
Introduction
Gallbladder wall thickening has a wide range of differential diagnosis, including various inflammatory conditions and cancer [1]. This poses a diagnostic dilemma, especially in geographic regions of the world with high incidence of gallbladder cancer (GBC) [2]. Failure to diagnose GBC in thickened gallbladder results in poor prognosis. Dual energy computed tomography (DECT) has been utilized with encouraging results in various oncological conditions [3, 4]. There is a paucity of data on the role of DECT in biliary diseases, except the improved detection of biliary stones [5]. Specifically, there are no studies on the role of DECT in the evaluation of gallbladder wall thickening.
Material and methods
The local ethics committee approved this retrospective study with waiver of informed consent (approval number: RDG/EC/Pub/06). Consecutive patients with suspected gallbladder wall thickening type of GBC who underwent DECT in the period from August 2020 to March 2021 were included. DECT examinations were performed on a 128-row detector dual source scanner (Somatom Definition Flash, Siemens Healthcare, Germany). The acquisition protocol comprised a dual-energy late arterial phase scan of the upper abdomen and a single-source portal-venous scan of the entire abdomen. Using the liver virtual non-enhanced (VNC) setting, an iodine map was generated. Iodine subtraction yielded VNC images.
The iodine maps and 80 keV/140 keV datasets were reviewed independently by two radiologists (1.5 years of experience in body imaging) The differences were resolved by a radiologist with 7 years of experience in abdominal imaging. All were blinded to the final diagnosis.
The findings specifically recorded on the iodine maps and compared with 80 keV and 140 keV datasets were symmetry of involvement, pattern of mural thickening, enhancement pattern, and intramural characteristics (Table 1). Additionally, the iodine density (mg I/ml) was evaluated at the site of thickening. The diagnosis of calculi was compared among VNC, 80 KeV and 140 KeV images. The final diagnosis was based on the histopathology or cytology from the gallbladder wall or from the metastatic sites. Ultrasound was the reference standard for gallbladder calculi.
Table 1
Dual energy CT findings in seven patients with gallbladder wall thickening
Results
Seven patients [mean age 52.3 years (range, 30-69 years); 5 males] were included Three patients underwent extended cholecystectomy [carcinoma (n = 1) and xanthogranulomatous cholecystitis (XGC) (n = 2)]. Carcinoma was diagnosed in the rest of the patients based on cytology. Calculi were present in two patients on ultrasound.
Three patients had diffuse thickening. Focal thickening of the body and fundus were seen in 3 and 1 pa-tients, respectively. Mean mural thickness was 4.32 mm (range, 3.3-5 mm). The interface with the liver, antropyloric region, and duodenum was indistinct in all the cases. The interface with the colon was indistinct in three patients. Biliary dilatation was seen in 5 patients (infiltration by mural thickening). Vascular involvement, liver metastases, omental metastases, ascites, and lymphadenopathy were present in 4, 3, 3, 2, and 6 patients, respectively.
