Introduction
The application of retroperitoneoscopy in the pediatric urology patient was delayed compared to the adult population. The smaller working space compared to transperitoneal laparoscopy, combined with reversed orientation of the kidney hilus, makes retroperitoneoscopy hard to master. Thus, retroperitoneoscopy is mostly performed in children with benign disease [1–5]. Few studies have concerned the advantages of retroperitoneoscopy in children, especially in the treatment of pediatric oncological patients. In this study, we describe a series of resection operations under retroperitoneoscopy in children to demonstrate its safety and efficacy in the management of nonfunctioning or poorly functioning kidney–kidney cyst, renal carcinoma, adrenocortical carcinoma–adrenal ganglioneuroblastoma–adrenal teratoma, neuroblastoma, Wilms’ tumor, and adrenal hemangioma.
Aim
We describe our experience in a series of resection operations under retroperitoneoscopy to demonstrate that the retroperitoneoscopic resection operation of a renal or adrenal specimen is feasible and safe in children, not only for benign disease but also in oncological patients.
Material and methods
Patients and data collection
We retrospectively reviewed 18 consecutive patients on whom retroperitoneoscopy was carried out by one pediatric urologist from December 2017 to July 2019. The data on clinical parameters such as gender, age, operative time, mass diameter and hospitalization duration were collected. To compare the differences between retroperitoneoscopy and transperitoneal laparoscopy in the treatment of oncological patients, clinical parameters of 13 consecutive patients who underwent transperitoneal laparoscopy were collected.
Operative technique
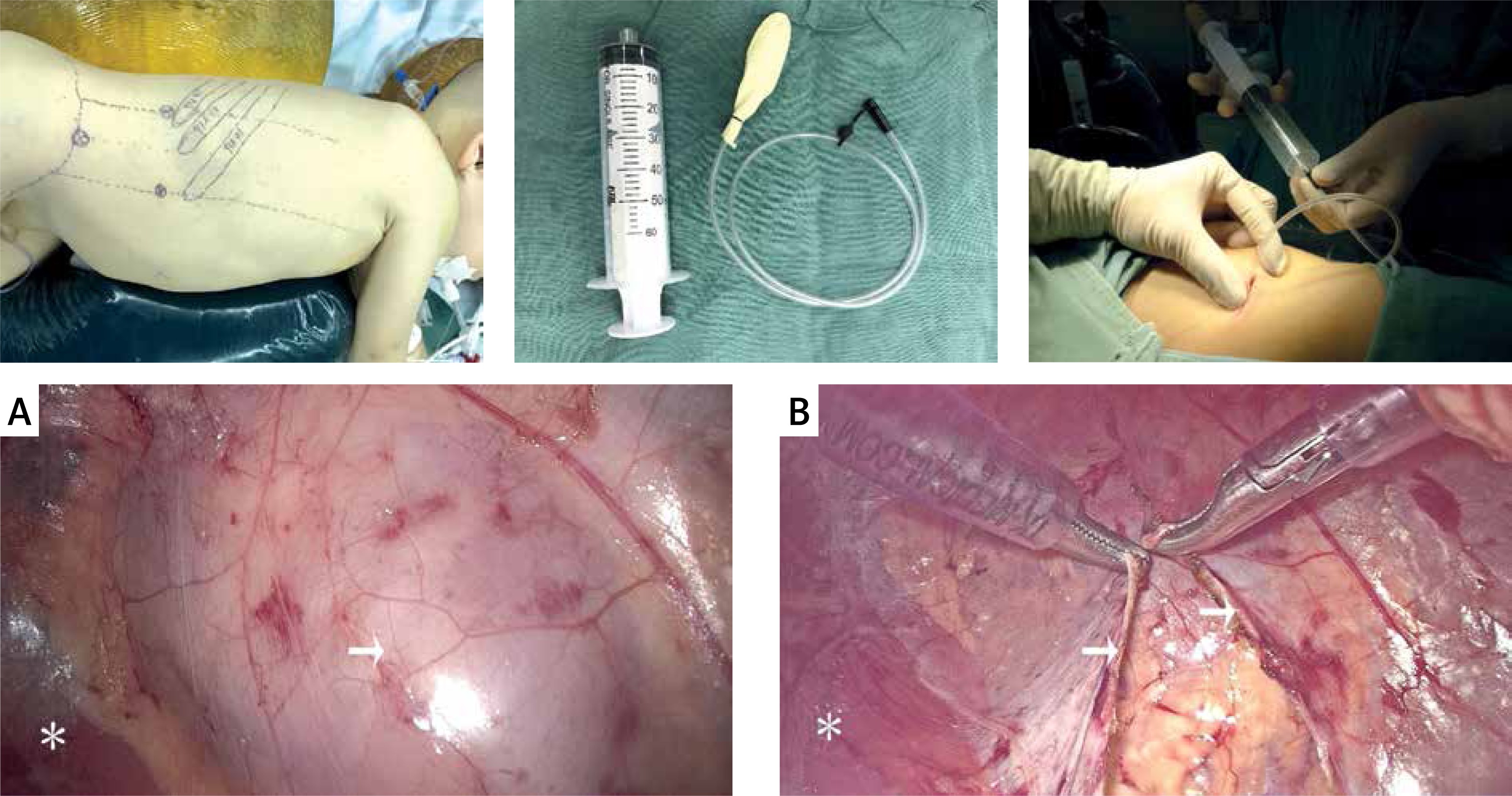
The retroperitoneoscopy was carried out using the technique described by Xu Zhang [6]. The patient was placed in the totally lateral decubitus position on the operating table. A 2-cm skin incision was first made below the 12th rib in the posterior axillary line. Then a homemade balloon was inflated outside Gerota’s fascia to create the retroperitoneal working space. The first trocar was inserted into this 2-cm incision after the balloon expansion. The other two trocars were inserted into the anterior axillary line under the subcostal margin and the midaxillary line above the iliac crest. The dissection began by incising Gerota’s fascia longitudinally to enter the perinephric space. The kidney or adrenal masses were carefully resected after being totally dissociated (Photo 1).
