








Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) has played a crucial role in the diagnosis and treatment of biliary and pancreatic diseases since it was applied to the clinic in 1968. ERCP-related techniques include endoscopic sphincterotomy (EST), endoscopic papillary balloon dilatation (EPBD), endoscopic nasobiliary drainage (ENBD), endoscopic retrograde pancreatic drainage (ERPD), bile duct or pancreatic duct stent placement, and bile duct or pancreatic duct stone removal. ERCP is more difficult than other endoscopic techniques and has a unique set of complications associated with it that include acute pancreatitis, biliary tract infection, gastrointestinal bleeding, and perforation; some of these are extremely dangerous, such as duodenal perforation [1–3].
Iatrogenic ERCP-related duodenal perforation is a rare and fatal complication of ERCP, and the incidence ranges from 0.29% to 3.5% [4–16], but the highest reported mortality rate is 34.4% [13]. Due to the low incidence and high mortality, there are few large multi-centre cases. The diagnosis, classification, and treatment methods are numerous, and each is reported to have both advantages and disadvantages [17, 18]. In particular, there are different opinions on treatment methods and timing, which bring about many difficulties in clinical treatment.
Perforations during ERCP are caused by endoscopic sphincterotomy, placement of biliary or duodenal stents, issues with the guidewire, and the endoscopy itself. According to the mechanism and location of the perforation, the classification of ERCP-related duodenal perforation is constantly updated [19–21]. Treatment mainly includes endoscopic treatment, surgical treatment, and conservative treatment. In the past, ERCP-related duodenal perforation was mainly treated by surgery [4]. However, in recent years, with the development in endoscopic technology and equipment, more and more cases of endoscopic perforation have been treated by endoscopy [7]. Despite this, the indications of surgical and endoscopic treatment remain unclear, and clinicians do not have a unified standard to select and distinguish surgical patients from endoscopic patients. Furthermore, there is no clear explanation for the timing of treatment, which is another issue that determines the efficacy of treatment.
Therefore, we reviewed the surgical and non-surgical management options for therapeutic ERCP-related perforations; we evaluated the main indications for surgical and non-surgical treatment, as well as the timing of treatment. We aimed to propose a scheme that will help to improve dynamic clinical treatment.
Morbidity and mortality
We retrieved ERCP-related duodenal perforation data from PubMed by reviewing articles reporting more than 10 perforation cases including the terms: “endoscopic retrograde cholangiopancreatography” or “ERCP” combined with “duodenal perforation” in the past 5 years. No other restrictions were imposed. Thirteen of these articles described the incidence of perforations; the incidence rate is 0.8% (0.29–3.5%) (Table I). The overall trend has not changed much from the previously reported 0.6% incidence rate [2], and the more cases studied, the lower the incidence rate. In total, 11 articles described the association of sex with perforation, and demonstrated that perforation is predominantly found in females (70.2%; range: 50–90%) although the reason for this remains unknown. Of the retrieved articles, 12 included age descriptions, with an average patient age of 66.2 years (46–75.7 years). In total, 11 articles showed an average case mortality rate of 6.3% (1.7–34.4%), an average surgical rate of 20.5% (3.4–78%), and an average operative mortality rate of 23% (0–50%).
Table I
List of major studies
| Time of article published | Number of patients having ERCP | Number of patients with ERCP perforation (%) | Number of female perforation (%) | Average age [years] | Mortality (%) | Surgery ratio (%) | Surgery mortality rate (%) |
|---|---|---|---|---|---|---|---|
| 2020 [4] | 25300 | 380 (1.5) | 16 (4.2) | 50 (13.2) | 16 (32) | ||
| 2019 [5] | 19468 | 58 (0.29) | 36 (62) | 68.5 | 1 (1.7) | 2 (3.4) | 1 (50) |
| 2019 [6] | 342 | 12 (3.5) | 7 (58) | 75.7 | |||
| 2018 [7] | 4196 | 28 (0.67) | 14 (50) | 71.3 | 1 (3.57) | 6 (21.4) | 1 (16.7) |
| 2018 [8] | 4513 | 36 (0.79) | 25 (69) | 72.02 | 4 (11.1) | 28 (78) | 2 (7.1) |
| 2018 [9] | 7249 | 35 (0.48) | 26 (74) | 59 | 1 (2.86) | 2 (5.7) | 0 |
| 2018 [10] | 3492 | 16 (0.4) | 12 (60) | 46 | 1 (5) | 5 (25) | 1 (20) |
| 2017 [11] | 6934 | 37 (0.53) | 25 (67) | 70 | 4 (10.8) | 8 (22) | 1 (12.5) |
| 2017 [12] | 2423 | 21 (0.9) | 11 (52) | 69.7 | 1 (4.8) | 4 (19) | 1 (25) |
| 2016 [13] | 9383 | 29 (0.33) | 18 (62) | 70.5 | 10 (34.4) | 15 (51.7) | 7 (46.6) |
| 2016 [14] | 3331 | 79 (2.37) | 71 (90) | 61 | |||
| 2015 [15] | 4600 | 23(0.5) | 66.7 | 1 (4.3) | 11 (47.8) | 0 | |
| 2015 [16] | 1923 | 15(0.78) | 12 (80) | 68.5 | 3 (20) | 8 (53) | 2 (25) |
| In total | 93154 | 769(0.8) | 257 (70.2) | 66.196 | 43 (6.3%) | 139 (20.5) | 32 (23) |
Risk factors
It was demonstrated that 15 factors increase duodenal perforation in ERCP, including senility, suspected sphincter of Oddi dysfunction (SOD), biliary stricture dilation, papillary stenosis, Billroth II reconstruction, presurgical sphincterotomy, stent-related issues, difficult canulation, unskilled surgeons, hypertension, and long operation time [8, 15] (Table II). Studies showed that SOD was a major risk factor for Stapfer II perforation. Hypertension is a new risk factor [11]. The other factors reported by different medical institution centres are different. Studies from six referral centres in Korea suggested that 37.3% of perforations were associated with sphincter cuts, about 28.9% were related to papilla pre-cut, and 25.4% were related to papilla balloon dilatation [17]. Patil et al. [4] also reported that 30% of patients with perforations had a history of difficult canulation, 20% had a pre-cut history, and 8% had a history of papillary incision. The new study of Niu et al. [3] showed that senility did not increase the risk of perforation.
