
Introduction
Surgical site infection (SSI) is one of the most common causes of prolonged hospital stay in the post-surgery period [1]. SSIs contribute to major post-surgery complications in patients undergoing coronary artery bypass graft surgery [2]. Multiple causes have been attributed to the occurrence of SSIs in post-surgery patients. The type of suture material for skin closure has been reported to influence postoperative wound complications [3].
Patients undergoing coronary artery bypass graft surgery constitute a large population of patients with anatomically similar incisions created under similar circumstances.
Aim
Our study aimed at analysing and comparing rates of SSIs at the sternotomy sites based on the material used for sternal closure with special emphasis on presence of risk factors such as diabetes (glycated haemoglobin (HbA1c) > 9) and obesity in the 2 respective groups.
Material and methods
This is a retrospective observational study. The data of all patients who underwent coronary artery bypass surgery at our centre from May 2016 to April 2018 were collected retrospectively.
Standardized anaesthetic and surgical procedures were applied in all cases. The antibiotic policy was as mentioned below. Skin preparation included pre-operative bathing with soap and hair removal by means of clipping. In the operating room, directly before the onset of the surgical procedure, the skin preparation was performed using antiseptic solution. Draping followed no sooner than 3 minutes after the last skin preparation. All patients underwent an operation through a full sternotomy.
A total of 864 patients were included in the study. The patients were grouped into 2 groups depending on the sternal wound closure strategy used. One group comprised the patients in whom polyamide sutures were used for skin closure, while the other group comprised patients in whom skin staples were used for skin closure. Incidence of sternal wound SSIs in both groups was noted. Co-morbid conditions such as diabetes mellitus (with HbA1c > 9) and obesity (body mass index (BMI) > 30 kg/m2) were noted and analysed as contributory factors for SSIs. SSIs were categorized into subgroups, namely local erythema, induration, discharge, wound dehiscence. Deep sternal wound infections were excluded from the study. Patients who developed leg wound were excluded from the study. The results of the study were evaluated by Fisher’s two-tailed test and an association was assessed.
Our antibiotic policy
As an institutional policy, at our institute patients are administered a shot of intravenous antibiotic (Inj ceftazidime and Inj amikacin) pre-operatively just before anaesthetic induction. Intravenous antibiotics are continued for a period of 3 days after surgery. In our opinion continuing antibiotics for a period of 72 hours after surgery has reduced incidence of post-operative pneumonia and other hospital acquired infections with rare occurrence of Clostridium difficile infection in our patients.
Results
The 864 patients who were considered for the study were divided into 2 groups. Group A comprised patients in whom sternal wound closure was done by means of a stapler, while group B comprised patients in whom polyamide sutures were used. The mean age of patients in group A was 63.2 ±9.4 years, while that in group B was 64.1 years ±8.9 years, which were comparable. The total incidence of SSIs in sternal wound was 62 (7.17%) patients.
Group A comprised 432 patients out of whom 42 (9.72%) had sternal wound SSIs. Group B comprised the other 432 patients of whom only 20 (4.62%) developed sternal wound SSIs. Co-morbid conditions were analysed in each group. Group A included 64 (14.8%) patients with diabetes (HbA1c > 9) of whom 22 (34.3%) developed sternal wound SSIs. Obesity (BMI > 30 kg/m2) was present in 28 (6.48%) patients, of whom 6 (21.8%) developed sternal wound SSIs. Both diabetes and obesity together were present in 22 (5.09%) of the patients, of whom 16 (72.72%) developed sternal wound SSIs. Group B included 56 (12.96%) patients with diabetes (HbA1c > 9) of whom 6 (10.71%) developed sternal wound SSIs. Obesity (BMI > 30 kg/m2) was present in 26 (6.01%) patients, of whom 4 (15.38%) developed sternal wound SSIs.Both diabetes and obesity together were present in 24 (5.55%) of the patients, of whom 4 (66.67%) patients developed sternal wound SSIs, as summarised in Table I.
