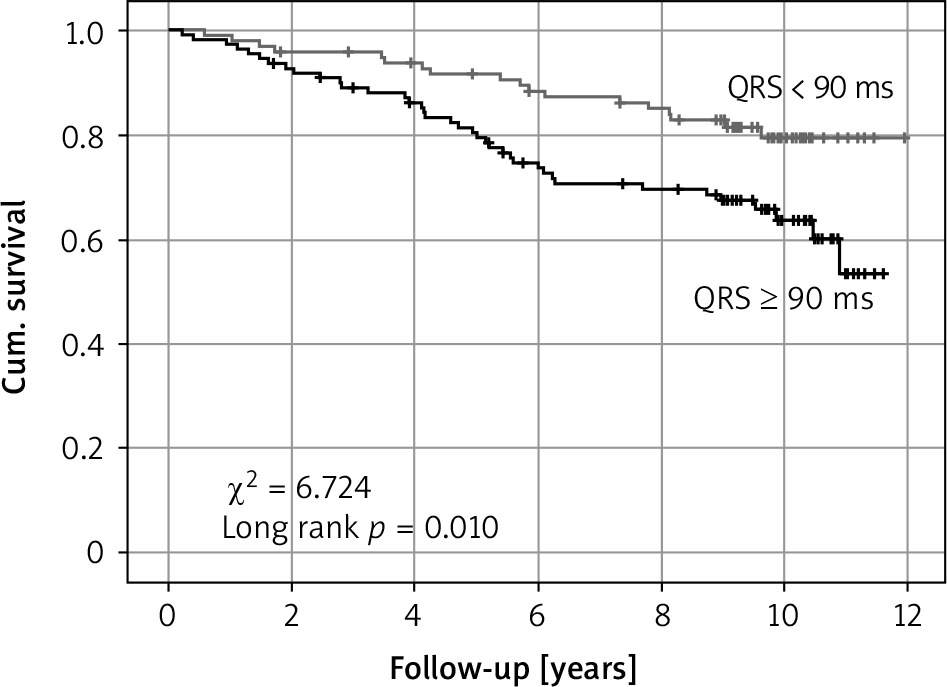
In univariate Cox regression analysis age (OR = 1.076, 95% CI: 1.042–1.110, p < 0.001), EuroSCORE (OR = 1.364, 95% CI: 1.226–1.517, p < 0.001), LVEF (OR = 0.957, 95% CI: 0.937–9.978, p < 0.001), severe carotid stenosis (OR = 1.805, 95% CI: 1.237–2.632, p = 0.002), extent of CAD (OR = 1.694, 95% CI: 1.033–2.776, p = 0.037), QRSd (OR = 1.049; 95% CI: 1.023–1.075, p < 0.001), and fasting glucose levels (OR = 0.994, 95% CI: 0.998-1.000, p = 0.039) were associated with all-cause mortality (Table II). In multivariate Cox regression analysis using the forward stepwise method EuroSCORE (OR = 1.342, 95% CI: 1.167–1.544, p < 0.001), extent of CAD (OR = 1.768, 95% CI: 1.034–3.020, p = 0.037), QRSd (OR = 1.029, 95% CI: 1.002–1.058, p = 0.035) and fasting glucose levels (OR = 0.992, 95% CI: 0.984–0.999, p = 0.029) were independent predictors of all-cause mortality. QRS duration > 89.5 ms determined all-cause mortality with a sensitivity of 73.7% and a specificity of 52% (OR = 2.07) due to ROC analysis. Comparing long-term survival of patients, all-cause mortality was significantly higher in patients with preop QRS duration > 90 ms, from the first year (c2 = 6.724, p = 0.010) (Figure 1).
Table II
Factors predicting mortality (Cox regression analysis)
Discussion
We found that in patients scheduled to have an isolated CABG operation, prolonged QRS, even if it was ≤ 120 ms, was an independent predictor of all-cause mortality over 9 years of follow-up. As QRS was prolonged, survival was significantly reduced at 9.2 years of follow-up.
In the long-term survival study conducted by Ramirez et al., 340 CABG patients were followed for 5 years, and the mortality group had a longer QRSd (100 ms vs. 92 ms; p = 0.021) [10]. Nevertheless, QRSd was not an independent predictor of mortality in multivariate analysis. The mentioned study, which had a shorter follow-up time and different design than our study, determined that QRSd was not an independent predictor of mortality, yet it produced data that support our study.