Table II
List of risk factors of iatrogenic duodenal perforations during endoscopic retrograde cholangiopancreatography
Classification of ERCP-related duodenal perforation
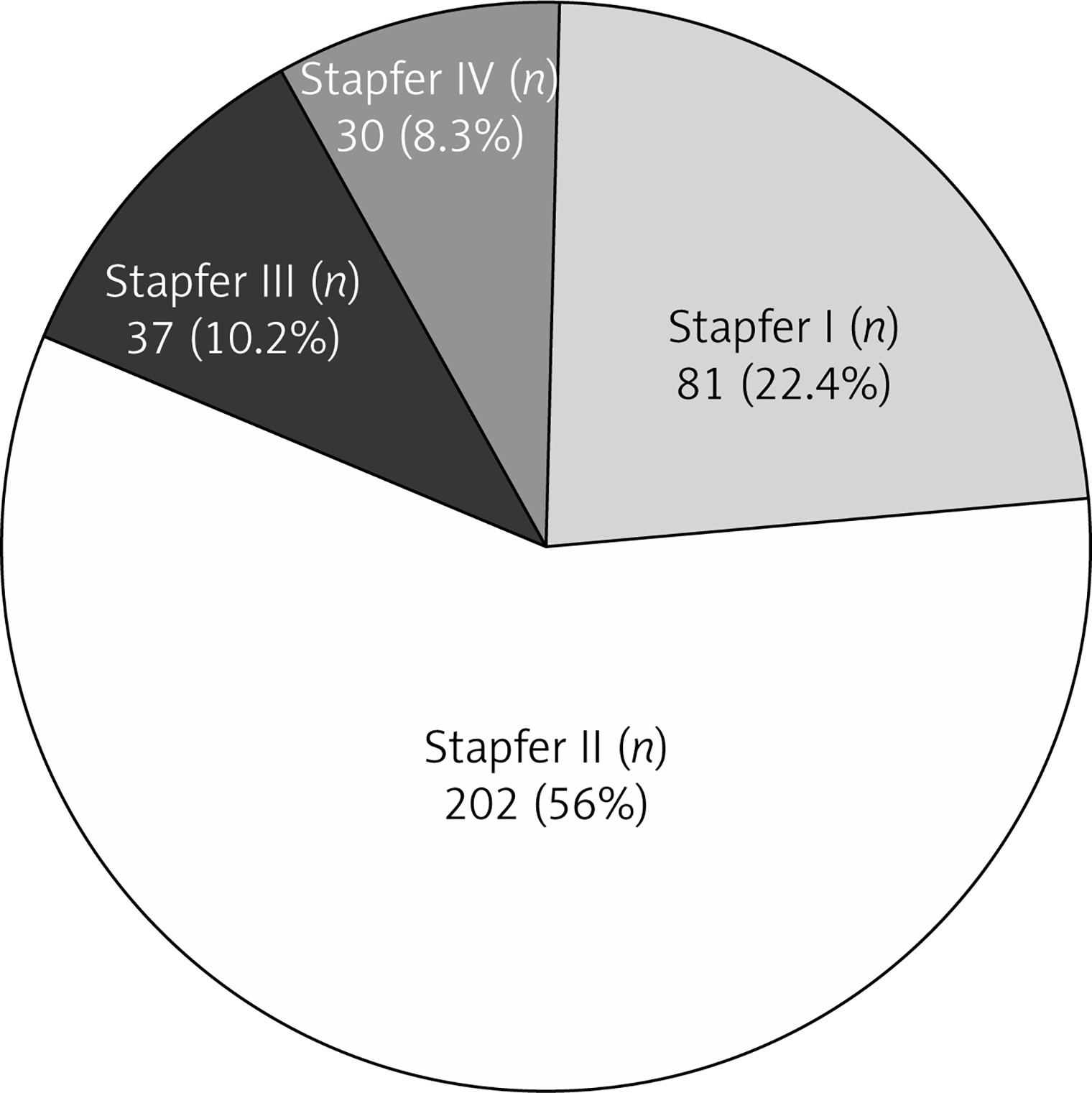
According to the mechanism and location of previous perforations, there were four types of ERCP-related duodenal perforations (Table III). Firstly, in 2000, Stapfer et al. [19] classified perforations into four categories (Stapfer I, II, III, and IV). This represents a classic classification that is widely recognised. The location and severity of the perforation were clarified and treatment methods were proposed, but it is difficult to distinguish these four types of perforation in clinical practice. Subsequently, Howard et al. [20], Enns et al. [21], and Kim et al. [22] classified perforations in a variety of ways according to the location of the perforation and the device that caused the perforation, but all have problems similar to the Stapfer classification. Because the perforation detection rate of ERCP intraoperative diagnosis is only 23.3%, and because of bleeding and infection after ERCP, it is more difficult to distinguish the location and type of perforation, which limits the clinical usefulness of these classifications; thus, a better classification is required [16]. In recent years, three new classifications have emerged (Table IV). Miłek et al. [18] preferred a classification treatment based on intraperitoneal and extraperitoneal perforation, while Bray et al. [12] and Wu et al. [23] proposed a classification based on computed tomography (CT) scan. The Wu et al. [23] classification divides patients into air-alone, air-fluid, and fluid-alone groups. This method is a good supplement, especially when the Stapfer classification cannot be used after ERCP, and it can also distinguish the severity of perforation. It may become an important classification method to distinguish non-surgical patients in the future. At present, the typing method proposed by Stapfer is used at home and abroad, and Stapfer II is the most common in the clinic (Figure 1). The high incidence of Stapfer II is related to more clinical canulation difficulties and papilla pre-cutting operations.
