
Hydatid cyst is a common dsease in developing countries caused by Echinococcus granulosus, affecting mainly the liver and lungs with a prevalence rate of 5–10% in endemic parts of Asia [1]. According to the global tuberculosis report 2020, tuberculosis is one of the top ten causes of death worldwide, accounting for 10 million cases, with India bearing a 26% global burden [2]. Ruptured hydatid cyst is a diagnostic challenge, radiologically presenting as a recurrent pneumothorax with an incidence rate of 2.4–6.2%, while co-existing pulmonary tuberculosis (PTB) with ruptured hydatid cyst and a recurrent pneumothorax has been rarely reported in the literature [3]. With no reports to date, we hereby report a tri-combination of ruptured hydatid cyst presenting as a recurrent pneumothorax with co-existing pulmonary tuberculosis and uniportal thoracoscopic management.
A 24-year-old male patient presented with sudden onset of dyspnea and chest pain for 2 days with a history of ipsilateral pneumothorax 15 days back, previously managed by intercostal tube drainage and unremarkable family history. He was hemodynamically stable and afebrile. Chest examination revealed decreased chest movement, hyper-resonant note and absent vocal fremitus on the left hemithorax with the absent breath sound. A massive pneumothorax with a collapsed left lung detected on a routine chest X-ray (Figure 1 A) was intervened with an intercostal chest tube. For 1 week, the lung did not appear to expand on repeated chest X-rays obtained at 48-hour intervals. Chest computed tomography (CT) done after 72 hours following chest tube insertion revealed a thick-walled cavitary lesion in the left lower lobe communicating with the pleural cavity with an underlying membranous structure and contralateral parenchymal nodular and infiltrative lesions (Figure 1 B). Bronchoscopy detected broncho-pleural fistula in the left lower bronchial orifice with negative findings for Mycobacterium tuberculosis in bronchoalveolar lavage and regular blood investigations. Both hydatid serology and sputum acid-fast bacilli testing were negative. As the diagnosis was inconclusive, he underwent a uniportal thoracoscopic procedure under single lung ventilation. The incision was placed in the 6th intercostal space between the anterior and posterior axillary lines. A wound protector was inserted, followed by a 30-degree telescope. A glistening white membrane with minimal purulent fluid and a left lower lobe cavitary lesion communicating with the pleural cavity, and a significantly diseased lung in the form of nodular and infiltrative lesions, were discovered intraoperatively (Figure 2 A).
Figure 1
A – Preoperative chest X-ray with a completely collapsed left lung. B – CT thorax showing cavitary lesion in the left lower lobe with bronchopleural communication and membranous structure
