







Introduction
The number of bariatric procedures performed worldwide still increases [1, 2]. According to Polish guidelines, bariatric surgery is recommended for patients between 18 and 65 years of age, however, qualification for bariatric surgery may be considered in selected cases of patients over 65 considering the patient’s general condition and biological age [3, 4]. The newest guidelines by IFSO/ASMBS indicate that there is no upper age limit for bariatric surgery [5]. Nevertheless, these recommendations do not explicitly refer to revisional bariatric operations (“redo” bariatric procedure). Obesity surgery has proven effectiveness not only in weight reduction, but also in the treatment of comorbidities (such as hypertension, diabetes mellitus or obstructive sleep apnea). The constantly increasing prevalence of obesity in the population and the lengthening of life expectancy affects the number of potential patients with pathological obesity in the elderly, thus increase in bariatric procedures performed in elderly patients, both primary bariatric procedures and revisional procedures, is observed [6]. Bariatric procedures in old age seem to be responsible for improving the quality of life to a greater extent than weight reduction and treatment of comorbidities. Age is an independent risk factor for postoperative complications in elderly patients [7]. Although older patients had more pre- and post-operative comorbidities and lost less weight than younger patients, the weight loss and improvement in comorbidities in older patients were clinically significant [8]. Morbidity and mortality for the patients aged over 70 undergoing bariatric surgery was increased relative to patients aged under 70 [9]. Subsequent surgery performed in the same abdominal region (as is also the case with bariatric revisional procedures) could increase the number of complications [10]. For these reasons, performing bariatric procedures in elderly patients should be well thought-out and it is crucial to analyze the possible benefits of the procedure along with possible complications. The qualification should be even more cautious if we are considering revisional procedure.
Aim
The aim of our study is to assess the indications for revisional bariatric procedures along with the safety and postoperative results in patients over 60 years of age compared to patients under 60.
Material and methods
Study design
The study was conducted among patients undergoing revisional bariatric procedures (RBS). The data were obtained through a multicenter, observational retrospective study involving 16 Polish bariatric centers, dubbed PROSS (Poland Revisional Obesity Surgery Study). In each center, surgeons, nurses and bariatric care coordinators involved in the surgical treatment of obesity recorded data concerning bariatric patients undergoing revisional surgery to create a comprehensive database. Inclusion criteria for this study were patients’ informed consent and revisional bariatric treatment. The study was designed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) [11].
The database included demographic characteristics: sex, age, maximal weight, weight before primary surgery, weight before revisional surgery, height and body mass index. It also included information concerning patients’ comorbidities and addictions – type 2 diabetes (T2D), hypertension, duration of obesity. Additionally, it included data concerning primary surgery (type of surgery, length of hospital stay (LOS)), incidence of complications, outcomes of primary bariatric treatment (lowest body weight, T2D remission, hypertension remission), data concerning revisional surgery (indication for revisional surgery, center conducting revisional bariatric surgery, LOS, type of surgery, complications), outcomes of revisional procedure (current weight, T2D remission, hypertension remission).
The database includes 799 patients who underwent revisional bariatric surgery. All patients were divided into two groups according to age at the time of revisional bariatric surgery: those operated on over 60 (over 60 yo group) and those operated on under 60 (under 60 yo).
Outcomes
Primary outcomes included analysis of indications for revisional (redo) bariatric operations and safety (complications, morbidity and length of stay in hospital). Secondary outcome was the influence of revisional bariatric surgery on the comorbidity treatment and the result of revisional bariatric surgery on weight loss.
Surgical technique and perioperative care
The surgical technique and the perioperative care protocol including the preoperative, intra-operative, and postoperative interventions were standard for each center participating in the study. The course of bariatric treatment due to the subject of the study was coordinated by the multidisciplinary bariatric team in each center, including surgeons, physicians, nurses, dieticians and psychologists.
