
Introduction
Despite inconclusive and conflicting results of trials and meta-analyses assessing aspiration thrombectomy in ST-segment elevation myocardial infarction (STEMI), trends toward reduced mortality were observed in the high thrombus burden subgroup [1–3]. With a large thrombus being one of the strongest predictors of the no flow phenomenon, manual thromboaspiration remains an effective method of its prevention, especially in patients who cannot undergo a staged procedure after IIB/IIIA inhibitor administration because satisfactory reperfusion has not been achieved during the initial intervention [4–8]. Since standard monorail coronary aspiration devices are often ineffective in the case of a large thrombus, guide extension catheters have been used for clot extraction. Their bigger lumen comes at a cost of worse trackability and a higher risk of artery dissection [9].
We present four transradial procedures, in which a neurointerventional catheter was utilized to remove an otherwise unextractable or inaccessible clot. In all cases, successful aspiration with a Sofia catheter was performed without any procedural complications (e.g., dissection, distal embolization, stroke).
Case reports
Case 1
A 42-year-old man with a history of hypertension was admitted due to retrosternal pain of 4-hour duration with inferior STEMI diagnosis. Angiography revealed tight stenosis with a large clot in the mid-segment of the dominant right coronary artery (RCA). Intracoronary eptifibatide was administered and aspiration thrombectomy with a 6 French Pronto catheter (Teleflex) was attempted without success due to the device’s inability to capture the clot. The 5 French Sofia, a neurointerventional aspiration catheter (Microvention, Terumo), was then used, successfully removing the clot. A drug-eluting stent was implanted with TIMI 3 (Thrombolysis In Myocardial Infarction) flow maintained.
Case 2
A 59-year-old man with a history of hypertension and smoking was admitted due to 3.5 h long chest pain and signs of inferior STEMI in electrocardiography (ECG). The dominant RCA was occluded just beneath the origin of the acute marginal artery with a large clot visible (Figure 1 A). Following an intracoronary eptifibatide bolus injection, several passes with a 6 French aspiration thrombectomy catheter Export AP (Medtronic) failed to retrieve macroscopic material but allowed for the visualization of a large thrombus filling the ectatic distal segment up to the bifurcation of the RCA (Figure 1 B). The 5 French Sofia was then utilized with a wireless passage technique, successfully removing the clot and restoring TIMI 3 flow (Figures 1 C, D, 2 A–D). A drug-eluting stent was implanted without flow deterioration.
Figure 1
Aspiration thrombectomy in patient 2. A – Distal RCA occlusion with a large clot. B – Partial recanalization after suction with Export AP aspiration catheter, showing a long thrombus filling the distal RCA up to its bifurcation. C – Wireless aspiration with the Sofia reaching RCA bifurcation (arrow points to the tip of the Sofia catheter). D – The result of the aspiration with the Sofia catheter.

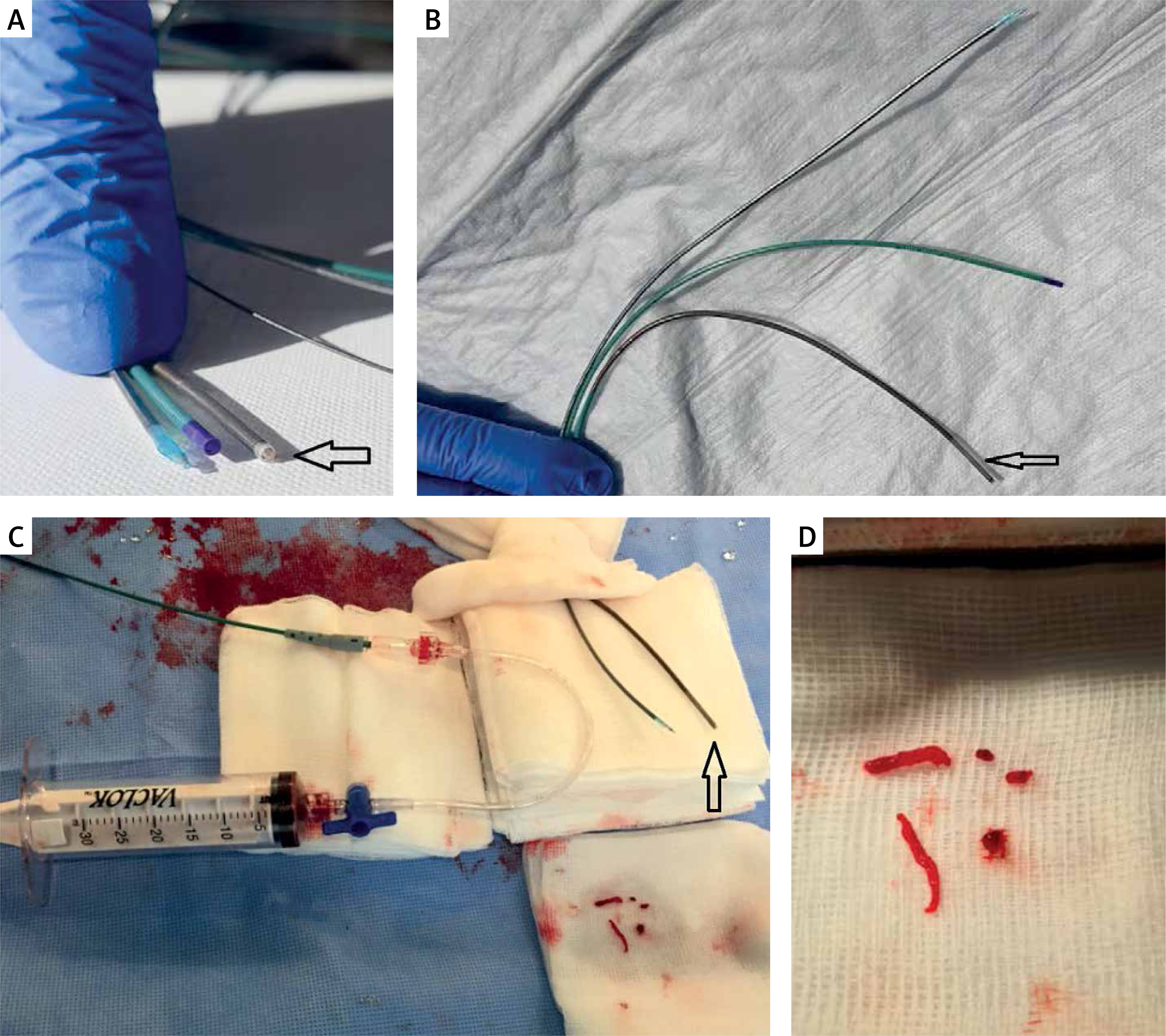
Figure 2
Sofia vs. standard coronary catheters used for clot aspiration, Sofia suction setup, and the thrombus retrieved in patient 2. A – From the left: coronary aspiration catheter Export AP, Telescope guide extension catheter, and Sofia neurointerventional catheter (arrow). B – From the top: Export AP, Telescope, and Sofia (arrow); the stiffness of each catheter can be appreciated in the vertical position; C – Typical setup for wireless aspiration with Sofia catheter (arrow), using a 30 ml vacuum locking syringe; D – Clots removed in patient 2 with the Sofia catheter
Case 3