Table III
Previous classification of iatrogenic duodenal perforations during endoscopic retrograde cholangiopancreatography
| Type | Stapfer et al. [19] | Howard et al. [20] | Enns et al. [21] | Kim et al. [22] |
|---|---|---|---|---|
| I | Lateral or medial duodenal wall perforation, endoscope related | Guidewire perforation | Oesophageal, gastric, and duodenal perforation | Scope itself |
| II | Periampullary perforations, sphincterotomy related | Periampullary perforation | Periampullary perforation | Needle knife used during the sphincterotomy |
| III | Ductal or duodenal perforations due to endoscopic instruments | Duodenal perforation | Guidewire-related perforation | Guidewire and is associated with the least risk of contamination |
| IV | Guidewire-related perforation with presence of retroperitoneal air at X-ray | None | None | None |
Table IV
New classification of iatrogenic duodenal perforations during endoscopic retrograde cholangiopancreatography
| Type | Miłek et al. [18] | Bray et al. [12] | Wu et al. [23] |
|---|---|---|---|
| I | Extraperitoneal (Duodenum except for duodenal bulb) Common bile duct Ampulla of Vater | Retroperitoneal contrast identified during ERCP | Air-alone groups |
| II | Intraperitoneal Duodenal bulb | Retroperitoneal air on subsequent imaging | Air-fluid groups |
| III | None | Retroperitoneal fluid on subsequent imaging | Fluid-alone groups |
| IV | None | Intraperitoneal air or fluid | None |
Diagnosis of ERCP-related duodenal perforation
Mortality can be reduced by early diagnosis and early appropriate interventions. The diagnosis rate varies greatly in different literature. Intraoperative diagnosis of ERCP-related duodenal perforation can identify the type of perforation and process it immediately; however, the diagnosis rate (8.4–100%) needs to be improved [4, 5, 16, 17, 24]. The conscious training of doctors before ERCP, the comparison of patients undergoing preoperative X-ray examination, and X-ray or fluorescence examination during and after ERCP can greatly improve the diagnosis rate of perforation [25]. The amount of retroperitoneal air may be independent of the size of the perforation, but rather the endoscope blows in the air during ERCP. The degree is related, and it is best to mirror carbon dioxide, which is capable of rapid absorption and high contrast [14].
Treatment
In recent years, endoscopic treatment ERCP-related perforations have gradually replaced surgery. Especially with the rapid development of endoscopic treatment methods and equipment, Endoclips, Endoloops, the over-the-scope clip system (OTSC), fully covered self-expandable metallic stents (FC-SEMS), and fibrin sealants have been successfully applied. These advances not only make endoscopic treatment safe and feasible, but also shorten the length of hospital stay, reduce the cost, and reduce the trauma and complications caused by surgery [26–30]. However, in certain cases surgery still needs to be considered. Conservative therapy is the basis of treatment and needs to be used in most patients.
