
A 35-year-old female patient was admitted to the surgical department with abdominal pain and elevated inflammatory markers. Her medical history included colorectal adenocarcinoma with abdominal wall metastases treated with pembrolizumab immunotherapy, and deep venous thrombosis managed with therapeutic doses of low molecular weight heparin (LMWH). A chemotherapy port had been implanted 6 months before admission. Initial computed tomography (CT) of the abdomen revealed a progressive tumor in the ascending colon with abscess-like fluid collections, infiltrating adjacent organs and the abdominal wall. The patient underwent emergency surgery. Post-operative management included empiric antibiotic therapy and vacuum-assisted closure dressings, which resulted in decreased inflammatory parameters and improved general condition. Follow-up CT showed an interloop irregular collection consistent with an abscess, which was deemed inaccessible for percutaneous drainage. Further surgical intervention was considered inappropriate. The imaging also identified pulmonary embolism and a chemotherapy port-related structure extending into the right atrium (Figure 1 A). Transthoracic echocardiography (TTE) confirmed a right atrial mass with imaging characteristics suggestive of thrombosis (Figure 1 B). The patient was maintained on systemic anticoagulation with intravenous unfractionated heparin. Following multidisciplinary discussion at a joint cardiology and cardiothoracic meeting, conservative management with therapeutic doses of LMWH was recommended due to her poor general condition. However, subsequent TTE, performed due to recurring fever and rising inflammatory markers, showed no reduction in the right atrial thrombus size despite therapeutic anticoagulation. Moreover, the mass had extended from the right atrium into the right ventricle (Figure 1 C). Transesophageal echocardiography confirmed the mass’s attachment to the chemotherapy port in the superior vena cava and its extension into both the right atrium and ventricle (Figures 1 D–F). After further cardiothoracic surgical consultation, the team proceeded with minimally invasive thrombus and chemotherapy port removal via right minithoracotomy (Figure 1 G). Bacteriological analysis confirmed an infected thrombus, and targeted antibiotic therapy was initiated. At 2-week follow-up, TTE showed no residual masses in the right heart chambers (Figure 1 F). The patient reported decreased dyspnea and improved overall well-being.