Statistical analysis
We conducted a descriptive statistical analysis. All data were analyzed using Statistica version 13.1PL (StatSoft Inc., Tulsa, OK, USA). Number and percentage were used for categorical variables. The Pearson χ2 test of independence was used to examine the relationship between them. The Shapiro-Wilk test was used to check for normal distribution of data and the T-student test was used for normally distributed quantitative data. For non-normally distributed quantitative variables, the Mann-Whitney U test was used. Mean and standard deviation was used for continuous variables with normal distribution. Median and range was used for non-normally distributed data. There were no missing data. A p < 0.05 was considered statistically significant.
Ethical considerations
All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments (Fortaleza). The protocol was registered at clinical trials.gov (NCT05108532). There were no changes in treatment for patients included due to the study. The course of the study was closely monitored by a primary investigator who processed and verified any missing or unclear data submitted to the central database. The study was approved by the Bioethics Committee of the Regional Chamber of Physicians, District of Warmia and Mazury, Poland (23/2021/VIII).
Results
Group characteristic
Our data consist of 799 patients who underwent revisional bariatric procedures. 55 (8.1%) patients were older than 60 years of age. The mean age was 43.81 ±9.89 years. The basic characteristics and the influence of redo bariatric procedure on weight loss of the groups are shown in Table I.
Table I
Basic characteristics
The types of primary bariatric procedures are shown in Table II.
Primary outcomes
The most common indication for redo bariatric surgery was weight regain – 340 (42.55%) patients. The aim of revisional bariatric surgery is shown in Table III.
Table III
The indication for revisional bariatric surgery
| The indication for revisional surgery | Under 60 yo | Over 60 yo | P-value |
|---|---|---|---|
| Weight regain | 318 (42.8%) | 22 (40%) | 0.856 |
| Insufficient weight loss | 257 (34.5%) | 21 (38.2%) | |
| Development of complications | 169 (22.7%) | 12 (21.8%) |
One anastomosis gastric bypass (OAGB) and Roux-en-Y gastric bypass (RYGB) were the most frequently performed RBS procedures (296 (37.04%) patients for OAGB and 287 (35.92%) patients for RYGB). The types of revisional procedures are shown in Table IV.
Table IV
Type of revisional procedures
| Type of procedure | Under 60 yo | Over 60 yo | P-value |
|---|---|---|---|
| OAGB | 272 (36.7%) | 24 (43.6%) | 0.512 |
| RYGB | 271 (36.5%) | 16 (29.1%) | |
| SG | 135 (18.3%) | 12 (21.8%) | |
| Other | 61 (8.3%) | 3 (5.5%) |
A total of 212 complications were noted in 181 (22.4%) patients after revision bariatric procedure (25 patients had more than one complication). A total of 9 (16.36%) patients older than 60 years experienced complications after RBS. No postoperative deaths were recorded. All complications are shown in Table V according to Clavien-Dindo classification [12].
Secondary outcomes
After revisional bariatric surgery, patients operated on over the age of 60 achieve comparable weight reduction to patients operated on at a younger age. The influence of the redo bariatric procedure on weight loss and post-operative length of stay in hospital are shown in Table VI.
Table VI
The influence of the redo bariatric procedure on weight loss and post-operative length of stay in hospital
Hypertension was diagnosed in 273 (43.17%) patients prior to redo bariatric treatment. A total of 145 (18.1%) patients prior to redo bariatric surgery were diagnosed with preoperative T2D. Comorbidities are shown in Table VII.
