
The simultaneous kissing stents technique (SKST) serves as a strategic bailout intervention for the management of intricate bifurcation lesions, particularly those involving the left main coronary artery (LMCA) [1, 2]. The treatment of such lesions via percutaneous coronary intervention (PCI) is fraught with challenges, given their association with heightened procedural risks and a markedly diminished therapeutic success rate [3]. We present a clinical case involving a patient who presented with an acute myocardial infarction (AMI) complicated by cardiogenic shock (CS) and subsequently underwent PCI of the left main coronary artery using the SKST, supported by the Impella CP device.
A 68-year-old male patient was admitted to our department from a remote hospital due to AMI. Before admission, he had experienced out-of-hospital cardiac arrest due to ventricular fibrillation. On arrival, he presented with symptoms of cardiogenic shock and required vasopressor infusion. Coronary angiography revealed multivessel disease, including left main (Medina 1, 1, 1) (Figure 1 A), combined with a very low left ventricle ejection fraction (EF) of 10% and moderate to severe mitral regurgitation. He was deemed eligible for high-risk PCI by the onsite immediate Heart Team.
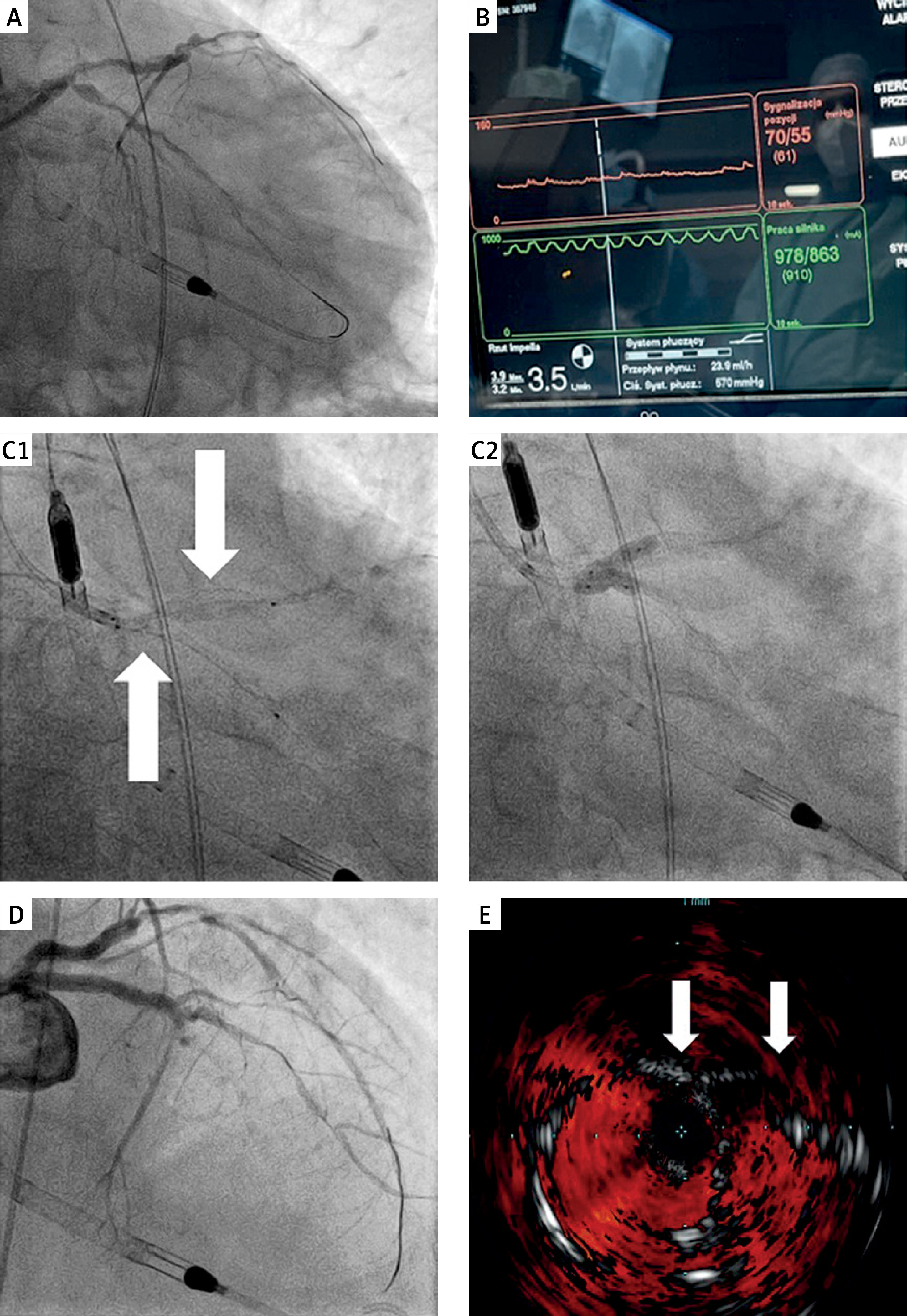
Figure 1
A – Left coronary artery (LCA) angiography. B – Pressure flat curve (laminar flow) on Impella CP monitor during revascularization. C1 – Kissing stents in left main coronary artery (LM)/left anterior descending artery (LAD) and LM/circumflex branch of left coronary artery (Cx) after implantation (top arrow: LM/LAD, bottom arrow: LM/Cx). C2 – Inflated kissing balloons in LM/LAD and LM/Cx. D – Final angiographic result of percutaneous coronary intervention of LCA. E – Double-barrel stents on intravascular ultrasound (arrows)
The Impella CP device was routinely inserted through the left common femoral artery. PCI of the left main (LM), left anterior descending (LAD), and left circumflex (LCx) arteries was performed from the right radial access.
After guidewire passage to the LAD and Cx, the patient was entirely dependent on Impella CP flow (Figure 1 B) and developed several episodes of ventricular tachycardia (VT) and ventricular fibrillation (VF) requiring urgent defibrillation. Balloon predilation of the LM/LAD and LM/Cx led to the same result, and the patient developed pulmonary oedema requiring urgent noninvasive ventilation (BiPAP).
Nonetheless, two drug-eluting stents were implanted simultaneously: LM to LAD 3.5 × 30 mm and LM to Cx 3.0 × 38 mm, both with protrusion into the aorta (Figure 1 C1). After implantation of the stents, the patient’s blood pressure rose to 150/90 mm Hg. Both stents were post-dilated at 16–20 atm using two 3.5 × 15 mm noncompliant balloons (NCB) and two 4.0 × 12 mm NCB in the “kissing balloon” technique (Figure 1 C). The result of the final angiography was optimal (Figure 1 D), and the procedure was guided by intravascular ultrasound, showing good apposition of the stents and a double-barrelled left main (Figure 1 E). The vasopressors were stopped during the procedure, and the Impella CP was successfully weaned and removed due to significant hemodynamic improvement of the patient. The echocardiography showed an immediate improvement in EF of up to 20%. The post-procedural period was uneventful, and after 3 days, the patient was transferred to another hospital for further treatment.
The SKST was selected as a bailout strategy in this highly unstable patient. Despite the very high risk of PCI and the patient’s critical condition, the use of the SKST yielded effective myocardial reperfusion. Disadvantages of such a strategy may include excessive metal burden in the proximal LM, which may limit future reintervention options and possibly increase the risk of restenosis or stent thrombosis. However, the literature regarding emergency PCI involving SKST in conjunction with left ventricular assist devices remains limited, underscoring the need for further research.