A 65-year-old patient with a history of hypertension and prior myocardial infarction with stent implantation in the RCA 6 years before was admitted with inferior STEMI with prolonged chest pain of 9 hours’ duration. The dominant RCA was occluded in the distal segment, inside the previously implanted stent, with a large clot visible. Aspiration with a 6 French GuideLiner (Teleflex) failed and dislodged the thrombus further downstream, where it could not be reached. GuideLiner balloon-assisted tracking was waived for fear of distal embolization. The Sofia catheter was advanced to the place of occlusion and the bulk of the clot was aspirated, with only a small residual thrombus left. Finally, a drug-eluting stent was deployed, with TIMI 3 flow maintained.
Case 4
A 57-year-old patient with a history of hypertension, prior myocardial infarction and bare metal stent implantation on two different occasions (in RCA 17 years before and in the left anterior descending artery 11 years before) was admitted due to inferior STEMI with 2 h long chest pain. Urgent coronary angiography showed distal occlusion of the RCA at the previously implanted stent. Eptifibatide was administered and aspiration thrombectomy attempted with a 6 French Export AP catheter, followed by a guide extension catheter GuideLiner. Both devices reached the target zone but failed to extract the thrombus, with the GuideLiner losing the retracted thrombus in the mid-RCA. The Sofia catheter was then advanced and managed to evacuate the clot, with TIMI 3 flow restored. Finally, a drug-eluting stent was deployed in the distal segment with a good immediate result.
Discussion
Neurointerventional tools have not been routinely employed in coronary procedures. There are only anecdotal reports of successful removal of a refractory clot with a stent retriever in the setting of acute myocardial infarction [10–12]. Building on our experience in stroke thrombectomy, we decided to reinvent neuroradiological devices for coronary interventions, much the same as the coronary armamentarium had inspired the invasive management of intracranial pathologies. Having tested several aspiration thrombectomy catheters in the tortuous intracranial vessels, we chose the 5 and 6 French Sofia (Microvention, Terumo) as one of our favorite intermediate catheters for ischemic stroke treatment. The device we used in STEMI treatment is a 5 French, 125 cm Sofia catheter, with a soft, atraumatic tip and 17 cm long, hydrophilic, flexible distal segment (Figures 2 A, B). It is extremely trackable, obviating even the use of a guidewire, with a wireless SNAKE technique (Sofia Non-wire Advancement techniKe) often used for its advancement in the cerebral circulation [13]. Not only does it provide a much larger extraction lumen than conventional coronary aspiration catheters (approximately 70% bigger cross-sectional area), but being less rigid and more hydrophilic, it also offers much better trackability. Theoretically, guide extension catheters such as GuideLiner (Teleflex) have a slightly bigger aspiration lumen; however, with their distal-only collar, they require guidewire for navigation, which takes some of the extraction area. Despite the inner diameter comparable to Sofia, guide extension catheters are stiffer and less hydrophilic, resulting in worse trackability and bend negotiation (Table I). Other nominally 5 French catheters used for intracranial aspiration such as JET D (Penumbra) and AXS Catalyst 5 (Stryker Neurovascular) are not compatible with 6 French coronary guiding catheters due to their bigger proximal size. In our experience, Sofia seems to offer the best of both worlds, with a well-balanced trade-off between a large clot capture potential and excellent trackability.