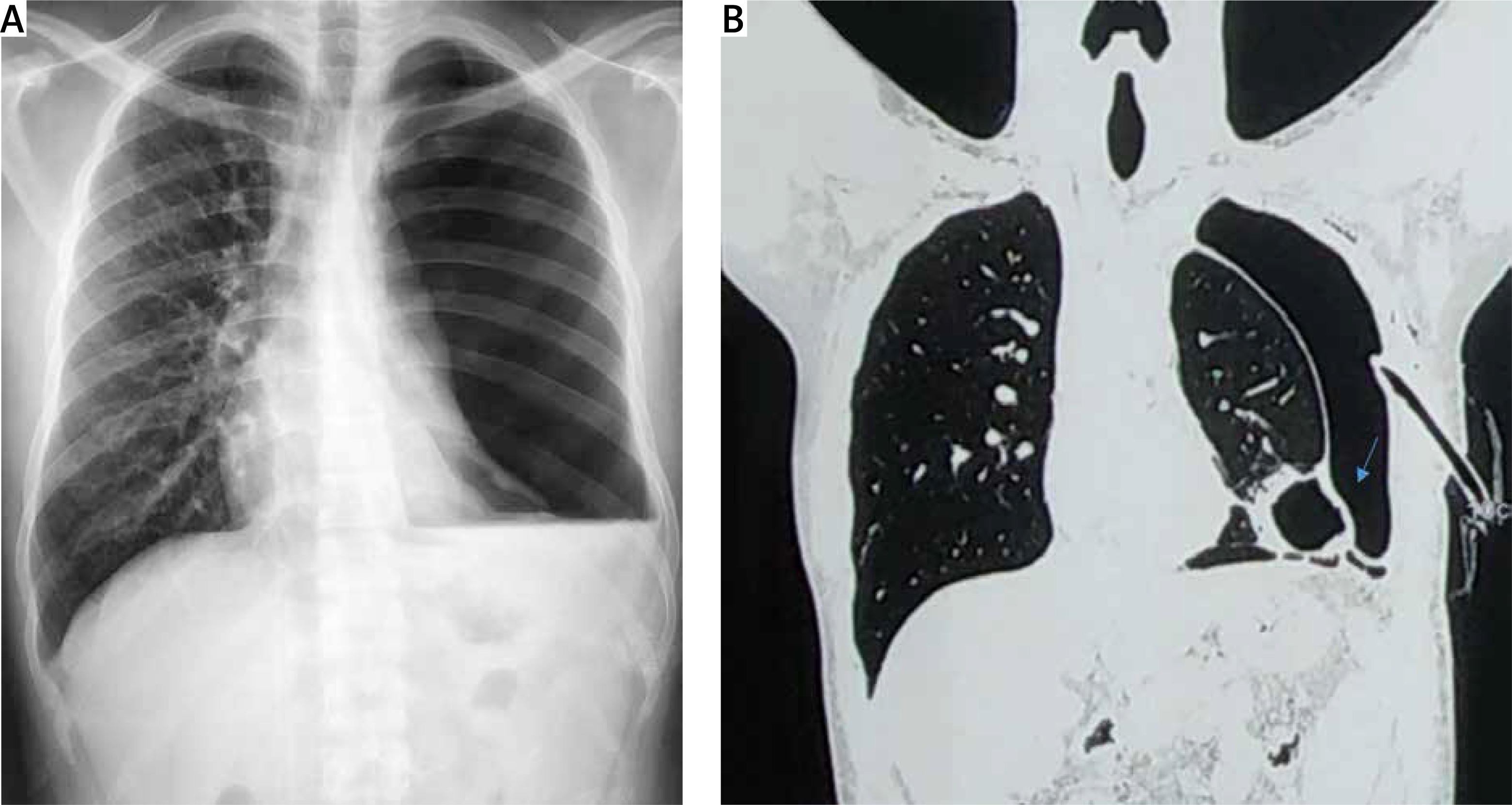
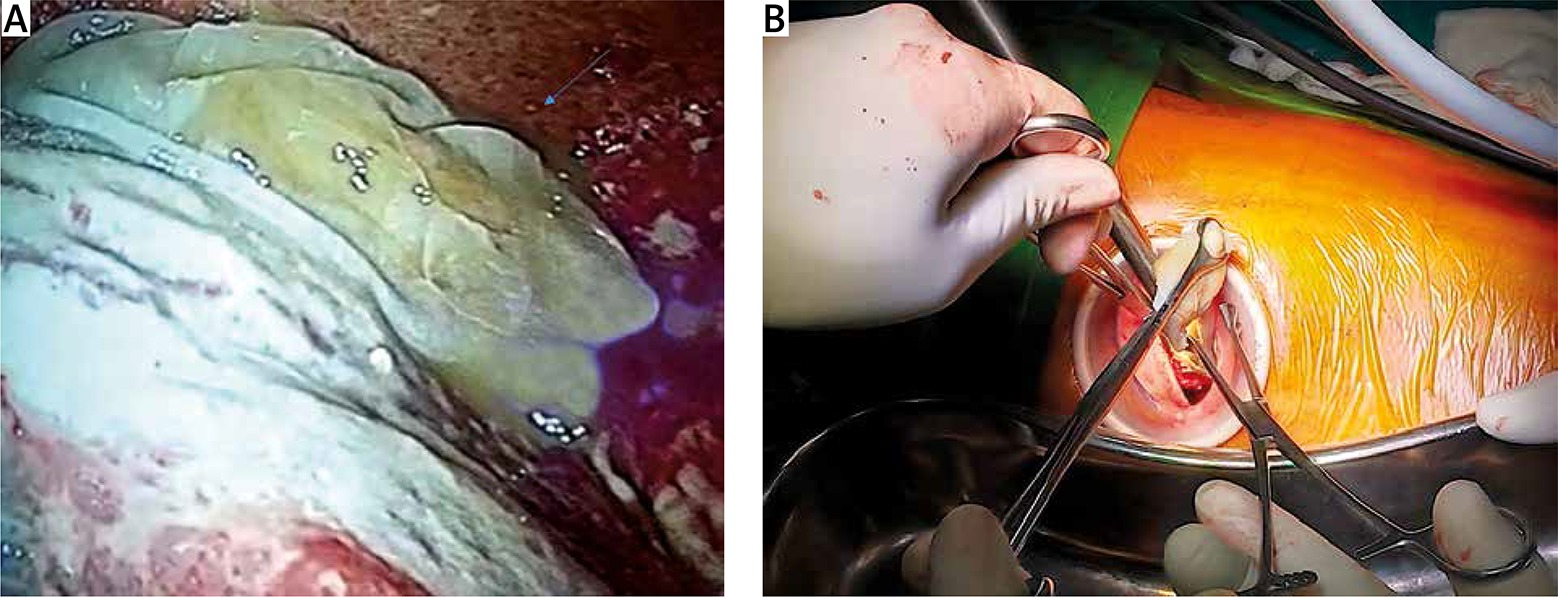
Figure 2
A – Ruptured hydatid cyst in the pleural cavity with diseased lung. B – Uniportal thoracoscopic approach for removal of hydatid cyst
The ruptured membrane, which appeared to be a hydatid cyst, was removed with sponge holding forceps (Figure 2 B) and confirmed histopathologically. Evacuated pleural fluid sent for analysis showed elevated adenosine deaminase (ADA) level and positive Ziehl-Neelsen staining for Mycobacterium tuberculosis, while pleural biopsy did not detect any granulomatous infection. The broncho-pleural fistula was closed with nonabsorbable suture, the cavity obliterated, and decortication done; however, the lung inflated minimally. A single chest tube was placed from the separate site and connected to a dry valve Sinapi chest drainage (Sinapi Biomedical, Stellenbosch, Republic of South Africa) system with a pressure of 2 kPa. The wound was closed in layers. The patient’s postoperative chest X-ray showed partial lung expansion compared to the preoperative chest X-ray. Persistent air leaks persisted in the postoperative period. On the 12th postoperative day (POD), as the drain subsided (below 50 ml), the chest tube was connected to a portable drainage system belonging to the same manufacturer, with a mechanism like that of the Heimlich valve and the patient was discharged. He was instructed to perform both passive and active breathing exercises and was followed up after 21 days. At his follow-up visit, he was asymptomatic, and his chest X-ray showed a better-expanded lung than on the day of discharge. As there was no drainage, irrespective of the air leak, the chest tube was removed.
Following removal of the chest tube, the lung did not collapse, which was confirmed by repeated chest X-ray after 6 and 24 hours. During a follow-up visit in the second and third months, the patient was asymptomatic with a small pneumothorax of 2 cm (Figure 3). However, the lung did not expand completely, but the patient did well. He received albendazole 15 mg/kg/day for 3 months and antitubercular therapy (ATT) according to the National Tuberculosis Elimination Programme for 6 months from the second and third POD, respectively.

Hydatid disease and PTB are common diseases present in our country. Common in both are unhygienic practices and low socioeconomic status. Transmission of hydatid cyst is via the fecal-oral route to humans from animal hosts, including dogs and sheep. The liver is the most common site, accounting for 60–70%, while the lungs are the second most common organ involved, with a higher predilection for the right lower lobe [4]. Cysts are usually solitary and unilateral in distribution, while bilateral involvement and multiple cysts are not uncommon, seen