Figure 1
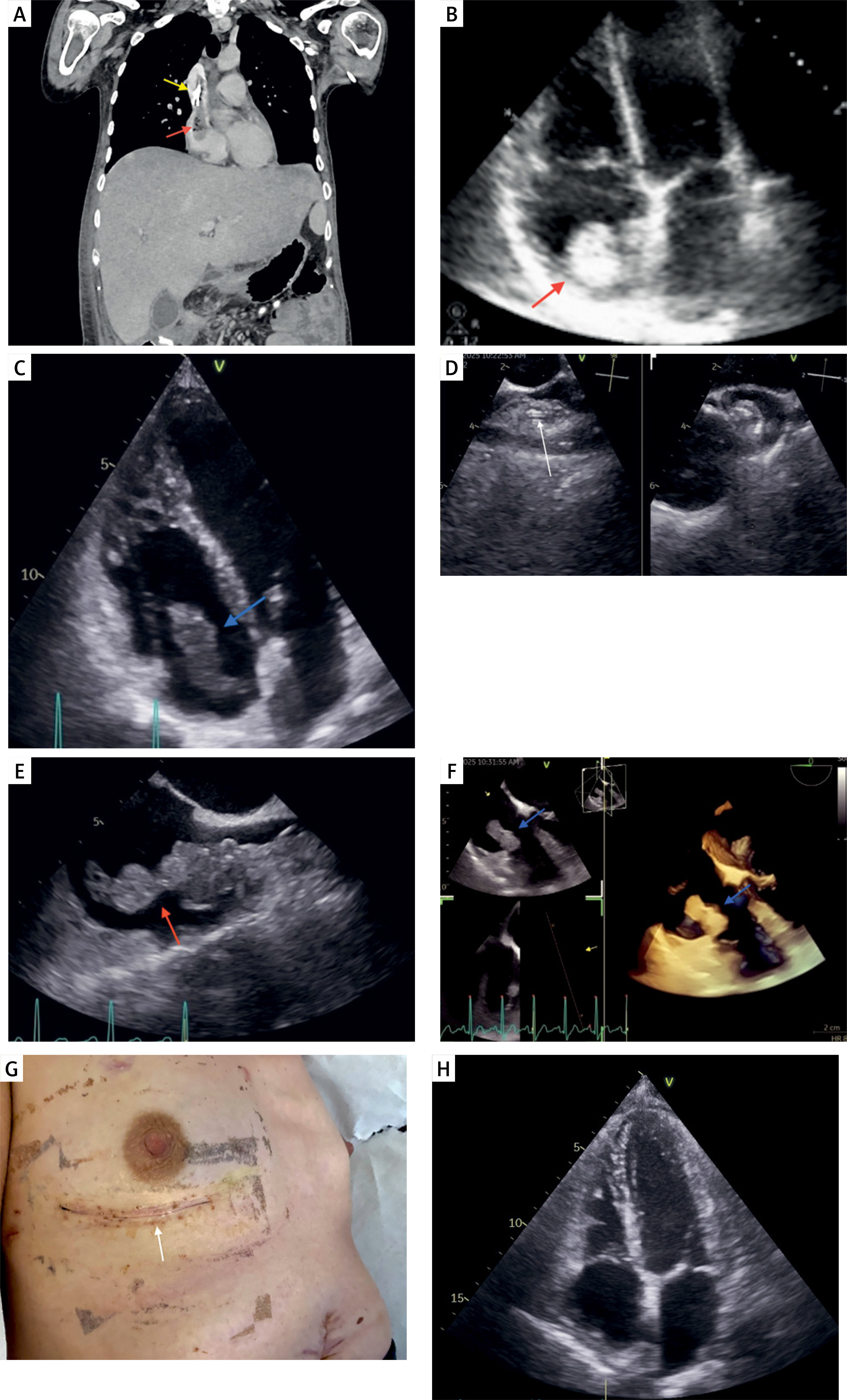
A – Computed tomography demonstrating a thrombotic mass in the right atrium (red arrow) attached to the chemotherapy port (yellow arrow). B – Transthoracic echocardiography showing an echogenic mass in the right atrium (red arrow). C – Follow-up transthoracic echocardiography revealing extension of the thrombotic mass from the right atrium into the right ventricle (blue arrow). D–F – Transesophageal echocardiography showing the chemotherapy port (white arrow) with associated thrombotic masses extending from the superior vena cava into the right atrium (red arrow) and right ventricle (blue arrow) G – Post-operative image showing the right minithoracotomy incision site (white arrow). H – Post-operative transthoracic echocardiography showing no residual masses in the right heart chambers
Cancer patients exhibit an elevated risk of thromboembolic complications, which is further amplified by chemotherapy [1]. While chemotherapy ports provide significant benefits including medication administration, blood sampling, and parenteral nutrition, they may lead to complications such as catheter-related thrombosis [2]. Port-related thrombosis, though relatively uncommon, presents with a spectrum of manifestations ranging from asymptomatic cases to severe hemodynamic compromise, shock, or cardiac arrest secondary to pulmonary embolism. The presence of right heart thrombus in acute pulmonary embolism carries significant prognostic implications and is associated with increased mortality. Thus, echocardiographic detection plays a crucial role in both risk stratification and therapeutic decision-making [3]. Primary treatment options for right heart thrombus include systemic anticoagulation, thrombolytic therapy, and surgical or percutaneous aspiration thrombectomy. Although systemic anticoagulation remains the recommended first-line therapy for hemodynamically stable patients, it may prove inadequate for well-formed, persistent or extensive thrombi, as demonstrated in our case [4]. In this context, thrombus resection via right minithoracotomy represents a minimally invasive alternative to conventional open surgical thrombectomy, offering a particularly advantageous approach for high-risk oncological patients. The possibility of using targeted antibiotic therapy resulted in a decrease in inflammatory markers and enabled the continuation of systemic cancer treatment.







