
Summary
Congenital heart disease (CHD) is the most common malformation from birth. The severity of the different forms of CHD varies extensively from superficial mild lesions with follow-up for decades without any treatment to complex cyanotic malformations requiring urgent surgical intervention. One of the most common severe forms of CHD is tetralogy of Fallot (TOF), characterized by a misalignment of the canal septum leading to a deviation of the aorta to the right. microRNAs (miRs) are crucial in cardiac development, giving rise to possible phenotypes in CHD. Therefore, we aimed to evaluate the expression of miRs in 23 children with TOF and 45 controls and correlate them with the clinical characteristics of both the children and the mothers. We analyzed the miRNA expression of miR-21-5p, miR-155-5p, miR-221-3p, miR-26a-5p, and miR-144-3p by RT-qPCR. In this study, we found that miR-221-5p, miR-21-5p, and miR-144-3p exhibited a significant difference in expression compared to controls. Through bioinformatics analysis, we found that the target genes of analyzed mIRs are members of the AKT1, SMAD, TNF-α, and FOX families. All have in common that they are associated with different cellular pathways that lead to cell cycle changes, cell growth, and apoptosis, mainly in hypoxic conditions. The expression levels of miRs in pediatric patients may contribute to the development of TOF. Additionally, the high expression of miR-221-5p, miR-21-5p, and miR-144-3p in children with TOF is associated with genes associated with many cellular pathways involved in TOF development.
Introduction
Congenital heart disease (CHD), defined as structural heart defects that occur at birth, is a common problem in pediatric patients. The severity of CHD varies widely from mild superficial lesions followed for many years without the necessity of treatment to complex cyanotic malformations that require immediate surgical intervention. One of the most common severe forms of CHD is tetralogy of Fallot (TOF), with an estimated incidence of five to seven per 10,000 live births, representing between 5% and 7% of all congenital heart lesions [1]. TOF is characterized by a misalignment of the canal septum, leading to a deviation of the aorta to the right. Consequently, it results in a significant ventricular septal defect (VSD) and varying degrees of narrowing of the right ventricular outflow tract, requiring surgical repair within the first years of life [2, 3]. Clear spatial and temporal transcript splicing transitions are conserved in the vertebrate heart during fetal and postnatal development [4, 5]. The proper transition from a fetal transcript splicing pattern to a postnatal pattern is required for correct heart development.
miRs are small non-coding RNA (~19–24 nucleotides in length), which are evolutionarily conserved and are known as post-transcriptional regulators of gene expression by binding to complementary target sequences in messenger RNA (mRNA). In the context of TOF, abnormal expression of specific miRs has been shown to play a significant role in the development of the disease. These miRs can coordinate and regulate multiple target genes that encode proteins with related functions, such as stem cell differentiation, neurogenesis, skeletal and cardiac muscle development, and function [6–9]. Furthermore, multiple miRs can interfere with individual mRNAs, allowing for enormous combinatorial complexity and regulatory potential in TOF development.
Recent advances in identifying new epigenetic biomarkers have highlighted the epigenetic function in some CHDs related to the intrauterine environment, which can help prevent, diagnose, and treat this type of CHD [10]. The potential of miR-21-5p, miR-144-3p, and miR-155-5p as biomarkers associated with fibrosis mechanisms [5, 11], and miR-26-5p and miR-221-3p related to angiogenesis [12], and miR-155-5p associated with the response to oxidative stress [13] offers a promising future for prenatal identification of fetal CHD [14–17]. These miRs, when identified in the prenatal stage, can serve as early indicators of potential CHD, allowing for timely intervention and management. We aimed to evaluate the expression levels of these miRs and their clinical significance in TOF patients, paving the way for more accurate and early diagnosis.
Material and methods
Patient population
A total of 68 children less than 3 months of age participated in this study, including 23 with TOF requiring surgical reconstruction from the Instituto Nacional de Cardiología, Ignacio Chávez, and 45 healthy children from the Instituto Nacional de Perinatologia (INPer). The study patients were carefully selected based on a structural approach, and imaging studies were conducted using echocardiography or tomography and angiography, ensuring the reliability of the diagnosis. The sample was taken before any clinical or surgical procedure, and controls without a family history of CHD and health diagnoses endorsed by a specialist doctor were recruited from INPer among individuals who went to the institute’s lactation bank. The exclusion criteria for both study groups were having other malformations or syndromes associated with infectious processes at the time of sample collection. Necessary information was collected from the medical records of each patient. In addition, the participants’ parents signed informed consent before the sample collection. The family and medical history information of the perinatal risk factors of participants and their mothers was obtained by medical records and standardized questionnaires.