Table I
Six French guiding catheter-compatible devices that can be used for coronary clot aspiration
For coronary clot removal with guide extension catheters and Sofia, we adopted the ADAPT stroke thrombectomy technique (A Direct Aspiration First Pass Technique), whereby extraction catheters are advanced with active suction until blood inflow is stopped, and then left in place for 2–3 min for efficient thrombus capture, with slow catheter retrieval performed under continuous negative pressure. This technique is used in stroke treatment to avoid embolization to new territory during thrombectomy. The large extraction lumen of the Sofia, which enables firm clot capture, often with its almost complete ‘internalization’, may potentially reduce the risk of its peripheral embolization and stroke during catheter retrieval, which plagued coronary thrombectomy trials [1–3]. Moreover, the continuous lumen of the Sofia should be able to generate greater suction power than the distal collar of guide extension catheters (Figures 2 C, D). Friction of the guidewire in a guide extension catheter during the device retrieval may detach the captured clot from the catheter tip, which is not the case with the SNAKE wireless passage that can be used with the Sofia [13]. Although we did not assess the histological composition of the retrieved clots, in our case, the Sofia seemed to have worked both for fresh (2 h) and older clots (9 h), despite having been designed for removal of thrombi occluding the intracranial arteries, where embolic events are more often the cause of ischemia.
In cases in which coronary aspiration catheters had been used as first-line devices, we performed thrombectomy with the Sofia using original 30 ml vacuum-locking syringes provided with the former (Figure 2 C). When the use of the Sofia had been preceded only by GuideLiner aspiration, we employed 60 ml vacuum-locking syringes that we use for clot suction in stroke cases.
Both guide extension catheter-related and aspiration catheter-induced coronary artery dissections have been reported, while the Sofia so far has had a relatively good track record in more tortuous and thinner intracranial arteries [9, 14]. However, as with any endovascular device, caution must be exercised during the Sofia’s coronary application, especially as it is an off-label use. Despite the large extraction lumen and excellent trackability, the risk of systemic embolism and coronary dissection should be considered.
In the case of a refractory clot, the exchange of a 6 French aspiration catheter or guide extension catheter for a 7 or 8 French device is an option, but it often requires femoral crossover with the risk of bleeding during IIB/IIIA inhibitor infusion typically administered in the case of a high thrombotic burden. It also prolongs time to reperfusion. Moreover, it should be kept in mind that access to the distal segments of the coronary arteries is very limited for 7 and 8 French devices.
In addition to manual thrombectomy devices, mechanical aspiration catheters such as the AngioJet (Possis) and X-Sizer (ev3) have been utilized in coronary circulation. However, studies assessing the benefits of their use in myocardial infarction were inconclusive.
The mixed results of coronary thrombectomy trials have driven further research into the design of aspiration devices and techniques. The conception of sustained mechanical aspiration with the CAT Rx catheter powered by the Penumbra ENGINE (Penumbra), engineered on the basis of the company’s neuro-tracking technology, was recently tested in the CHEETAH clinical study. The results of the trial were presented at the Transcatheter Cardiovascular Therapeutics conference in November 2021 [15]. The assumption of greater efficacy is based on the simulations showing that in the case of manual aspiration, the vacuum in a syringe drops off quickly as blood enters. However, despite the enhanced trackability and continuous suction, the CAT Rx’s aspiration lumen is still no better than that of conventional thrombectomy devices used in the coronary circulation.
It may be time to redesign coronary aspiration devices with a catheter escalation or catheter sizing strategy developed. The aspiration portfolio, however, should include large diameter, continuous lumen devices sharing the unique properties of neurointerventional catheters. With a paradigm shift from a one-type-fits-all approach to a wider choice of different catheter types and sizes, interventional cardiologists will be offered an option of a more thrombus-tailored therapy. Given the risk of clot embolization and the no flow phenomenon, the first pass effect should be the ultimate goal of coronary aspiration. Neurointerventional aspiration techniques such as ADAPT, reducing the risk of clot embolization, should also be considered in the coronary circulation. With such a nuanced approach, the place of aspiration thrombectomy in acute myocardial infarction management may need to be reassessed in randomized studies.
Conclusions
Neurointerventional aspiration catheters such as the Sofia appear to be a viable and unsophisticated option for refractory and/or inaccessible clots preventing coronary reperfusion in acute myocardial infarction. Unfortunately, the Sofia is a rather costly device, roughly 3.5 times more expensive than conventional coronary aspiration devices and 1.5 times more than guide extension catheters. Moreover, it should be kept in mind that the Sofia has been approved for interventional stroke treatment, so its use in coronary aspiration is an off-label procedure.