Table VII
Comorbidities before bariatric procedures
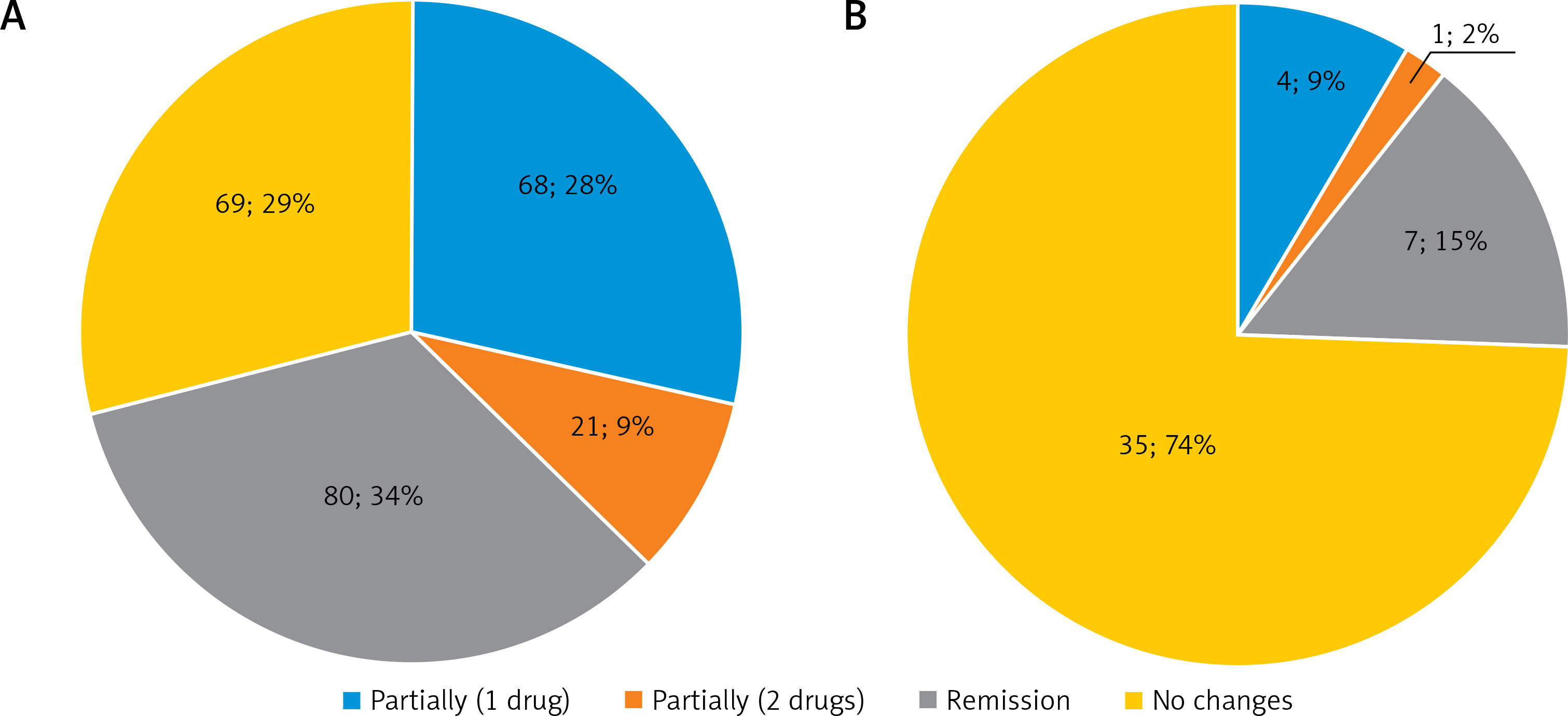
After redo bariatric surgery, 63 (43.4%) patients achieved complete remission of T2D. Better glycemic control in type 2 diabetes and partial remission was observed in 54 (37.2%) of all patients, 47 (37.3%) patients in the younger group and 7 (36.8%) patients in the elderly group. In the group of 87 (31.9%) patients we observed remission of hypertension. Partial improvement of hypertension treatment (reduction of treatment to 1 or 2 drugs) was observed in 94 (34.4%) of all patients, 89 (37.4%) patients in the younger group and 5 (14.3%) patients in the elderly group. In 42.1% and 65.7% of patients in the group of patients over 60 years of age, no changes were observed in the treatment of type II diabetes and arterial hypertension, respectively (in the group of younger patients, the percentage was 16.9% and 29% of patients, respectively). Comorbidities treatment after revision bariatric procedure is shown in Figures 1 and 2.

Discussion
Revisional bariatric procedures are getting more common worldwide and they are also performed on elderly population. In our study, 55 (8.1%) patients over 60 underwent redo bariatric surgery. The most common indications for revisional bariatric surgery in the group of patients over 60 years of age are recurrence of obesity (40%) and inadequate weight loss (38.2%), and no statistically significant differences were found compared to the group of younger patients.