Results
Retroperitoneoscopy was performed in 18 patients, 11 having solid tumor, 2 with cyst and 5 with a nonfunctioning or poorly functioning kidney. As show in Table I, the mean age was 69.5 ±46.9 months (range: 16–156). The mean size of the mass was 6.4 ±3.8 cm (range: 16 to 2) in the largest diameter. The mean operative time was 138.6 ±57.7 min (range: 65–245). Mean hospitalization duration from surgery to discharge was 6.3 ±1.8 days (range: 2–8). The mean time to resume full oral feeding was 30.4 ±11.8 h (range: 12–43). Two patients (patients 14 and 15) were converted to open surgery due to the large diameter of the great mass diameter (16 and 13.5 cm, respectively). Patient 15 received a 400 ml blood transfusion. Pathological diagnoses included two kidney cysts, two renal carcinomas associated with Xp11.2 translocations/TFE3 gene fusion, one adrenocortical carcinoma, one adrenal ganglioneuroblastoma, two adrenal teratomas, two neuroblastomas, one Wilms’ tumor, one cystic solid kidney mass with calcification, one adrenal hemangioma and 5 cases of poorly functioning kidney.
Table I
Patient characteristics and operative details of retroperitoneoscopy
Clinical parameters of 13 consecutive oncological patients who underwent transperitoneal laparoscopy were then collected (Table II), which were used to compared with the 11 solid tumor patients in Table I. As shown in Table III, the transfusion rate (p < 0.05) and mean time to resume full oral feeding (p < 0.01) were significantly lower in retroperitoneoscopy compared to transperitoneal laparoscopy. No significant differences between the two group were found in regard to age, operative time, hospitalization duration and conversion rate.
Table II
Patient characteristics and operative details of transperitoneal laparoscopy
Table III
Statistical analysis of retroperitoneoscopy and transperitoneal laparoscopy in treatment of oncology patients
Discussion
Most pediatric urologists prefer transperitoneal laparoscopy because of a wider working space and familiarization with transperitoneal anatomy compared to retroperitoneoscopy. Comparative studies based on adult patients had showed no significant differences in operative time, estimated blood loss, specimen weight, or complication rates [7–9]. However, few pediatric surgeons attempt to conduct a resection operation of kidney or adrenal masses under retroperitoneoscopy, especially in infants with oncological diseases. Hence most of the pediatric studies were based on the application of retroperitoneoscopy in the management of benign disease such as duplex or nonfunctional kidney. According to our findings in this study, retroperitoneoscopic resection operation of a renal or adrenal specimen is feasible and safe in children, not only for benign disease but also in oncological patients.
Some surgeons prefer to conduct retroperitoneoscopic procedures on patients lying in the prone position [10–12]. The patient lies in the prone position with pads under the chest and pelvis so as to create a working retroperitoneoscopic space. Although there is no significant difference in operative time between the lateral and posterior approaches, the prone position may affect the breathing of the children and reduce their lung capacity. In our opinion, the totally lateral decubitus position can avoid this problem and provide direct access to the adrenal gland and the kidney. This greatly reduces the potential injury to intra-abdominal organs. As shown in Photos 2 A–D, the adrenal masses are safe to dissociate and resect. There was almost no damage to the intra-abdominal organs if all the procedures were conducted within Gerota’s fascia. However, the risk of conversion to open surgery increased with the growth of the specimen’s diameter, because the narrow working space limits the procedure. Hence, retroperitoneoscopy is not recommended for large specimens.