Table I
Incidence of sternal wound SSIs in patients
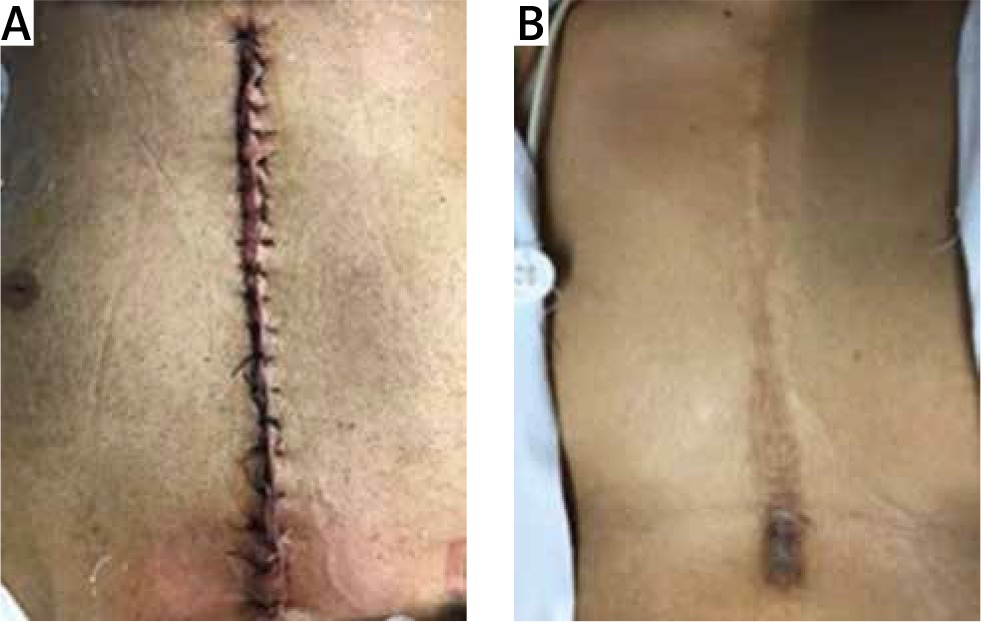
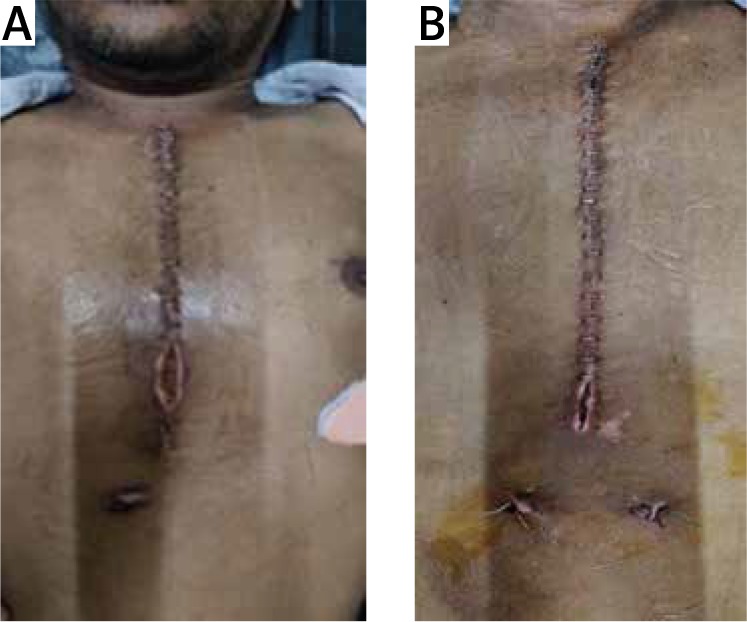
SSIs were classified into further subgroups of local erythema (Figures 1 A, B), induration, discharge, wound dehiscence (Figures 2 A, B), as shown in Table II. Patients who developed deep sternal wound infections were rejected and hence excluded from the study.
Discussion
Though the type of suture material is a contributory factor for SSIs, there are a few studies that have failed to show the association [3, 4].