The patient’s blood pressure (BP) readings were performed with number 2 and 3 bracelets, as the American Heart Association (AHA) indicated. The measurement bracelets were placed on the patient’s right arm, measuring the supine position with the oscillometric method using a Philips M3046A monitor that meets AAMI SP-10 precision. In all cases, three successive shots were taken with a difference of 2 min between each shot. Heart rate and O2 saturation were measured using a Nellcor pulse oximeter (PM1000N). Vital signs were recorded on the same day the blood samples were obtained. This study was conducted according to the Declaration of Helsinki and approved by the National Institute of Cardiology Ethics Committee (Institutional Review Board, Number: 20-1181).
Blood and plasma sample
Subject blood samples were collected during study enrollment and placed into sterile tubes containing EDTA. Plasma was separated immediately by centrifugation for RNA isolation.
RNA extraction
Total RNA was extracted from plasma samples using the miRNeasy Serum/Plasma Kit (Qiagen) according to the manufacturer’s instructions. As an internal control, a synthetic miR (cel-miR-39 from C. elegans) was added to each sample in equal amounts. The total RNA was subsequently stored at –80°C.
miRNA quantitation using real-time PCR
Reverse transcription reaction was performed in samples of total RNA of plasma using the specific primers for miR-21-5p, miR-26a-5p, miR-144-3p, miR-155-5p, and miR-221-3p with the TaqMan MicroRNA Reverse Transcription Kit (Thermo Fisher). The expression levels were quantified using a commercial kit (TaqMan Gene Expression Assay, Thermo Fisher), employing the CFX96 Touch Real-Time PCR Detection System (Bio-Rad). Cycling conditions were 2 min at 50°C and 10 min at 95°C, followed by 40 cycles of 15 s at 95 °C and 1 min at 60°C [17]. Expression levels were measured in duplicate and normalized with the endogenous gene cel-miR-39_1. Relative quantification was carried out using the 2-ΔΔCT method [18].
Statistical analysis
Data were analyzed using SPSS v21 software (IBM Corp., Armonk). (https://www.ibm.com/mx-es/products/spss-statistics). The normality of each variable was determined using the Kolmogorov-Smirnov test. The mean ± standard deviation (S.D.) was used to represent the quantitative variables, and the qualitative variables were reported as frequencies with percentages. The median with an interquartile range of 25 to 75% (IQR) was used to represent the relative expression of miRs based on distribution analysis. Variables were compared using Student’s t test or the Mann-Whitney U test for two groups and the Kruskal-Wallis test for comparison between more groups. The diagnostic value of miRNA expression was assessed by calculating the area under the curve (AUC) in ROC models and Youden’s score index of each miR to define the optimal cut-off point. Data were presented as odds ratios (OR) with a confidence interval of 95%. A level of p < 0.05 was considered statistically significant.
Results
Clinical characteristics
Sixty-eight children were included in this study, of whom 23 had a TOF diagnosis and 45 subjects constituted the control group (CG). The anthropometric and clinical characteristics of the study population are shown in Table I. Samples were collected from all children during the first month of birth. We found that heart rate (p = 0.002), respiratory rate (p = 0.001), and oxygen saturation (p < 0.001) were statistically different between groups.
