
Introduction
Liver cancer is one of the most common cancers in the world. Liver cancer incidence and mortality are increasing over time. A 2017 report estimated that there were 950,000 new cases and 800,000 deaths from liver cancer, twice as many as in 1990 [1]. Hepatectomy is considered a basic and effective method in the treatment of liver cancer. In 1963, Dr. Ton That Tung introduced the method of hepatectomy called Ton That Tung by controlling the vascular pedicle after cutting the liver parenchyma, thereby limiting complications due to an abnormal state of the liver’s anatomical characteristics [2]. In 1986, Takasaki introduced extrafascial Glissonean dissection [3] to control the Glisson pedicle at the hepatic hilum. This technique had some advantages in hepatectomy including the precise determination of the hepatectomy area, helping to cut the liver safely, limiting the ischemia of the remaining liver parenchyma, reducing blood loss, and avoiding spreading cancer cells to avoid cancer cell proliferation to neighboring lobes during surgery.
This study was conducted to evaluate the results of hepatectomy for hepatocellular carcinoma (HCC) by the combination of extrafascial extrahepatic (Takasaki method) and extrafascial intrahepatic pedicle approaches (Ton That Tung method).
Material and methods
Study design and patients
This longitudinal study was performed at Nghe An General Friendship Hospital, Vietnam from April 2017 to July 2021. Patients were recruited if: 1) they were indicated for hepatectomy to treat hepatocellular cancer by the combination of extrafascial extrahepatic (Takasaki method) and extrafascial intrahepatic pedicle approaches (Ton That Tung method); 2) they and their caregivers agreed to participate in the study. A total of 83 patients were invited to the study during this period. They were followed up for 4 years to assess survivorship after surgery. This study was approved by the institutional review board of Nghe An General Friendship Hospital.
Surgical technique and data collection
The surgical procedure has been described elsewhere [4]. In brief, we used the Takasaki method for extrahepatic extrafascial Glissonean dissection. Then, we used the Ton That Tung hepatectomy method by performing parenchymal transection and intrahepatic division of Glissonean pedicles.
Patient information was collected using a medical record. The information includes age, gender, clinical characteristics, the status of hepatitis and cirrhosis, surgical outcomes, type of liver resection, time of surgery, intraoperative complications, blood loss, length of hospital stay, and survivorship after 4 years of follow-up.
Statistical analysis
Data were analyzed using SPSS 22.0 software (IBM Corp., USA). Descriptive statistics were performed. Overall survival (OS) and disease-free survival (DFS) were described according to clinical characteristics and surgical characteristics, using the log-rank test for comparison. The Kaplan-Meier analysis method was conducted to assess the probability of survival of patients 4 years after surgery. A Cox regression model (proportional hazard model) was used to analyze prognostic factors for the probability of patient survival. P < 0.05 was considered to be statistically significant.
Results
Table 1 shows that of 83 patients with HCC, the mean age was 53.23 ±10.47 years. The majority of them were male (68.7%), having hepatitis B (79.5%), having Child-Pugh grade A (91.6%), and stage IB (67.8%) according to the tumor-node-metastasis (TNM) classification.
Table 1
Demographic and clinical characteristics of hepatocellular carcinoma patients
Table 2 shows that all cases underwent anatomical liver resection, in which minor hepatectomy accounted for 75.9%. The percentage of left and right pedicle control was 14.5% and 72.3%, respectively. Surgical margin in the range 0.5-1 cm was major, which accounted for 43.4%. The average parenchymal transection time was 37.43 ±9.94 minutes, and the average operative time was 158.7 ±53.12 minutes. The volume of blood loss during surgery was 247.32 ±145.15 ml. Some complications were recorded including biliary fistula (3.6%), pleural effusion (26.5%), ascites (16.9%), and postoperative liver failure (1.2%). According to the Clavien-Dindo classification, grade I accounted for the majority with 35%. No patient died during the hospital stay.
Table 2
Surgical characteristics, outcomes and complications among patients
The average postoperative follow-up time was 25.06 ±14.04 (3-53) months. The number of survivors was 61 and 22 patients died during the study period. Overall survival at 1, 2, 3 and 4 years was 88.4%, 76.3%, 69.5% and 56.9%, respectively. The mean time of OS was 40.68 ±2.17 months. Probability of DFS after 1, 2, 3 and 4 years was 67.1%, 56%, 53.1% and 50%, respectively. The mean time of DFS was 32.58 ±2.56 months (Fig. 1).