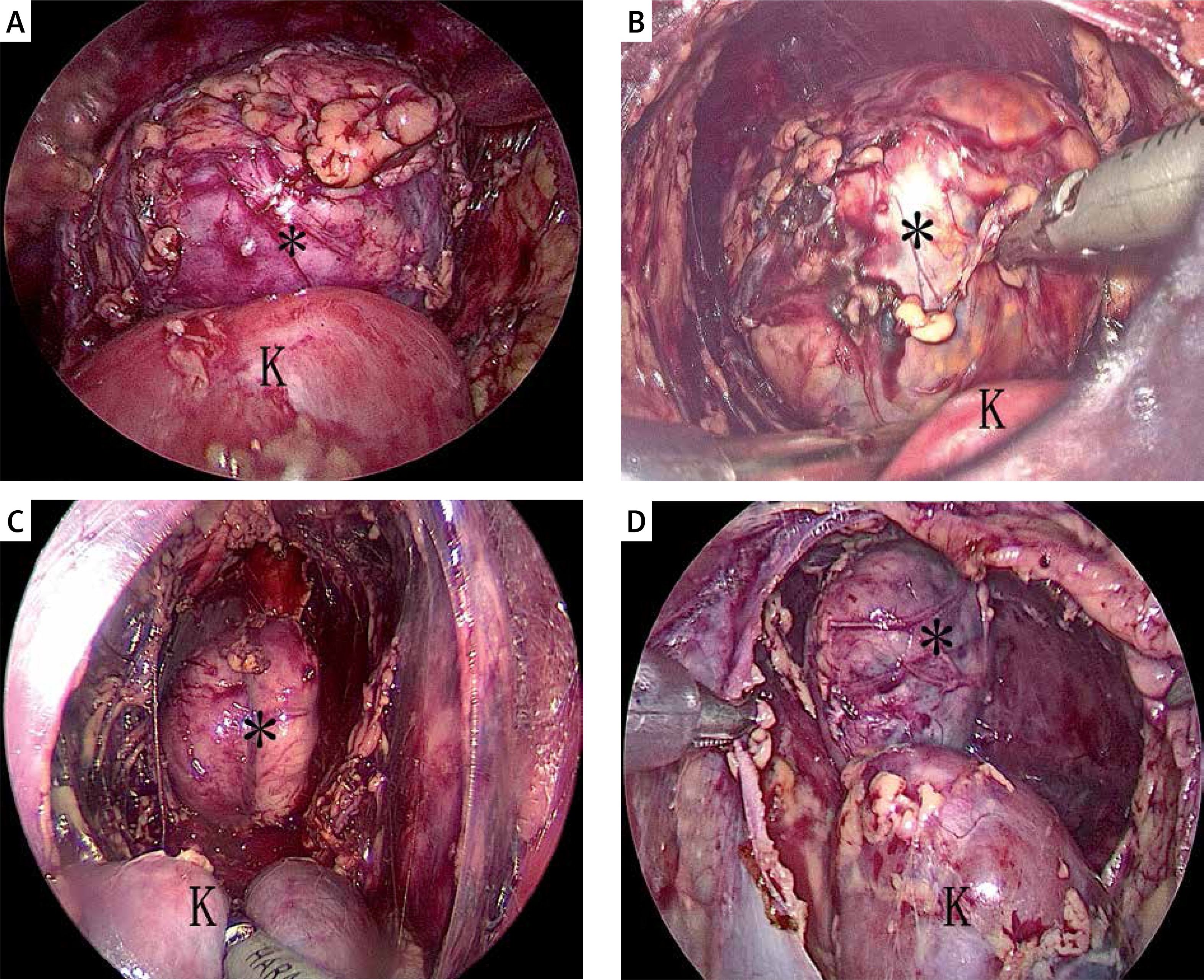
Photo 2
The lateral decubitus position provides direct access to the adrenal and kidney. A, B, C, D are patients 18, 5, 7, 9 respectively. Adrenal mass (black asterisk), kidney (black K)
Another advantage of retroperitoneoscopy in children is that it provides easy visualization of the adrenal vein and the kidney vessel compared to the transperitoneal approach. That greatly reduces the risk of bleeding, which is advantageous when dealing with the oncological patient. Dealing with the central adrenal vein is the last step in adrenal surgery. As shown in Photos 3 A and B, it is safe to clip the central adrenal vein on the surface of the vena cava, although both the patients were 17 months old and the largest diameter of the adrenal mass was 5.5 and 4.5 cm, respectively. Photos 3 C and D show the left side of children on whom retroperitoneoscopic surgery was performed. Both the trunk and branches of the renal artery were safe to visualize when dissected on the surface of the psoas major. The left genital vein and lumbar vein, which drain into the left renal vein, can also be dissected safely in children (Photos 3 C). The transfusion rate, which is significantly lower in retroperitoneoscopy, further confirmed that it is safer in the treatment of the oncological patient than transperitoneal laparoscopy. Moreover, the mean time to resume full oral feeding, which is also significantly shorter in retroperitoneoscopy, demonstrated that the recovery is faster than in the group of transperitoneal laparoscopy.