Timing of treatment
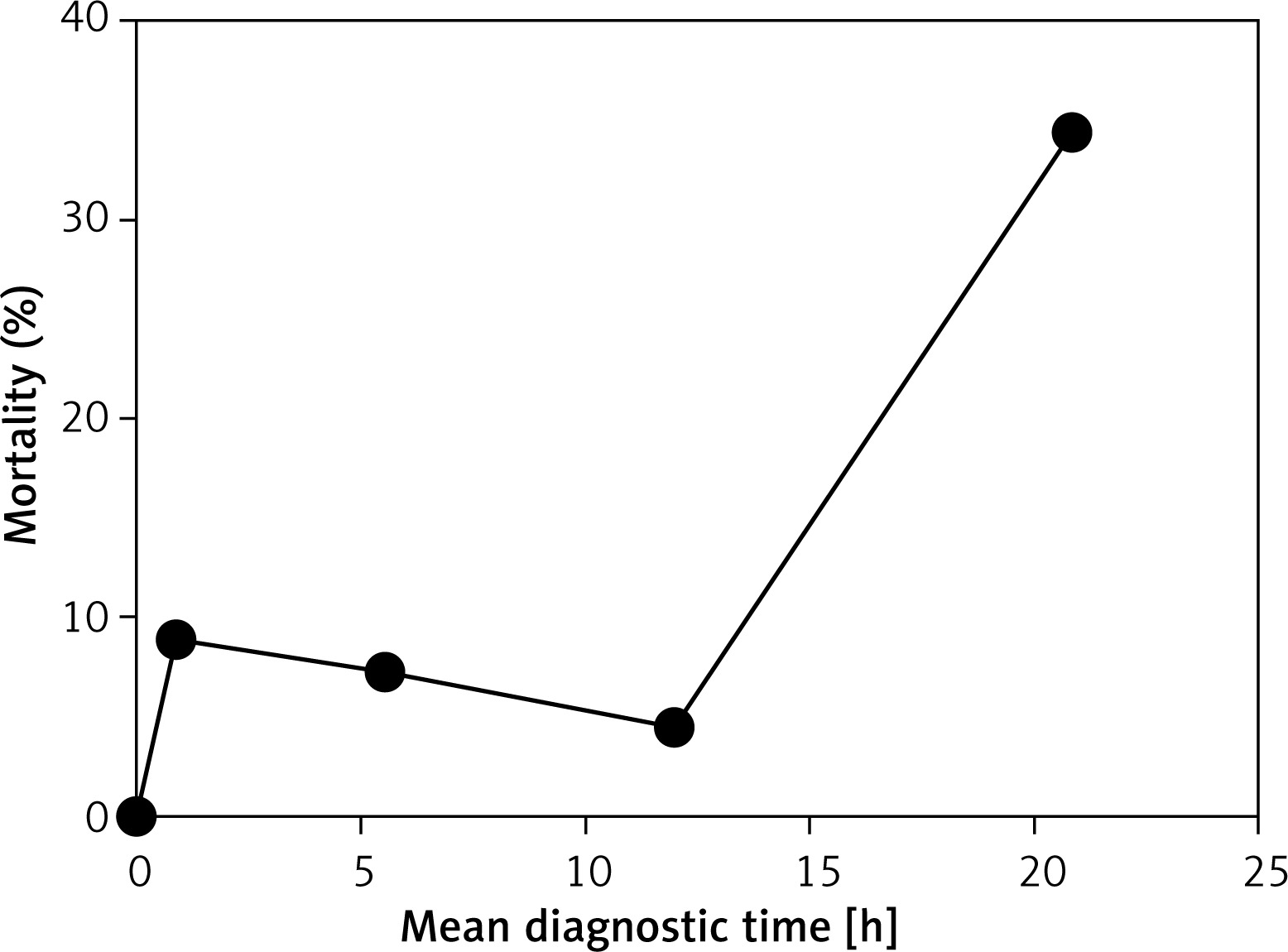
The treatment and prognosis of ERCP-related duodenal perforation are closely related to time (Figure 2), which is also an important factor in determining the most appropriate treatment. A particular emphasis is placed on early diagnosis and early differentiation between surgical and non-surgical cases, and delayed surgery can greatly increase mortality. However, the definition of ‘early’ is unclear. It is reported that the intervention time is mainly during ERCP and 12 h, 24 h, 72 h after ERCP [5, 7, 13, 24]. First, delays greater than 72 h were generally not controversial because the prognosis was poor [13, 16]. Secondly, several studies have demonstrated that an abdominal scan before ERCP, especially a computed tomography (CT) scan, will greatly improve the intraoperative diagnosis rate of ERCP-related duodenal perforation. If the perforation is found during surgery and directly treated by endoscopic methods, the postoperative complications and mortality will be reduced. Indeed, this is the best time to treat; even if the endoscopic treatment fails, early surgery can be performed and the prognosis is better [5, 7, 14]. Finally, some studies have shown that the mortality rate within 12 h of diagnosis and treatment was within 10%, and the difference between surgery and endoscopic treatment was small [10, 11, 15, 17, 24]. The mortality rate increased after 24 h, and the surgical mortality rate could be as high as 50% [4, 5, 13, 16, 18]. At the same time, it is worth noting that there are studies that suggest a 12-hour diagnosis, with a total mortality rate of 4.3% and zero surgical mortality [15]. Therefore, early diagnosis and treatment recommendations are considered to be most effective within 12 h and no later than 24 h.
Endoscopic indications
With the development of endoscopic techniques, reports of endoscopic treatment perforations have increased in recent years. Most reports suggest that perforation should be directly treated by ERCP if the perforation is found during ERCP. For example, Shi et al. [5] reported the successful treatment of Stapfer I, Stapfer II, as well as perforation of the duodenum horizontal, large perforation with endoscopy [5, 8]. All were previously recommended for surgery. This suggested that the size and type of perforation was no longer the main factor in distinguishing surgical and non-surgical patients. Simultaneous endoscopic treatment is also feasible after perforation of ERCP. Indeed, surgical and endoscopic comparison results by Artifon et al. [15] also showed that within 12 h of ERCP, the success rate of endoscopic and surgical treatment was 100% regardless of the size and type of perforation. Jin et al. [17] considered that there was no systemic inflammatory response (SIS) or peritonitis (PIS) in perforation, and thus no preferred endoscopic treatment. Kumbhari et al. [14] proved that SIS was no longer a surgical indication. Therefore, time may be important to distinguish endoscopic patients. The perforations found during ERCP can be treated directly under the endoscope. For postoperative perforation, endoscopic closure can be attempted within 24 h, and especially within 12 h, but PIS needs to be ruled out.