OAGB and RYGB are the most common revisional procedures in both groups of patients with no statistically significant differences. A questionnaire-based survey of 460 surgeons who perform RBS shows that RYGB is by far the most commonly used revisional procedure performed after primary bariatric surgery of any type [13]. In our study, SG and AGB, as primary bariatric procedures, most often require a revisional procedure, both because of the lack of effect of weight reduction and treatment of comorbidities, as well as because of the development of complications. Nearly 20% of the patients scheduled for revisional surgery were qualified due to postoperative complications, mainly exacerbation of gastroesophageal reflux symptoms. The results were comparable in both groups and no statistically significant differences were found. In our study, revisional procedures were most often performed in patients after primary SG and AGB. Therefore, one possible reason for qualifying for revisional surgery due to severe GERD symptoms is the type of primary bariatric surgery.
The third most common primary bariatric procedure among patients undergoing revisional surgery is vertical banded gastroplasty (VGB). In the group of patients revised at the age of over 60 years, 16.4% of primary bariatric procedures were VBG, compared to 5.6% in the younger group. In the past, it was a frequently performed bariatric procedure, but its use has been questioned due to its high risk of complications, unfavorable short- and long-term outcomes, and high risk of revision (up to 80%) [14]. The laparoscopic RYGB is the most commonly performed revisional procedure after VBG [15, 16].
There are no guidelines in the available literature regarding the best revisional procedure for elderly patients. Taking into consideration primary procedures, SG patients had the lowest readmission and reoperation rate, and RYGB patients had the highest procedure-related mortality rate (1.4%) in a group of operated patients aged over 60 years [17]. In our opinion, the procedure should not differ from the guidelines for the entire population, and the choice of method and procedure should be individualized and selected depending on the primary bariatric procedure, patient’s comorbidities and health condition.
Revisional bariatric procedures are more difficult and challenging than primary surgeries, with a statistically higher risk of complications and mortality [18]. Nevertheless, revisional bariatric surgery can be performed with an increased but acceptable risk, with at least short-term weight loss comparable to primary operations [19]. In our study, the overall number of complications was statistically significantly lower in the group of patients over 60 years of age undergoing revisional bariatric surgery, and there was a statistical difference between groups in the number of complications classified as Grade 3 in Clavien-Dindo classification (p = 0.044). A systematic review of bariatric surgeries performed in patients aged 60 years or older shows a pooled overall complication rate of 14.7%, ranging from 1.33% to 47% [20]. Nevertheless, the impact of bariatric procedures in the group of elderly patients on the risk of postoperative complications has been repeatedly investigated and the results presented are controversial and ambiguous. Data obtained in the available literature can be divided into two groups: on the one hand, studies in which the number of postoperative complications in older patients is higher compared to the group of younger patients [9, 19, 21], on the other hand, studies in which the differences in the number of complications are not statistically significant [22–24]. Redo bariatric or metabolic procedures in the elderly are relatively rarely performed and the amount of information in the available literature is limited, so it is difficult to draw reliable conclusions about the risk of postoperative complications based on very limited data. It seems that some of the postoperative complications may be the result of the patients’ advanced age and changes occurring in the body and metabolism of elderly patients, known as the frailty syndrome [25]. Qualification for elective procedures of elderly patients, including bariatric procedures, must be based on a comprehensive health assessment and detection of potential factors increasing the risk of perioperative complications. It is worth noting that age should not be the only factor disqualifying a patient from an elective bariatric procedure.
The length of stay in hospital was comparable in both groups and amounted to 3 days. Revisional procedures are more complicated and involve a prolonged hospital stay compared to primary procedures [26]. Hospital stay after surgery in elderly patients is also extended, e.g. due to multi-morbidity, as a result of the frailty syndrome and worse physical condition. LOS after revisional procedures can be shortened using the early discharged principle, in accordance with the Fast Tract Protocol (FTP), as a safe method that does not increase postoperative complications, but requires open and frequent contact between patients and medical personnel [27]. The FTP concept in patients undergoing bariatric surgery is safe and reliable and should be recommended in bariatric surgery practice [28]. In the RCT study, the FTP applied to elderly patients after laparoscopic oncological surgeries promote faster postoperative recovery, improve early postoperative nutritional status better, and more effectively reduce postoperative stress reaction [29]. An RCT study evaluating the use of the FTP protocol in elderly patients after revisional bariatric procedures may yield interesting results.