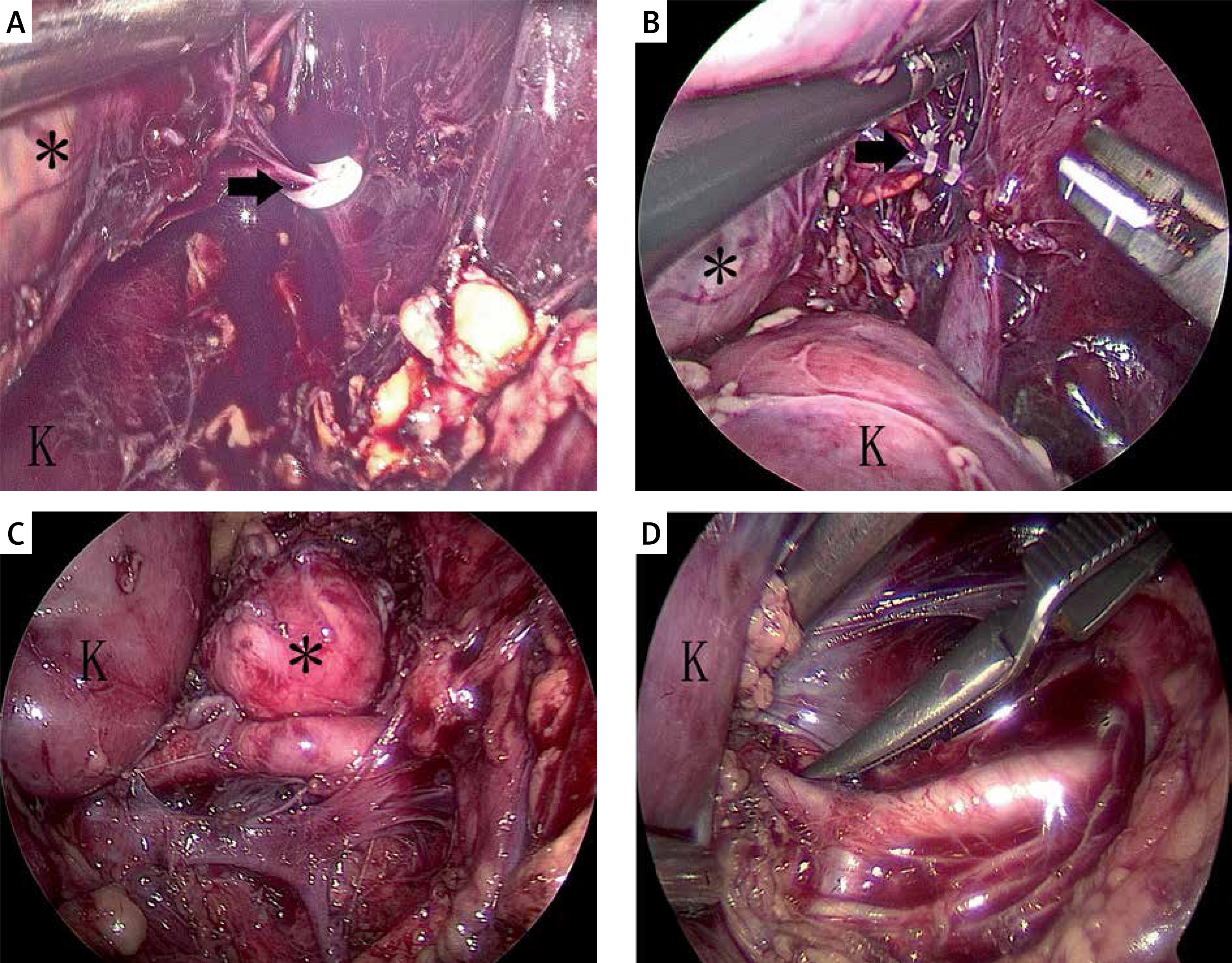
Photo 3
Visualization of adrenal vein and kidney vessel. The central adrenal vein was clipped with a Hem-o-lock (black arrow) in patient 5 (A) and patient 9 (B). C – Renal artery and vein were visualized in patient 8. D – The renal artery branch was dissected and blocked in patient 11. Adrenal mass (black asterisk), kidney (black K)