Surgical staples for skin closure have gained popularity in cases where rapid wound closure is needed or when operating time is of concern and when cosmetic closure is not an important issue. The potential benefits of surgical staples is that they may facilitate wound healing by everting the wound edges but in general are poorly tolerated and require staple removal instruments and tend to leave railroad track scars. Staples are frequently used nowadays in cardiac surgery for sternotomy wound closure.
Though the use of staplers to close skin has emerged in surgical practice, situations where tension across the dermis at margins is to be maintained, conventional polyamide skin sutures showed superiority [5]. In spite of tight closure of the subcutaneous layer with absorbable polyglactin sutures in patients with risk factors such as obesity and associated DM, strength and tension at skin level are important factors to prevent SSI.
The reported incidence of sternal wound infection has ranged from 1.2% to 9% [6–8]. The total incidence of sternal wound SSIs was 7.17% in our study. However, the incidence of sternal wound SSIs in the stapler group (9.72%) was higher than the polyamide suture group.
A further subgroup analysis on the basis of the co-morbid conditions present in the patients was done. It was observed that in the diabetic patient group, incidence of sternal wound SSIs in the polyamide suture group (10.71%) was significantly lower (p = 0.0023) than the stapler group (34%).
Similarly in patients with diabetes and obesity, it was observed that the incidence of sternal wound SSIs in the polyamide suture group (16.66%) was significantly lower (p = 0.003) than the stapler group (72.72%).
The obesity group did not show any significant difference (p = 0.729) in the incidence of sternal wound SSIs between the polyamide suture group (11.11%) and the stapler group (21.42%).
Johnson et al. [9] in 1997 prospectively compared 242 patients with sternal and saphenous vein harvest wounds. These wounds were closed half way with staples and the other half with intradermal sutures. Wound infection rates were found to be similar using either staples or intradermal sutures in chest and leg wound closure. There was, however, a significantly higher complication rate (defined as drainage, erythema, separation, necrosis, seroma or infection) using staple closure for either chest or leg wounds. Sixty-two percent of patients preferred leg closure with sutures compared to 20% preferring staples.
Angelini et al. [10] in 1984 performed a prospective randomized controlled trial separating 113 patients into four groups. The leg wounds were either closed with continuous polyamide vertical mattress suture (Ethicon), continuous subcuticular absorbable suture (Dexon), metal skin staples (Premium) or adhesive sutureless skin closure material (Op-site). The use of continuous subcuticular suture (Dexon) resulted in significantly less wound infection when compared to any of the other modalities.
Chughtai et al. [11] in 2000 performed a prospective, randomized, controlled trial, comparing outcomes between subcuticular suture technique and skin stapling technique for closure of sternal and leg incisions in 162 CABG patients. There was a tendency towards increased wound infections when staples were used for both chest and leg incision closure. Cosmetic outcomes were similar but the staples cost three times as much as the sutures.
All patients who were diagnosed with sternal wound SSIs at our institute were subjected to the same management protocol. A wound swab was taken from the sternal wound and appropriate antibiotics were started as per the sensitivity reports. The patients were then subjected to local debridement of the wound until all slough and necrotic tissue were excised. Patients were then subjected to secondary closure of the sternal wound with or without the use of vacuum-assisted drainage devices (as per the individual preference of the surgeon).
Though our study emphasised and analysed diabetes and obesity, as contributory factors [12] to sternal wound SSIs, it did not address other contributory factors such as presence of drain, immune status, etc. The study does not take into account the cost-benefit comparison between staplers and polyamide sutures.
Conclusions
The surgical scar remains the only visible evidence of the surgeon’s skill, and, not infrequently, all of his efforts are judged on its final appearance. With the host factors controlled by pairing staples and sutures in each patient, we observed a significantly lower incidence of total wound complications with suture closure than with staple closure. We conclude that sutured polyamide skin closure for chest wounds is superior to stapler closure in patients with diabetes (HBA1c > 9) and obesity (BMI > 30 kg/m2).