The comparative findings on iodine maps, 80 keV, and 140 keV images are shown in Table 1 and Figures 1-3. None of the patients had intramural cysts. The mean iodine density in patients with carcinoma was 1.35 mg I/ml (±0.20) compared to 0.85 mg I/ml (±0.33) in patients with XGC (p = 0.79).
Fig. 1
Gallbladder wall thickening in a 30-year-old man with carcinoma. A) In the 80 keV image, the thickening is subtle (arrows) and characteristics including asymmetry and heterogeneity are difficult to assess. B) At 140 keV, the thickening is not apparent. C) Iodine map shows heterogeneous asymmetrical mural thickening (arrows) better than 80-keV
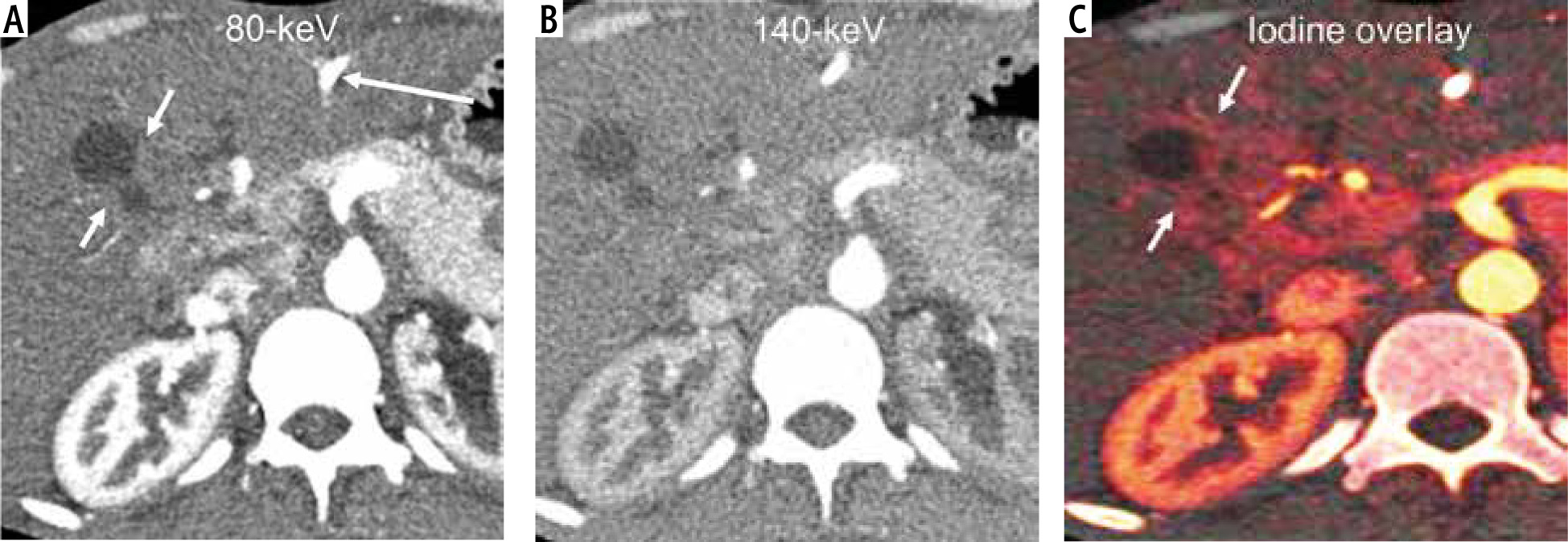
Fig. 2
Gallbladder wall thickening in a 69-year-old woman with carcinoma. A) 80 keV image shows asymmetric mural thickening of the body of the gallbladder (short arrows). A prominent enhancing mural nodule is seen (arrow). B) At 140 keV, the entire extent of the thickening is not apparent. Enhancing mural nodule (arrow) is seen (C). Iodine map shows heterogeneous asymmetrical mural thickening (short arrows) as well as liver infiltration better than 80-keV. The mural nodule is also seen
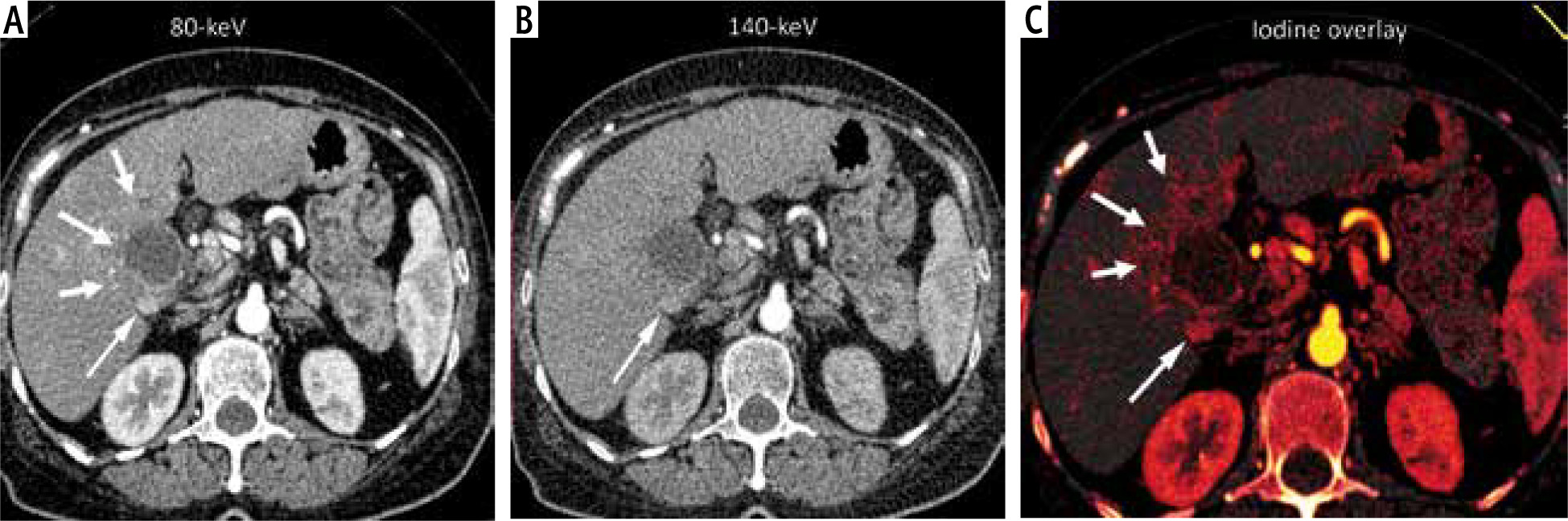
Fig. 3
Gallbladder wall thickening in a 46-year-old man with xanthogranulomatous cholecystitis. A) 80 keV image shows asymmetric mural thickening of the body of the gallbladder (arrows). Note that the gallbladder is contracted. B) At 140 keV, the thickening is poorly visible. C) Iodine map shows asymmetrical mural thickening (arrows) with lower iodine uptake (0.66 mg I/ml) than in case 1 (1.36 mg I/ml) and case 2 (1.66 mg I/ml). Also note that the gallbladder is adherent to the antropyloric region

Discussion
In this study evaluating the role of DECT in suspected gallbladder wall thickening type of GBC, we found that the iodine maps and 80 keV dataset performed better than the 140 KeV dataset for depiction of mural characteristics. There was higher iodine uptake in GBC compared to XGC. Accurate evaluation of mural characteristics is critical for diagnosis of gallbladder wall thickening. Single layered heterogeneously enhancing mural thickening and bilayered thickening with a thick inner layer have been reported as predictors of gallbladder malignancy on routine CT [6-9]. Besides enhancement, detection of intramural hypodense nodules, intramural cysts, interface with adjacent structures, liver metastases, and omental nodules is useful in characterization of gallbladder wall thickening [10]. DECT may provide better characterization of these features compared to routine CT. Additionally, the iodine density map generated from DECT may be an objective surrogate marker for differentiation of benign and malignant gallbladder wall thickening.
Limitations include the small sample size and lack of histopathology in all cases. Wall thickening due to adenomyomatosis, chronic cholecystitis, and polyps is not represented in this series.
In conclusion, there is a potential role of DECT in characterization of non-acute gallbladder wall thickening.