Gomes et al. determined that QRSd > 114 ms as an independent predictor of cardiac arrest or arrhythmic death in patients with ischemic cardiomyopathy [22]. This finding supported the results of the GUST study [23]. Pudil et al. investigated the prognostic significance of QRSd in 1100 acute myocardial infarction patients [14]. The patients were divided into three groups as < 90 ms, 90–110 ms, > 110 ms, according to the QRS duration on the admission ECG. When the mortality data of 7 days, 30 days, and 1 year were compared, the mortality was significantly higher in the 90–110 ms group than the < 90 ms group (p < 0.001). In addition, in the group with intermediate QRS prolongation, the peak CK-MB level was higher than in the group with QRS duration < 90 ms, and intermediate QRS prolongation was an independent predictor of all-cause mortality in multivariate analysis (OR = 2.21). This research is essential to reveal the clinical significance of QRSd, even if it is a narrow QRS complex. Remarkably, in our study, the preop QRS duration of > 90 ms was the most sensitive and specific marker in determining the long-term prognosis, and there was a significant difference in the long term between the two groups in the Kaplan-Maier survival graph (Figure 1).
Some researchers have revealed that it is clinically significant to have ≥ 100 ms of QRSd without branch block, and defined it as intermediate QRS prolongation. Brilakis et al. reported that intermediate QRS prolongation is an independent predictor of in-hospital mortality in non-ST elevated myocardial infarction (MI) [24]. In a similar study, Tsukahara et al. revealed that ST elevated MI patients undergoing reperfusion had more severe CAD in those with intermediate QRS prolongation [25]. Ilkhanoff et al. evaluated the relationship between cardiac MR imaging, QRSd, and left ventricular (LV) structure in 4591 patients and found that LV volume and mass were higher, and LVEF was lower in patients with QRSd > 100 ms [26]. Additionally, the incidence of heart failure was higher in patients with prolonged QRS in the 7.1 years of follow-up. Similarly, Kurisu et al. reported that intermediate QRS prolongation was positively associated with LV end-diastolic volume and LV end-systolic volume, and was inversely associated with LVEF, in patients with prior anterior MI [27]. Bader et al. stated that QRS prolongation is the most critical predictor of ventricular electromechanical asynchrony, worsening prognosis in heart failure [28]. As a result, for patients with intermediate QRS prolongation, poor LV remodeling is prominent as in wQRS. Thus, intermediate QRS prolongation, clinically and prognostically, seems to mimic the wQRS complex.
Electrocardiography is a cost-effective and practical method that can help to predict sudden cardiac death (SCD) [29]. Increased QRSd is a higher risk for SCD [30]. Implantable cardioverter-defibrillator observational studies and subgroup analyses showed the benefit of narrowing QRS with electrical synchronization [31]. Teodorescu et al. evaluated the effect of prolonged ventricular depolarization and repolarization on the ventricular arrhythmia in CAD patients [32]. They found that 642 SCD cases detected from the general population had an increased QRSd of 8 ms compared to 473 control CAD patients.
The QRSd has a poor prognosis also in preserved LV systolic function. Hummel et al. demonstrated that QRSd is an essential indicator of long-term mortality in patients with preserved left ventricular systolic function hospitalized for heart failure [33]. Joseph et al. reported a similar result [34]. The patients of these studies had the wQRS complex. There are not enough data in the literature related to intermediate QRS prolongation.
In conclusion, for patients undergoing an isolated CABG operation, intermediate prolonged QRS affects prognosis in the long term. The causes are similar to the studies with the wQRS complex. So, in patients undergoing isolated CABG surgery, intermediate prolonged QRS may be a guide in determining long-term increased all-cause mortality risk.
Since the study was retrospective, cardiac death could not be distinguished; therefore, all-cause mortality data could be obtained. The effect of medical treatment on long-term mortality was not evaluated. The number of patients is limited. Only the QRS duration was taken into account in the ECGs of the patients. Fragmented QRS and QRS morphology were not evaluated in the study. Long-term prospective studies may better demonstrate the effectiveness of QRSd measurement, a simple and inexpensive method, in demonstrating long-term risk increases in for patients undergoing CABG surgery.