Table I
Clinical characteristics of the study participants and their mothers
miR expression
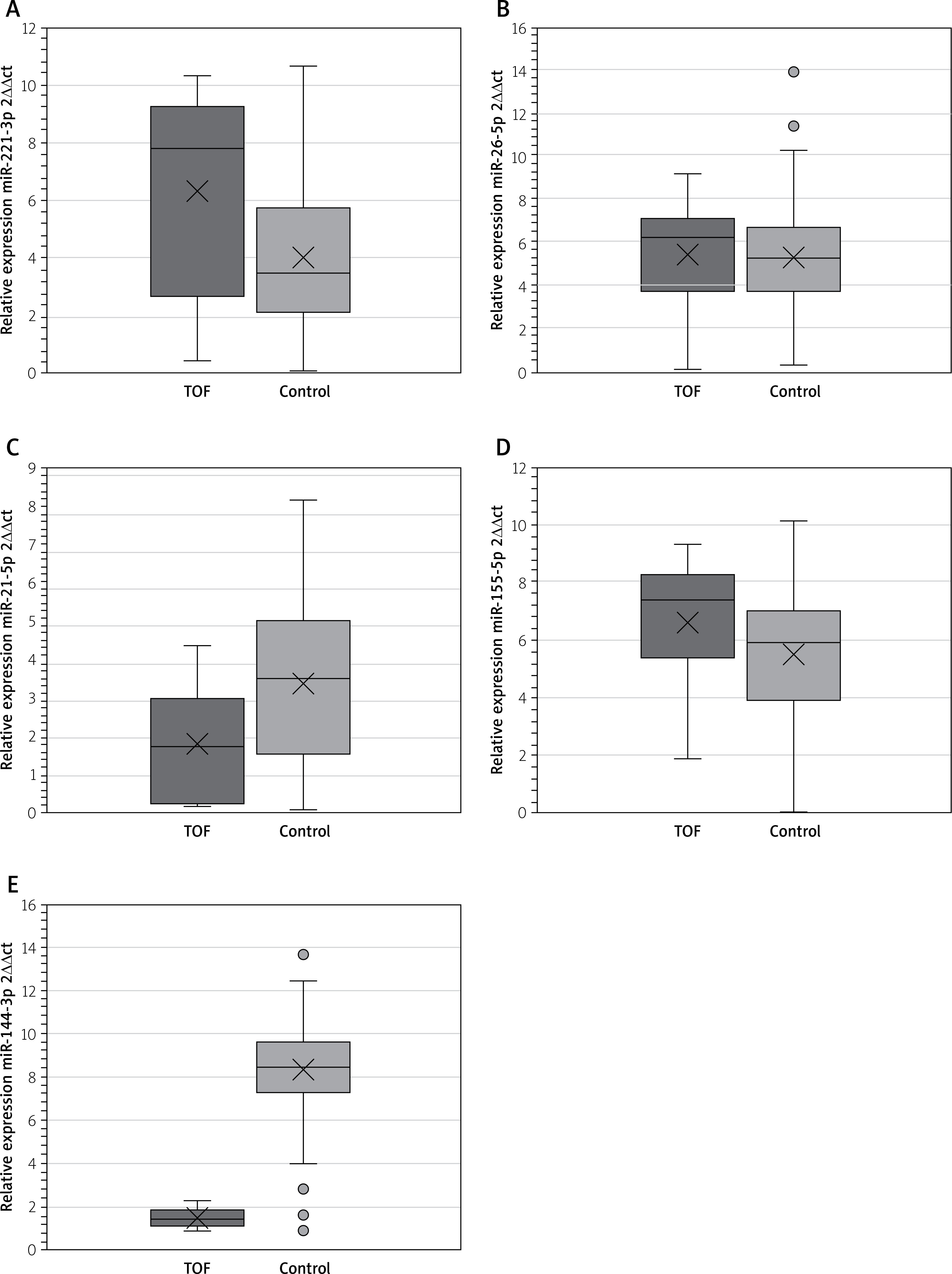
Plasmatic miR analysis of TOF and the control group was carried out. TOF had significantly higher expression of miR-221-3p compared to controls (7.764 (0.083–10.22) versus 3.427 (0.062–10.65); p < 0.001); miR-26-5p (6.215 (0.108–9.170) versus 5.246 (0.257–10.285); p = 0.07), and miR-155-5p (7.387 (1.863–9.341) versus 5.879 (0.010–10.152); p = 0.50). Otherwise, miR-21-5p (1.856 (0.248–4.474) versus 3.450 (0.091–8.382); p = 0.008), and miR-144-3p (1.51 (0.926–2.302) versus 8.287 (4.033–12.472); p = 0.001) had statistically lower expression in TOF (Figure 1).