Endoscopic modes
It was demonstrated that 14 endoscopic methods treat perforations (Table V, Figure 3). There is no unified standard for the selection of methods. We have described them briefly based on the initial closure and reclosure. Jimenez Cubedo et al. [8] reported the first closure of a human duodenal perforation using an endoscope. First, for the initial closure of the perforation, especially the perforation found in the endoscope, an initial closure can be performed using an endoscopic clip and an endoscopic ring, an endoscopic clip and an annulus, OTSC, and an under cap-assisted endoscopy [5, 24, 25, 28]. For small perforations (< 1 cm), a single endoscope clip is sufficient. For larger perforations (> 1 cm), it is best to combine Endoloops and Endoclips, double endoscopic band ligation and Endoclipping, and multiple endoscopic devices [31, 32]. In double lumen endoscopically, a plurality of titanium clips should be used to secure the snare to the perforated edge before tightening the snare. The device is then closed to the perforation (3 cm). When the perforation of the duodenal bulb is initially closed, it is better to perform endoscopic titanium clip closure. For perforations that occur at the junction of the duodenal bulb and descending part, due to the acute angle of the anatomical structure, the use of a front-view ERCPscopy with a transparent cap during using titanium clamps to close this perforation can provide a good field of view and can effectively clamp the perforation [28]. If a duodenoscope is used, the difficulty of surgery will increase.
Table V
Characteristics of perforation and corresponding endoscopic treatment methods
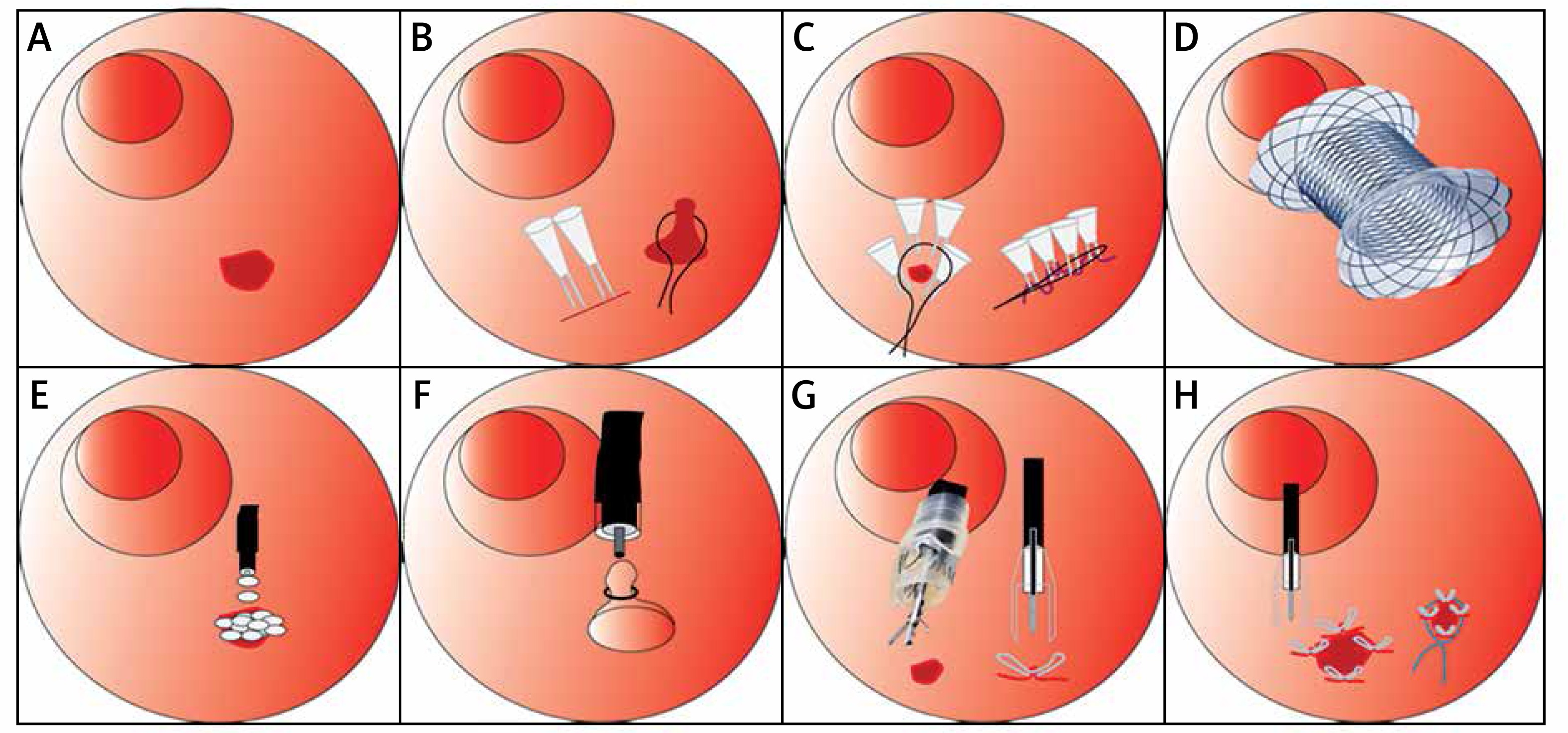
Figure 3
Therapeutic diagram of endoscopic closing duodenal perforations. A – Endoscopic retrograde cholangiopancreatography (ERCP)-related duodenal perforations. B – Endoclips and Endoloops. C – Pursestring suture. D – Fully covered self-expandable metallic stent (FC-SEMS). E – Fibrin glue. F – Endoscopic band ligation (EBL). G – Over-the-scope clip (OTSC). H – Tulip bundle
Drainage is important for prognosis when treating perforation. Immediate placement of metallic Endoclips, covered metal stent, self-expandable metallic stents (SEMS), and fully covered self-expandable metal stents (FC-SEMS) can close perforations more effectively [29, 30]. This can reduce peritonitis and shorten hospital stays by reducing patient pain and white blood cell counts. In particular, FC-SEMS has been widely reported in recent years for the treatment of Stapfer II perforations. Reports showed that FC-SEMS played a role not only in biliary drainage but also in sealing perforations. Since the FC-SEMS may block the perforated area by radial force, the perforated area can heal quickly [5].