in 20% and 30% of cases, respectively [5]. The term complicated cyst includes hydatid cysts with pleural involvement and the associated infection [3]. A complicated cyst caused by a rupture can be either spontaneous or traumatic [3]. Presentation is variable, depending on the nature of the perforation and overlap of clinical manifestation of PTB, which was typical in our case. In our case study, a chest X-ray revealed pneumothorax; however, a CT thorax showed a cavitary lesion in the left lower lobe with a membranous structure that was confirmed thoracoscopically as well following a histopathological examination. The following immune mechanism explains the masking of clinical presentation.
The immune response in PTB controlled by CD4+Th1 cells is mediated by the cytokines interleukin 12, tumor necrosis factor-α and interferon-γ, while in hydatid disease, the immune response controlled by CD4+Th2 cells is mediated by the cytokines interleukin 4, 5 and 13. As a result, immune responses are antagonistic [1]. Thus, hydatid disease’s predominant Th2 response downregulates the Th1 response, creating an anti-inflammatory environment intensifying PTB and masking clinically early manifestations of hydatid disease in patients with respiratory infections [1].
Surgical intervention is the treatment of choice for ruptured hydatid cysts, and albendazole 15 mg/kg/day is the recommended drug in the postoperative phase for 3–6 months to prevent a recurrence [5]. The patient in the case study received albendazole for 3 months, and no recurrence was observed on follow-up visits. ATT recommended in PTB is scheduled as per National Tuberculosis Elimination Programme guidelines. ATT was prescribed based on intraoperative clinical finding, radiological findings, elevated ADA and positive pleural pus for Mycobacterium tuberculosis.
Persistent air leak is the most common complication seen in the tubercular lung with inadequate lung expansion secondary to alveopleural or bronchopleural fistula (BPF) and its management in the postoperative phase is challenging [6]. In our case study, despite the closure of BPF, air leaks persisted, and the lung did not seem to expand. The probable reason was the extensively diseased lung secondary to tuberculosis resulting in persistent air leak, affecting lung expansion. Initially, a dry valved Sinapi chest drainage system with pressure 2 kPa was placed for 12 days, later was substituted with a portable chest drainage system for approximately 21 days with a mechanism similar to that of a Heimlich valve, and was later discontinued once the drainage was almost nil, irrespective of the presence of air leaks. During the 21-day interval, adhesions that formed in various areas of the pleural space prevented enlargement of the pneumothorax, allowing the lung to expand [7].









