
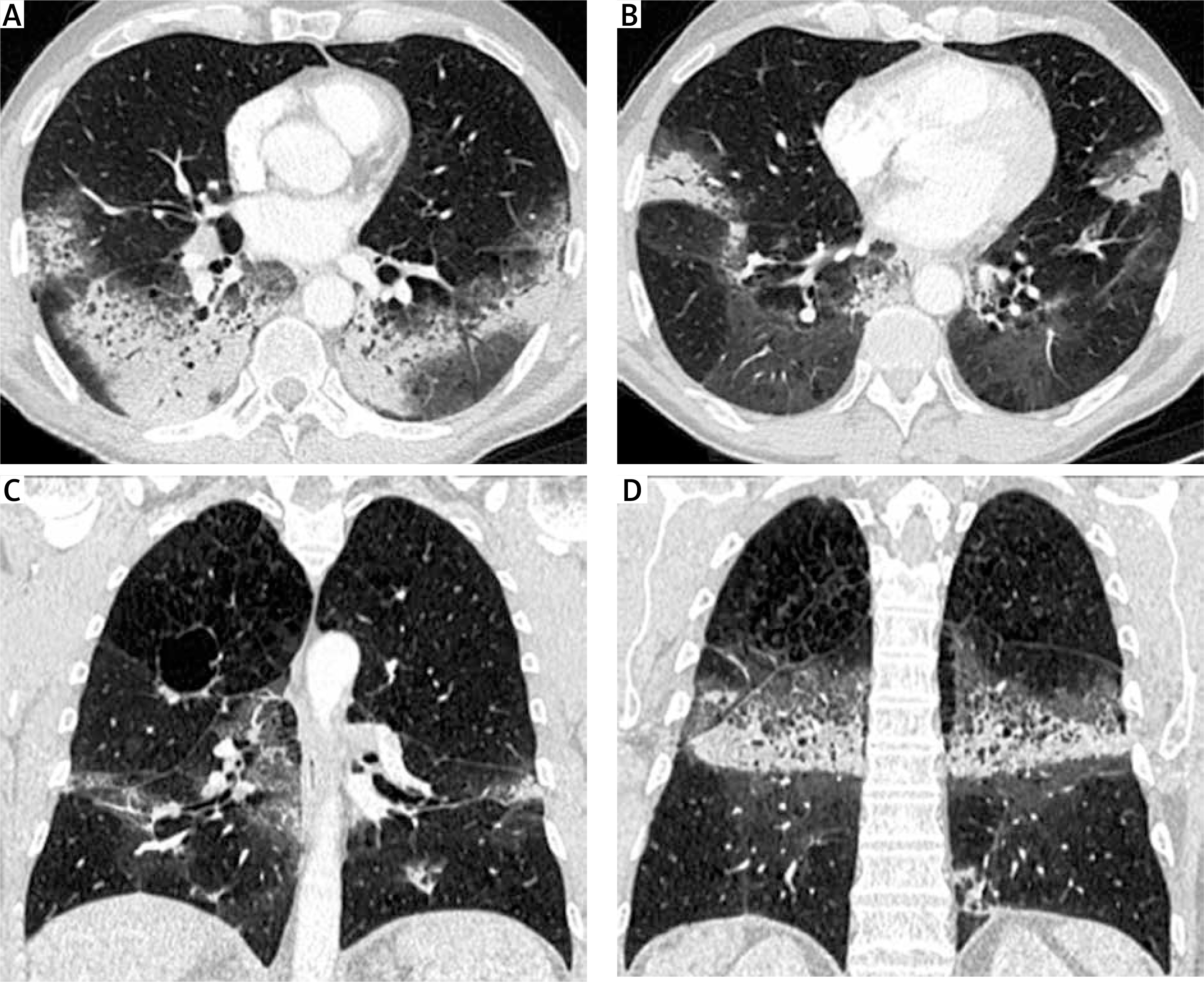
A 56-year-old man with stage IV non-small cell lung cancer (NSCLC) presented to the emergency department with progressive dyspnea and hypoxia. He had been diagnosed with adenocarcinoma of the right upper lobe 16 months earlier. PD-L1 expression in the tumor was 2%, and no other gene driver mutations were detected. The patient initially received treatment with a combination of platinum-based chemotherapy and immunotherapy (pembrolizumab). After the initial partial response to treatment, the patient remained in consolidation therapy treated only with pembrolizumab (Keytruda) for the last 12 months. At the time of the investigation of the progressive dyspnea, a chest radiograph and a computed tomography (CT) scan were performed. The chest radiograph showed bilateral airspace opacities consistent with either pneumonia or pneumonitis (Figure 1). The CT scan showed symmetrical bronchocentric consolidation with distribution suggestive of organizing pneumonia induced by pembrolizumab treatment (Figure 2). Bronchoalveolar lavage (BAL) was performed confirming the radiological diagnosis and excluding infection. The patient was treated with steroid therapy with clinical improvement and resolution of the symmetrical consolidation. Pembrolizumab (Keytruda) is a programmed cell death protein 1 inhibitor that is used as frontline treatment for NSCLC, with significant improvement of the survival rate [1]. Despite pembrolizumab’s clinical benefits, some patients develop associated immune-related adverse events (IRAE) including pneumonitis [2]. Immunotherapy-associated pneumonitis is a rare (3–6%) [3, 4] but severe complication characterized by focal or diffuse parenchymal inflammation. The time of onset of pneumonitis after administration of immunotherapy is variable [5]. Symptoms are often nonspecific, including dyspnea, cough, malaise and low-grade fever, requiring a high index of suspicion, whilst some patients may be asymptomatic [4]. As a result, diagnosis of immunotherapy-induced pneumonitis is usually achieved by excluding other potential causes. Clinically it is graded using the Common Terminology Criteria for Adverse Events (CTCAE) severity scale, which ranges from grade 1, asymptomatic, through to grade 5, where death occurs [6]. Diagnosis is based on appropriate history and suggestive radiological findings on CT scanning. The most common radiological features include ground glass opacities, interstitial reticulation, or bronchocentric consolidation suggestive of patterns of organizing pneumonia (OP), non-specific interstitial pneumonia (NSIP), diffuse alveolar damage (DAD) or hypersensitivity pneumonitis (HP) and reflecting the histological patterns of interstitial pneumonia [7–9]. Definitive diagnosis may require a combination of BAL and/or a biopsy. Treatment options include supportive therapy alone, oral or intravenous corticosteroids and cessation of immunotherapy [9].