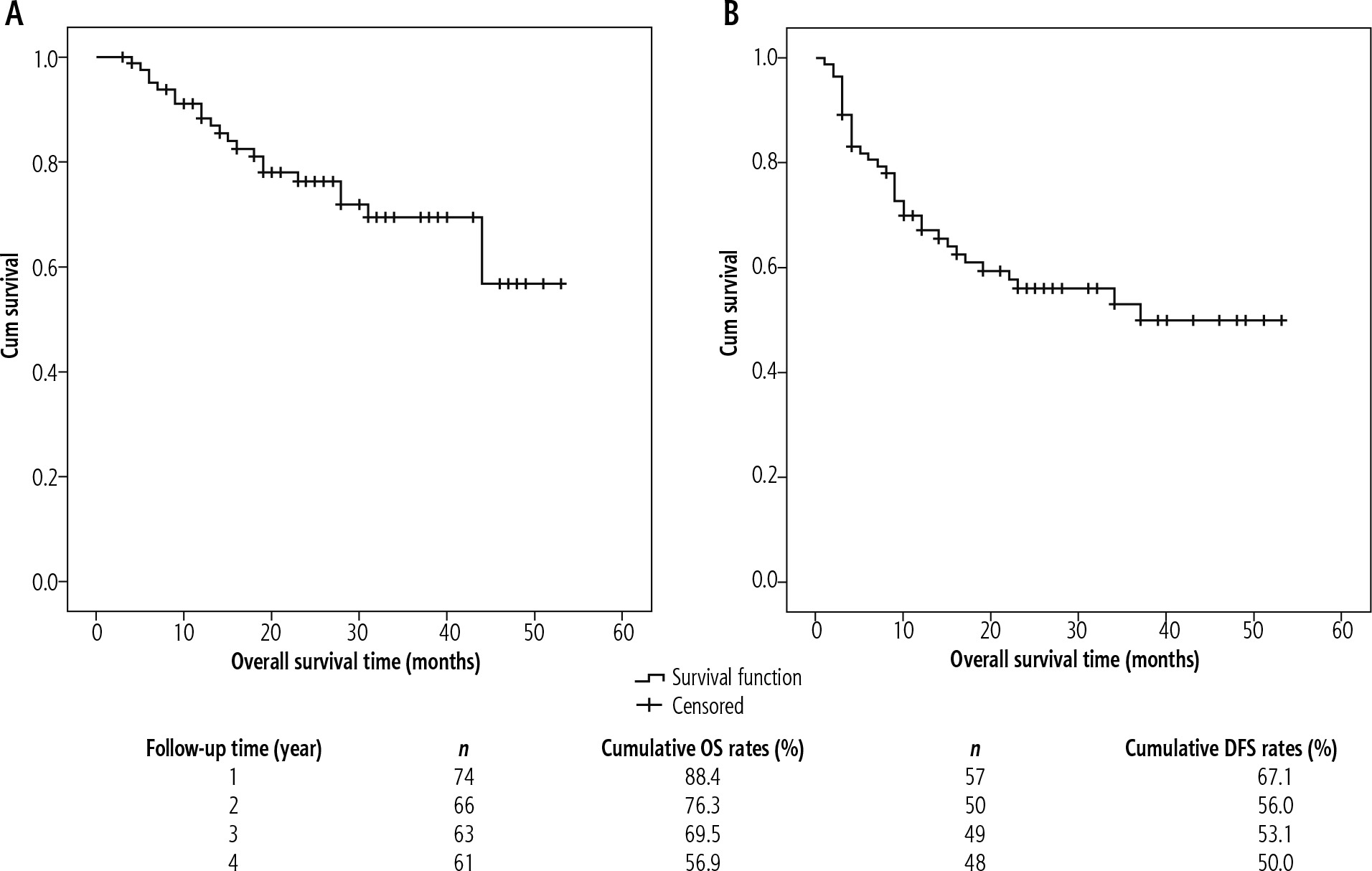
Table 3 shows that tumor size, surgical margin, portal vein tumor thrombosis, and Barcelona Clinic Liver Cancer (BCLC) stage were significantly associated with overall survival (p < 0.05; Table 3), while α-fetoprotein (AFP), tumor size, surgical margin, portal vein tumor thrombosis, and BCLC stage were significantly associated with DFS (p < 0.05; Table 4).
Table 3
Overall and disease-free survival according to different socio-demographic and clinical characteristics
Table 4
Multivariate analysis for overall and disease-free survival
Table 4 shows that surgical margin was an independent prognostic factor for both overall and disease-free survival. Portal vein tumor thrombosis was identified as an independent prognostic factor for OS (HR = 8.843, 95% CI = 2.081-37.574, p = 0.003). Tumor size was an independent prognostic factor for DFS (HR = 0.471, 95% CI = 0.238-0.933, p = 0.031).