ROC curve analysis
To evaluate whether the miRs analyzed could serve as potential biomarkers for the diagnosis of TOF, ROC curve analyses were performed with the AUC of the miRNAs studied. The results obtained were miR-21-5p (0.727 (95% CI: 0.651–0.803)), miR-26-5p (0.760 (95% CI: 0.689–0.831)), miR-144-3p (0.568 (95% CI: 0.479–0.656)) and miR-221-3p (0.450 (95% CI: 0.358–0.542)), and miR-155-5p (0.362 (95% CI: 0.274–0.449)). Then, we calculated Youden’s index score to establish an optimal cut-off value for each miR, considering only those miRs that had a discriminative capacity above 0.5 (cutoff = 0.230 for the miR-21-5p, cut-off = 0.330 for the miR-26-5p, cut-off = 0.165 for the miR-144-3p; Figure 2).
Figure 2
ROC curve analysis. A ROC model was performed to differentiate between the control and congenital heart disease groups. The whole population was analyzed, 23 TOF patients and 45 controls. The optimal cut-off point was defined through Youden’s score index to maximize the sum of sensitivity and specificity of miR-21-5p, miR-26-5p, and miR-144a-3p

Finally, we conducted bioinformatic analyses. Through TargetScan (http://targetscan.org/vertGO/), we searched for genes related to the miRs analyzed. Subsequently, the interaction network generated by GeneMANIA revealed the complexity of these molecular interactions, showing how their target genes interact within these pathways (Figure 3).

Discussion
To evaluate the roles of miRs in the development of TOF, we analyzed the plasmatic expression of miR-21-5p, miR-155-5p, miR-221-3p, miR-26a-5p, and miR-144-3p in children with and without TOF.
First, we analyzed the clinical variables in both children and mothers. We found significant differences in beats, breaths, and oxygen saturation between the two study groups. It is known that TOF is the most common cyanotic congenital heart disease in children beyond the neonatal period, with an incidence of 7–10% of all congenital disabilities [19]. TOF is a heart defect that involves a combination of four related heart defects that often occur together: ventricular septal defect, aortic overriding, right ventricular outflow tract obstruction, and right ventricular hypertrophy [2]. However, the clinical presentation depends fundamentally on the degree of pulmonary obstruction. Therefore, these differences in the clinical manifestations of children with TOF were to be expected. On the other hand, in the case of obstetric history, we did not find significant differences between the groups of mothers.
As with most congenital heart defects, the precise etiology of the malformation is unknown, and 90% may be related to genetic and environmental factors [20]. Several studies have focused on analyzing miRs and their association with the pathogenesis of congenital heart disease using different models, such as murine and cell cultures; however, there are few studies in children.
In this study, we found that miR-221-3p, miR-26-5p, and miR-155-5p showed higher levels of expression; however, only miR-221-5p showed a significant difference. Otherwise, both miR-21-5p and miR-144-3p had lower expression compared to controls.
In this context, miR-221 is encoded in tandem with a gene cluster on the X chromosome (Xp11.3). Previous studies have shown that miR-221 participates in many types of cancer, such as breast cancer, liver cancer, pancreatic cancer, prostate cancer, gastric cancer, colorectal cancer, glioma, multiple myeloma, and inflammatory diseases [21, 22]. These pathologies are linked to various cellular pathways, resulting in alterations to the cell cycle, proliferation, growth, and apoptosis [23]. Through bioinformatics analysis, we found that miR-221 interacts with SMAD proteins and transforming growth factor β (TGF-β). SMADs comprise a family of structurally similar proteins that are the primary signal transducers for receptors of the TGF-β superfamily, critically important for regulating cell development and growth. TGF-β2 may be a target gene for diagnosing and treating children with CHD by the TBX1/miR-193a-3p/TGF-β2 axis. This pathway regulated cardiomyocyte ferroptosis, which could be involved in cardiac defects; also, overexpression of TGF-β2 reduced nuclear factor erythroid 2-related factor (NRF2) protein expression [24, 25]. Otherwise, we found that both miR-21-5p and miR-144-3p had lower expression than the control group. Lacedonia et al. [26] reported a reduction in the expression of miR-23, miR-210, miR-21, and miR-145 under hypoxic conditions – as if there was a kind of “annihilation effect”, as they described it; similar hypoxic conditions are found in TOF patients. Arterial oxygen saturation in children with tetralogy of Fallot may decrease abruptly and noticeably. This phenomenon, known as the tetralogy period, usually occurs due to a sudden, more significant constriction of the outflow tract to the lungs. Hence, blood circulation to the lungs is further limited. Other reports revealed that miR-21 was sensitive to sustained hypoxia, which could downregulate the expression of miR-21 in cardiomyocytes [27]. During hypoxic conditions, the cellular response is modulated by activation of the hypoxia-inducible factor, which regulates the expression of many genes involved in metabolism, angiogenesis, erythropoiesis, cell proliferation, differentiation, and apoptosis. Han et al. [28] demonstrated that miR-21-5p inhibits Bax expression and increases Bcl-2 expression, inhibiting cell apoptosis and reducing the effect on the PTEN/AKT1/FOXO3 signaling pathway in cardiomyocytes.