Revisional surgery in patients over 65 years of age may produce comparable results in terms of weight loss and resolution of comorbidities compared to younger patients [24]. In our study, BMI index, EWL and %WL after revisional surgery in both groups was comparable with the average postoperative follow-up time of 23 months. Few studies confirmed that bariatric surgery is effective in older patients to achieve significant weight loss and EWL [24, 30, 31]. Bariatric surgery for older patients has been shown to be safe and effective not only for EWL but also in improvement of obesity comorbidities, especially type 2 diabetes and blood pressure [30].
Bariatric surgery improves the quality of life of obese elderly patients without compromising their nutritional status, and this may be an important argument in preoperative assessment of patients and qualification for revisional procedures [32]. Bariatric surgery including diversionary procedures (RYGB, BPD-DS) is safe and effective in improving obesity-related comorbidities in older patients (≥ 60 years) especially those suffering from super obesity [33]. In our study, comorbidities (HTH and T2D) were present more often in the group of patients undergoing revisional surgery over 60 years of age (34.5% vs. 16.9% for T2D and 63.6 vs. 31.9 for HTH). This group of patients before the primary bariatric procedure also suffered from HTH and diabetes in a higher percentage compared to the group of younger patients (38.2% vs. 22.2% for T2D and 69.1 vs. 39.9 for HTH). Revisional surgery in patients with persistent or relapsed T2D after bariatric surgery can significantly improve glucose control and use of diabetes medications [34]. The authors of meta-analysis of 33 studies, with a total of 1593 patients, suggest that revisional bariatric surgery improves the outcomes of obesity-related comorbidities (92% of patients had improvement in diabetes with 50% remission and 81% achieved improvement of hypertension with 33% complete remission after RBS) and should be considered in patients with persistent metabolic disease after primary bariatric surgery [35]. Meta-analysis of old versus young patients revealed that bariatric surgery for patients ≥ 55 years results in weight loss and reduction in comorbidities comparable (but with better comorbidity outcomes for younger patients) to the general bariatric surgery population [36]. The results of our study were similar as the above-mentioned meta-analysis. An improvement of HTH treatment (reduction in the number of drugs and remission) after revisional surgery were more frequent in younger patients (71% vs. 26%). Similar results were obtained in the treatment of T2D, much higher percentage of patients achieved remission of diabetes in the group of operated patients under 60 years of age (47% vs. 13%). Data available in the literature show that bariatric surgery performed in elderly patients may improve or resolve 84.41% of the co-morbidities with the average remission rate of 34.74% [23]. Higher first-year percentage total body weight loss, lack of preoperative insulin use, and younger age at operation were independently associated with T2D remission after RYGB [37]. Greater weight regain before RBS was minimizing odds for bariatric success in patients operated due to weight regain or insufficient weight loss. OAGB was associated with a greater chance of complete remission of hypertension and/or diabetes [38]. The duration of diabetes and preoperative BMI and C-peptide levels are the independent factors predicting complete remissions [39]. Short duration of T2D , low baseline HbA1c and no need for insulin treatment are all favorable predictors of T2D remission following bariatric surgery [40, 41].
Our study is limited by the biases of retrospective analysis and a small sample size in a cohort of older patients undergoing a revisional bariatric surgery. Due to the overall rare nature of revisional surgery nationally, compounded by the fact that these revisions are even rarer in elderly patients, our small sample size is unavoidable.
Conclusions
Revisional bariatric procedures appear to be safe and appropriate in elderly patients. Revisional bariatric procedures in the group of patients over 60 years of age do not cause an increased risk of postoperative complications or prolonged hospital stay. Despite the comparable effect of weight loss after revisional surgery, the possibility of achieving remission or improvement in the treatment of comorbidities in patients operated on over 60 years of age is relatively lower than in the group of patients operated on under 60 years of age. Regarding the qualification for revisional bariatric procedures in patients over 60 years of age should be made rationally, after prior analysis of the periprocedural risk and the potential benefits of the introduced treatment.