Discussion
Selective hepatectomy and anatomical hepatectomy are considered standard techniques for HCC. Ton That Tung improved the technique based on the principle of finding and tying the Glisson pedicle in the liver parenchyma [2]. Takasaki introduced the technique of controlled hepatectomy of the Glisson pedicle at the hepatic hilum. Combining both techniques helps to limit complications due to anatomical abnormalities, minimize the ischemia of the remaining liver parenchyma, limit postoperative liver failure, reduce blood loss during surgery and avoid cancer cell proliferation to neighboring lobes.
In this study, the results showed that no patient died after surgery. There was one patient with transient liver failure after surgery, whose condition was improved after receiving medical treatment. Complications after surgery were mainly graded I (Clavien-Dindo grade). The postoperative complications we encountered included infection, ascites, and pleural effusion. The mechanism of pleural effusion and ascites was due to the release of the liver, the cutting of the ligaments that affect the regional lymphatic circulation or liver dysfunction after surgery. Pleural effusions were usually small in number, were treated medically or aspirated, and rarely required pleural drainage [5]. In this study, there were three cases of biliary fistula, accounting for 3.6%, and two patients underwent percutaneous biliary drainage intervention. There was one patient who had left liver resection and then had a biliary fistula and had to undergo biliary stenting to stop the leak. The cause of the biliary fistula, in this case, was the narrowness of the biliary tree. It might be related to clamping and cutting the left hepatic peduncle close to the biliary tree; hence when suturing the Glisson pedicle with Prolene string, it caused narrowing of the biliary tree. Biliary fistula is also a serious complication of liver resection. To limit biliary fistula after the liver tumor was extracted, we checked and sutured the cut Glisson pedicle with Prolene string, and pressed a dry gauze pad to the cut area for 3-5 minutes to check for bleeding points or biliary fistula. There are cases when we pump water through the cystic duct to check for biliary fistula. The incidence of biliary fistula in some studies ranged from 4.0% to 17%. Yoshioka et al. performed a retrospective analysis on 505 liver resections that showed a biliary fistula rate of 6.7%, with three independent risk factors: major hepatectomy, liver surface resection ≥ 57.5 cm2 and intraoperative bleeding 775 ml [6].
Recurrence of HCC is frequent, and about half of patients who undergo surgery will have a tumor recurrence within 3 years. In this study, there were relationships of tumor size, surgical margin, and portal vein thrombosis with patient mortality. Recent studies in large patient populations have shown that tumor size acts as an important predictor of HCC tumors [7-9]. This may be explained by the fact that large tumors are often associated with other clinical factors including microsatellite nodules, spermatogenesis, multiple neoplasms, major vascular invasion, or distant metastases, which have a positive association with tumor recurrence but a negative impact on patient survival. Ishii et al. concluded that patients with large HCC tumors < 7 cm in diameter have a high risk of poor prognosis due to the high rate of lung metastases, even in the absence of gross vascular invasion [10]. Tumor size is an important risk factor for HCC metastasis. In the group with tumor size larger than 5 cm, the rate of liver metastasis increased by about 30% and the rate of portal vein thrombosis doubled compared with the group smaller than 5 cm [9].
The surgical margin in hepatectomy is determined to remove microsatellite nodules and thrombus caused by cancer cells invading blood vessels around the tumor, prevent future recurrence, and preserve sufficient healthy liver parenchyma. This is particularly important for HCC because the disease develops mainly from cirrhotic tissue, and adequate preservation of healthy liver parenchyma is critical to successful treatment. Although extensively studied, the optimal surgical margin for liver resection remains controversial. The determination of the width of the surgical margin and variation according to tumor stage is still inconsistent; it ranges from 2 to 10 mm depending on the author [11-13].
Median OS in patients with advanced HCC with reported portal vein thrombosis ranged from 2.7 to 4.0 months if untreated [14]. Recent studies from China and Japan have shown that hepatectomy is associated with better survival than nonoperative therapies in HCC patients with thrombosis limited to the first branch of the portal vein or higher. Although advances in surgical technique and perioperative care have made surgery safer in patients with portal vein thrombosis, the occurrence of portal vein thrombosis in many studies remains a negative prognostic factor, which reduces the survival time of patients [15, 16].
Conclusions
Hepatectomy for HCC by a combination of extrafascial extrahepatic (Takasaki method) and extrafascial intrahepatic pedicle approaches (Ton That Tung method) is effective and safe, and side effects and complications can be controlled. Patient selection is a key issue and plays a very important role in the outcome of treatment.