Endoscopic fibrin sealant and tulip bundle rescue can be used to close a failed perforation for the first time [22, 27, 31]. Fibrin is an adhesive that contains fibrinogen and thrombin, which can promote tissue repair for up to 2 weeks and can be absorbed by both macrophages and fibroblasts. In cases of endoscopy failure due to insufficient titanium clamp closure, it is also conceivable to use fibrin adhesive alone. For perforation located in the retroperitoneum, retroperitoneal tissue prevents fibrin adhesives from working, and the diffusion effectively seals the perforations. The tulip bundle was used for closure after failure was reported for the first time. Zimmer et al. [33] reported that “tulip bundled rescue” could be used for Stapfer I perforation that OTSC failed to treat.
Endoscopic nasobiliary drainage (ENBD) and endoscopic retrograde biliary drainage (ERBD) can be used alongside adjuvant treatment at the same time. Loske et al. [30] reported endoscopic vacuum therapy with a novel open-pore film drainage (OFD) treatment for perforation. These methods can be used for both small and large perforation-assisted treatment.
Surgical indications
In the past, ERCP complicated duodenal perforation advocated surgical treatment. However, with the results of endoscopic treatment, many indications have changed. Changes in surgical indications are mainly based on classification, clinical symptoms and signs, and the severity of the disease. Firstly, Stapfer I, Howard III, and Enns III perforations are classified as large perforations, and surgery was recommended performed immediately in the past [14, 19–21]. But now Shi et al. [5] disagree because they successfully treated Stapfer I perforations with endoscopy. Secondly, the surgery is sometimes determined based on imaging data. Indeed, Rabie et al. [34] believe that liquid on the CT is an indication for surgery. They proposed three surgical hard signs: contrast agent extravasation, ascites, and intra-abdominal air, as well as a series of soft signs: duodenal wall thickening, air in the duodenal wall, and retroperitoneal air. If the diagnosis is conservative within 24 h, without improvement or worsening, the abdomen should be opened [18]; another angle is the general vital signs and symptoms. Koc et al. [35] suggest that surgery should be performed if the systolic blood pressure is lower than 90 mm Hg, heart rate is higher than 120 beats/min, and the body temperature is greater than 38°C. Moreover, obvious symptoms of abdominal pain are planned indications for surgery. Jin et al. [17] suggested that the mortality of ERCP-related duodenal perforation is associated with peritoneal irritation (PIS) and the systemic inflammatory response (SIS), and they advised that surgery should be performed promptly following the appearance of these two symptoms. In summary, almost all researchers believed that sepsis is an indication for immediate surgical intervention; these are common signs, but some are not particularly common. A study of surgery and endoscopic treatment by Patil et al. [4] found that high total leukocyte count (TLC) and hypoalbuminaemia occurred 12 h after ERCP, and non-surgical treatment was prone to failure, which was an indication for planned surgery. Furthermore, Kumbhari et al. [14] reported the relationship between perforation size and surgery and found that most patients with a perforation diameter greater than 1 cm underwent surgical treatment. Also, many recent studies have proposed that patients should be comprehensively managed, rather than focusing on a certain clinical manifestation. Theopistos et al. [7] stated that a plan should be formulated based on the patient’s diagnosis time, clinical symptoms, and disease progression [15]. The clear clinical symptoms are abdominal tenderness, rebound tenderness, and muscle tension. Moreover, imaging findings have suggested that CT or ERCP massive contrast agent exudation, CT-enhanced scan that confirms large intra-abdominal or retroperitoneal effusion, huge subcutaneous emphysema, unrelieved biliary obstruction, and foreign bodies in the bile duct that fail to be expelled are representative of cases that require immediate surgery. In addition, a number of researchers have identified non-surgical indications. Tavusbay et al. [13], Stapfer et al. [19], and Kim et al. [22] have indicated that simple retroperitoneal air should not be used as an indication for surgery [8, 19]; therefore, the consideration of Theopistos et al. [7] may be better for the clinic. If PIS occurs, radiologically persistent leaks and vital signs are unstable, surgical intervention may be better within 24 h of ERCP but is not recommended after 72 h.
