
A 59-year-old man was referred to our hospital for chest pain he had been experiencing for several hours. The electrocardiogram showed ST-segment elevation in leads II, III, aVF, V4-V6. Emergent coronary angiography (CAG) showed a total occlusion of the proximal right coronary artery (RCA) with multiple calcified coronary artery aneurysms (CAAs) (Figure 1 A). There was no significant lesion of the left coronary artery.
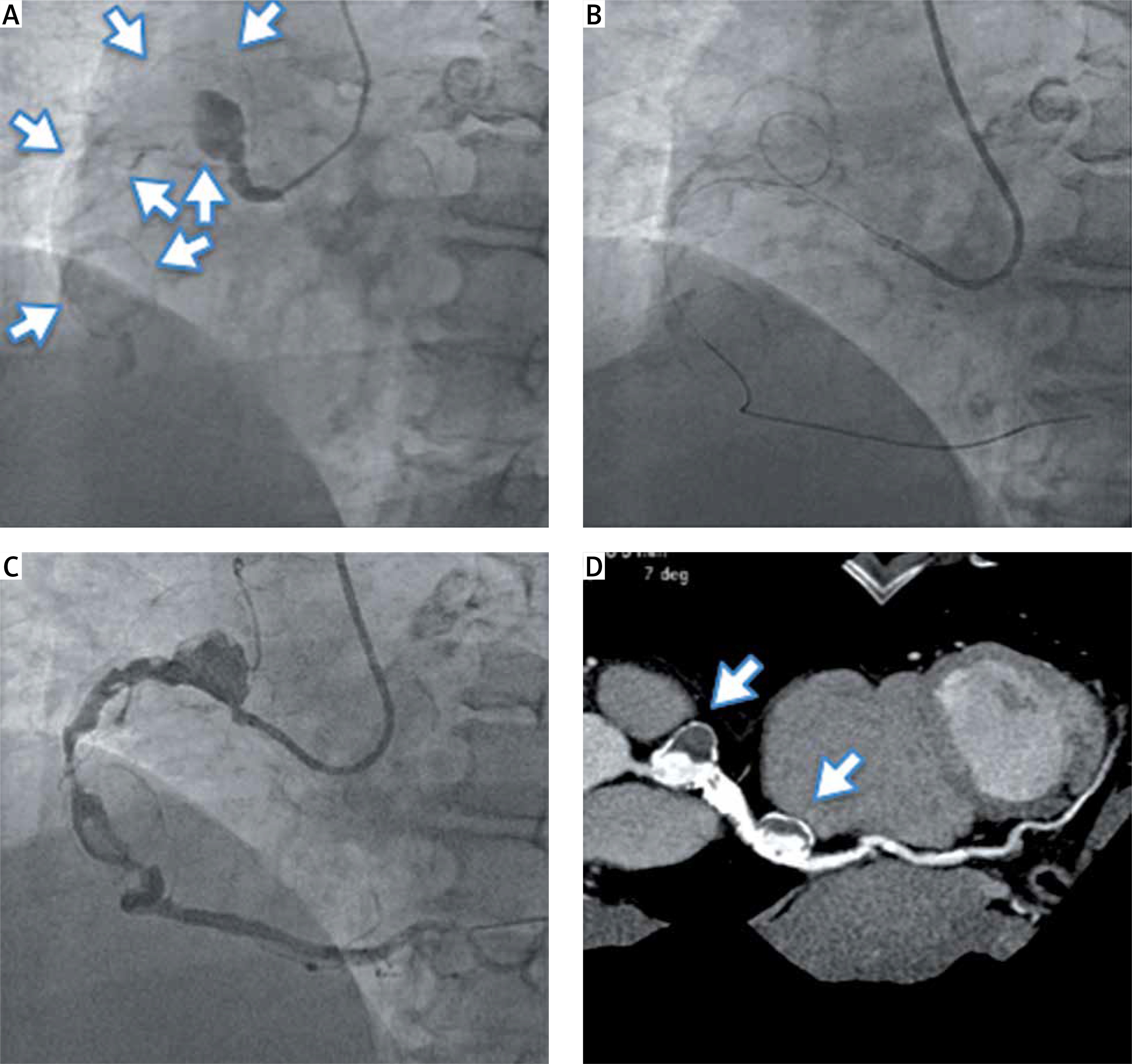
Figure 1
coronary angiography (CAG) before and after percutaneous coronary intervention (PCI), and follow-up computed tomography (CT). A – Right CAG before PCI, white arrows: multiple coronary artery aneurysms, B – right CAG after wire cross, C – right CAG after PCI, D – CT angiography 18 months later, white arrows: multiple coronary artery aneurysms
The RCA was intubated with a 7-Fr Amplatz-left 1.0 guiding catheter (Launcher; Medtronic, USA). A 0.014 guidewire (Runthrough NS Floppy; Terumo, Japan) could not pass through the lesion. We switched to the 0.014 guidewire (Conquest Pro12; Asahi Intecc, Japan). Supported with a microcatheter (Caravel MC; Asahi Intecc, Japan) the guidewire passed through the lesion in a loop (Figure 1 B). Ballooning with a 3.0 × 30 mm catheter (Euphora; Medtronic, USA) was performed with post-dilatation using a 4.0 × 10 mm catheter (Raiden3; Kaneka, Japan). The balloon did not fully expand in the lesion, so stenting was not attempted. We performed thrombectomy using a 7-Fr catheter (ThrombusterIII-GR, Kaneka, Japan) more than 10 times and a large amount of red thrombus was obtained. Although we confirmed TIMI-3 flow after repeating thrombectomy and ballooning, some residual thrombus was still noted on CAG (Figure 1 C). Therefore we decided to administer intracoronary 120,000 units of urokinase. We confirmed resolution of his chest pain and ST-segment elevation, and preserved left ventricle (LV) function. Although we offered low-dose aspirin and warfarin, aspirin was stopped due to minor bleeding 14 months later.
After 18 months coronary computed tomography (CT) was performed to assess patency and morphology of the CAAs (Figure 1 D). Although coronary bypass surgery was offered to him, he refused to undergo surgery.
CAAs are defined as dilatation of coronary artery diameter ≥ 1.5 times its original size and are reported to have an incidence of 0.3–5% in angiographic series [1, 2]. Atherosclerosis is the most common cause of CAAs and other etiologies of CAAs are: congenital, complicated percutaneous coronary intervention (PCI), Kawasaki’s disease, and Marfan syndrome [1]. The cause of CAAs in this case is unknown because the patient does not have any past histories. PCI of an aneurysmal culprit vessel in the setting of acute myocardial infarction (AMI) is associated with lower procedural success and higher incidence of no-reflow and distal embolization [2]. It is difficult to assess the sizing and landing zone of the stent to be deployed at an aneurysmal vessel in consideration of the risk of stent thrombosis and stent migration [2].
Patients who are asymptomatic or have no significant coronary atheromatous disease can be considered good candidates for conservative therapy, the principal goal of which is to prevent formation of any thrombus inside the aneurysm. This goal can be by attained by treating this population of patients with anticoagulation therapy with follow-up every 3 months [3, 4].
In conclusion, the presented case with multiple CAAs causing AMI is rare and the treatment depends on the clinical findings, location, and size of the CAAs. Because primary PCI involving CAAs is challenging, causing difficulties in “wiring” the distal part of the lesion, it might be useful to wire with a loop by using a microcatheter.