On the other hand, the evidence regarding miR-144-3p identification in congenital heart diseases in pediatric age is very scarce and practically non-existent in TOF. Abu Halima et al. [29] studied adult patients later after surgical repair of non-syndromic TOF by analysis of circulating miRs by microarray. They reported changes in the expression of some miRNAs, among which the most significant were miR-1231, miR-144, and miR-505, with fold changes of 6.94, 4.82, and 4.61, respectively. Using another method, Liang et al. [30] demonstrated that miR-144-3p could be a predictor of increased risk of type 2 diabetes (T2DM) and insulin resistance; significantly upregulated expression of miR-144 in T2DM patients indicated downregulated expression of the gene ADBR2/ADBR3 (β-adrenoreceptors), an essential target for epinephrine. Different polymorphic forms, point mutations, and downregulation of this gene are associated with nocturnal asthma, obesity, T2DM, and cardiovascular disease. Also, miR-144-3p downregulated expression of the gene NR3C1. This glucocorticoid receptor can function as a transcription factor that binds to glucocorticoid response elements in the promoters of glucocorticoid-responsive genes to activate their transcription and as a regulator of other transcription factors. This receptor is involved in inflammatory responses, cellular proliferation, and differentiation in target tissues [31]. Chen et al. [32] identified through bioinformatics analysis five genes (TIGAR, CEP55, E2F8, STIL, and TOP2A) as core genes in lung cells as candidate genes for miR-144-3p [33]. In particular, TIGAR is known to be involved in suppressing proliferation, mediating programmed cell death, and autophagy.
Finally, through bioinformatics analysis, we found that among the target genes in the analyzed miRs are AKT serine/threonine kinase 1 (AKT1), also called protein kinase B. AKT kinase comprises three isoforms in humans – AKT1, AKT2, AKT3 – and they have a similar structure but not function. AKT1 in embryos and newborns of AKT1-deficient mice are found to have heart defects, and heart function also decreases, indicating that AKT1 is indispensable for heart development and function [34, 35]. AKT is a crucial signaling protein involved in many biological processes, such as cell survival, growth, proliferation, and protein synthesis. AKT participates downstream of phosphoinositide 3-kinase in the signaling pathway. Phosphoinositide 3 kinase/protein kinase B pathway is a critical regulator of mesodermal progenitor cells – original cells of heart development in the embryo stage – especially by modifying expression of transcription factors in the heart.
However, investigations of circulating miRs in TOF patients still need to be completed. In this study, we aimed to identify the specific patterns of circulating miRs in the blood of patients with TOF and assess whether these particular miRs may help differentiate patients with and without TOF. Furthermore, multiple miRNAs can target individual mRNAs, allowing enormous combinatorial complexity and regulatory potential.
These observations suggest that circulating miRs predict TOF illness and sensitive biomarkers for improving the diagnostic accuracy of TOF.
The limitations of this work were: 1) The number of pediatric patients ought to have been higher; however, the fact that they were children under 100 days of age, coupled with their clinical condition, limited sample collection and made the study more complicated. 2) It is essential to carry out more studies on the role of the proposed miRNAs according to the specific type of heart disease present. One of the models had a wide confidence interval, which is observed when the sample size is smaller; however, the statistical significance achieved strengthens the study’s ability to verify the findings’ reproducibility and certainty.
Conclusions
To our knowledge, this is the first study to report dysregulation of the expression of plasma levels of miR-221-3p, miR-155-5p, miR-144-3p, and miR-21-5p in human patients with TOF compared to controls, indicating their potential role in the severity and progression of the disease. Additionally, the bioinformatic analysis identified their relationship with genes such as AKT1, SMAD, and FOX, which can participate in cardiogenesis and, therefore, in the appearance of the disease.