Surgical methods
The surgical interventions commonly used to treat ERCP-related perforations include duodenal suture, retinal patch repair, pyloric exclusion, gastrointestinal anastomosis, and T-tube drainage with or without cholecystectomy [17, 19, 20]. Koc et al. [35] also reported extensive surgical procedures for the treatment of ERCP-related perforations, including the following: simple retroperitoneal drainage; insertion of a perforated T-tube for duodenal repair; common bile duct exploration and T-tube placement; duodenal resection and gastric jejunum anastomosis or gastrojejunostomy; pyloric exclusion and pancreaticoduodenectomy; laparoscopic cholecystectomy (LC) + common bile duct exploration (LCBDE) + T-tube + intra-abdominal and/or retroperitoneal drainage; biliary exploration; and biliary derivation [8, 35]. Surgery is associated with many factors, including underlying disease, and the size and location of the perforation. In patients with perforation due to problems such as papilla incision or biliary stenosis, bile duct exploration, duodenal repair, T-tube drainage, and jejunostomy are required. In cases where the perforation of the intestinal wall is large, due to technical inexperience and side view angle problems, further perforation repair is needed. For the perforation of the intestinal wall far away from the duodenal papilla, usually due to a large perforation and a short endoscope, simple duodenal suture is not ideal, and gastrointestinal anastomosis and ostomy are required. The most common surgical method is a simple duodenal suture with or without omental fixation (93.7%) [2].
Conservative treatment
The consensus is that ERCP patients need intestinal rest, parenteral nutrition, intravenous and/or oral antibiotics during perforation treatment, and the symptomatic use of proton pump inhibitors and somatostatin to maintain the stability of the internal environment [5, 13, 15, 24]. If the perforation is small, or if it is only retroperitoneal air, the patient can be treated with medication alone. If retroperitoneal or peritoneal effusion is present, percutaneous drainage is performed under CT guidance [23]. In specific drug treatment, research by Bray et al. [12] showed that early antibiotic use is beneficial for prognosis.
Prevention strategy
Because some patients are prone to ERCP-related perforations, the risk factors of ERCP-related perforation should be considered, and measures should be taken to prevent the occurrence of perforation as much as possible.
Prevention of patient-related risk factors
First, for patients with gastrointestinal reconstruction involving the duodenum, and patients with biliary and pancreatic tumours, the application of duodenoscopy to ERCP can easily cause bowel perforation; the choice of a front-view ERCPscopy can reduce this risk of perforation. Secondly, there is a risk of perforation when there is a diverticulum or diverticulum papilla adjacent to the duodenal papilla [36]; to avoid this, a small incision + balloon dilation or a simple balloon dilation can be performed.
Prevention of operation-related risk factors
First, duodenal papillary incision is performed in cases with difficult canulation. Although the risk of perforation is high, the use of new instruments, such as the DUAL knife, can reduce this risk. Second, the use of larger diameter balloons to dilate the duodenal papilla, or the presence of bile duct stenosis, carries a high risk of perforation, so the use of excessively large diameter balloons for dilation should be avoided. Third, the risk of perforating the duodenal papillectomy is high, and the indications for this operation should be carefully considered. If a longer stent needs to be placed, using another type of stent (dual pigtail type) may prevent perforation [11]. Moreover, it is necessary to perform the surgery carefully and to try to operate under X-ray surveillance. During the operation, close attention should be paid to the X-ray fluoroscopy image, and signs of perforation should be found early to facilitate early treatment [25].
Discussion
Our review of ERCP-related duodenal perforation suggests that perforation related to ERCP is inevitable, and identified risk factors that can improve prognosis [2]. Mortality can be reduced by early diagnosis and early appropriate interventions. The classification of perforation is mainly based on the mechanism, location, and treatment. There are seven main classifications, of which the first four have been mentioned in previous literature [19, 22]. The latter three categories are classified according to videography location and severity and were not covered in previous literature. Compared to other classifications, Stapfer classification is detailed and reasonable, but it was difficult to use in clinical practice. The Wu et al. [23] method is a good supplement, especially when the Stapfer classification cannot be used after ERCP, and it can also distinguish the severity of perforation. It may become an important classification method to distinguish non-surgical patients in the future.