Full text
Symmetric lung injury computed tomography pattern in pembrolizumab-induced severe pneumonitis
- Radiology Department, King’s College Hospital NHS Foundation Trust, London, UK
- Department of Radiology, Metaxa Cancer Hospital, Piraeus, Greece
- Department of Surgery, General University Hospital of Patras, Greece
- Department of Surgery, General Hospital of Eastern Achaia – Unit of Aigio, Greece
- Department of Medical Oncology, „Metaxa” Cancer Hospital, Piraeus, Greece
- Department of Radiology, AHEPA University Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece
- Department of Oncology, General University Hospital of Patras, Greece
- Department of Cardiothoracic and Vascular Surgery, Westpfalz-Klinikum, Kaiserslautern, Germany
- Respiratory Department, Athens Naval Hospital, Athens, Greece
- Department of Surgery, General Hospital of Lamia, Greece
- Department of Cardiothoracic Surgery, General University Hospital of Patras, Patras, Greece

References
Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe S, O’Brien M, Rao S, Hotta K, Vandormael K, Riccio A, Yang J, Pietanza MC, Brahmer JR. Updated analysis of KEYNOTE-024: pembrolizumab versus platinum-based chemotherapy for advanced non-small-cell lung cancer with PD-L1 tumor proportion score of 50% or greater. J Clin Oncol 2019; 37: 537-546.
Naidoo J, Wang X, Woo KM, Iyriboz T, Halpenny D, Cunningham J, Chaft JE, Segal NH, Callahan MK, Lesokhin AM, Rosenberg J, Voss MH, Rudin CM, Rizvi H, Hou X, Rodriguez K, Albano M, Gordon RA, Leduc C, Rekhtman N, Harris B, Menzies AM, Guminski AD, Carlino MS, Kong BY, Wolchok JD, Postow MA, Long GV, Hellmann MD. Pneumonitis in patients treated with anti-programmed death-1/programmed death ligand 1 therapy. J Clin Oncol 2017; 35: 709-717.
Sears CR, Peikert T, Possick JD, Naidoo J, Nishino M, Patel SP, Camus P, Gaga M, Garon EB, Gould MK, Limper AH, Montgrain PR, Travis WD, Rivera MP. Knowledge gaps and research priorities in immune checkpoint inhibitor-related pneumonitis. An Official American Thoracic Society Research Statement. Am J Respir Crit Care Med 2019; 200: e31-e43.
Johkoh T, Lee KS, Nishino M, Travis WD, Ryu JH, Lee HY, Ryerson CJ, Franquet T, Bankier AA, Brown KK, Goo JM, Kauczor HU, Lynch DA, Nicholson AG, Richeldi L, Schaefer-Prokop CM, Verschakelen J, Raoof S, Rubin GD, Powell C, Inoue Y, Hatabu H. Chest CT diagnosis and clinical management of drug-related pneumonitis in patients receiving molecular targeting agents and immune checkpoint inhibitors: a position paper from the Fleischner Society. Chest 2021; 159: 1107-1125.
Delaunay M, Cadranel J, Lusque A, Meyer N, Gounant V, Moro-Sibilot D, Michot JM, Raimbourg J, Girard N, Guisier F, Planchard D, Metivier AC, Tomasini P, Dansin E, Pérol M, Campana M, Gautschi O, Früh M, Fumet JD, Audigier-Valette C, Couraud S, Dalle S, Leccia MT, Jaffro M, Collot S, Prévot G, Milia J, Mazieres J. Immune-checkpoint inhibitors associated with interstitial lung disease in cancer patients. Eur Respir J 2017; 50: 1700050.