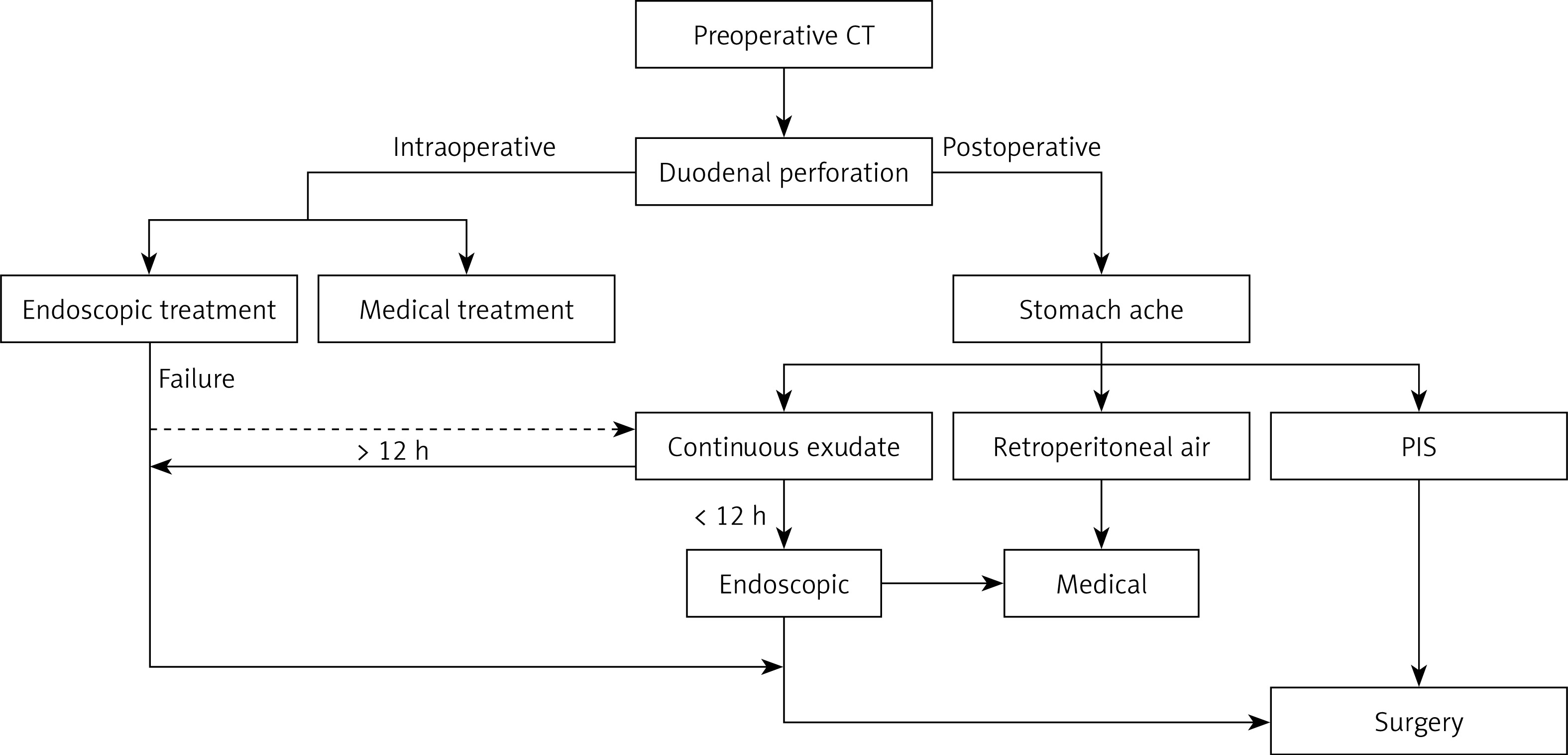
In the past, the treatment of ERCP-related perforation was mainly surgical. However, in recent years, with the development of endoscopic treatment technology, many cases that were previously considered to require surgical treatment have been successfully treated by non-surgical means. Our systematic review also suggests that a non-surgical approach is feasible [28]. Endoscopic treatment has advantages in mortality, hospital stay, and complications. In particular, the combined application of multiple endoscopic devices, such as Endoclips, Endoloops, and OTSC, has led to the successful treatment of many large perforations, which can be successfully treated by endoscopic stent implantation, even if accompanied by massive exudation [29, 36, 37]. The majority studies also have suggested that obvious and continuous abdominal pain, as well as continuous fluid or contrast agent leakage under CT or ERCP, are operative hard indications. Early leakage can be treated with endoscopy, but surgical treatment is recommended because surgery that is delayed more than 24 h greatly increases mortality [16]. Retroperitoneal air is no longer an indication for surgery. Surgical and endoscopic interventions are closely related to the timing of treatment. Endoscopic treatment can be successfully performed early (less than 24 h), excluding cases with hard indications, especially for perforations within 12 h. Furthermore, surgical treatment can be continued even if endoscopic treatment is unsuccessful. Therefore, we proposed a simple algorithm such as that outlined in Figure 4, to provide some suggestions for clinical, especially endoscopic treatment.
Figure 4
Algorithm of the management of endoscopic retrograde cholangiopancreatography (ERCP)-related duodenal perforations
PIS – peritonitis.
Recent advances in ERCP endoscopic treatment related to duodenal perforation are exciting, primarily in the early (< 12 h) and early diagnosis of patients with advanced equipment and expert use of endoscopes, endoscopic clips, endoscopic suturing device, fibrin sealant, and SEMS insertion. This has benefited many patients. However, based on the complexity of the clinical status of the perforation, there is currently no clear consensus on the best treatment regimen that can be used in all cases. In the future, more comparisons between prospective trials between endoscopy and surgery and new methods of endoscopy may be needed. The current view has a number of limitations. Although the quality of the included papers is good and the numbers of cases are relatively large, they also include many new endoscopic treatments. Furthermore, there are fewer cases, especially the comparison between endoscopy and surgery, and there is only one randomisation.
Conclusions
Although duodenal perforation after ERCP is uncommon, if it is not treated adequately and promptly, it can cause serious complications. In particular, in elderly women at high risk, preoperative evaluation by abdominal scan is necessary. Preoperative scanning and careful observation during ERCP can greatly improve the intraoperative diagnosis rate. Once perforation is found in ERCP, endoscopic treatment can be performed regardless of the size of the aperture, as can a combination, and repeated application, of multiple endoscopic techniques. There is also the question of surgical intervention. Surgical treatment has decreased in recent years. However, since delayed surgery can greatly increase mortality, experienced surgeons should be consulted at the same time as conservative treatments are administered. Surgery remains necessary once a perforation continues to exfoliate, or in cases with severe peritonitis and sepsis. Above all, non-surgical treatment is feasible if the perforation is noted early and management of the perforation and peritoneal contamination is minor. Even in cases with fluid leakage, it is possible to treat by drainage and decompression; however, once there is a continuous large amount of exudate and severe peritonitis, or even sepsis, surgery is still preferred.