
Summary
The aim of this study was to evaluate the implementation of the guidelines for secondary prevention of coronary artery disease in patients following non-emergency coronary artery bypass grafting or percutaneous coronary intervention. Control of risk factors and cardioprotective drug use was similar in patients who had undergone percutaneous or surgical revascularization. The analysis of three multicenter surveys provides evidence of a persistent potential for further improvement in cardiovascular risk in revascularized patients.
Introduction
Cardiovascular diseases are a leading cause of mortality in developed countries [1]. Despite advances in the pharmacological and invasive treatment of coronary artery disease (CAD) in recent years the risk of recurrent cardiovascular events in patients with CAD remains high [2, 3]. Patients who have undergone an elective myocardial revascularization procedure also constitute a very high cardiovascular risk group and have the most to gain from secondary prevention [4]. One of the most important factors increasing the risk of mortality in patients with established CAD is still unsatisfactory secondary prevention including lifestyle changes, control of risk factors and pharmacotherapy [4–8].
Aim
The aim of the present analysis was to evaluate temporal changes in the implementation of European Society of Cardiology (ESC) guidelines for secondary prevention by assessing control of the main risk factors and the rate of cardioprotective drug use in patients following myocardial revascularization procedures.
Material and methods
We analyzed the data of participants from three surveys appraising secondary prevention in patients with established CAD in 2006–2007, 2011–2013, and 2016–2017 [9–11]. The same five hospitals providing cardiological care in the city and surrounding districts participated in each survey. The methods used in surveys had been published previously and were similar each time [9–11]. Briefly, patients aged < 81 years and hospitalized for an acute coronary syndrome or a myocardial revascularization procedure were recruited and interviewed 6–18 months after discharge from hospital. The inclusion criteria for the present analysis were elective percutaneous coronary intervention (PCI) or scheduling for coronary artery bypass grafting (CABG). A patient’s personal medical history, lifestyle and medications used were evaluated using a standard questionnaire. Diabetes status was determined based on the diagnosis found in the discharge letter. Smoking status was verified by assessing the concentration of breath carbon monoxide using a Smokerlyzer (Bedfont Scientific). Height and weight were measured in a standing position without shoes and heavy outwear using standard scales with a vertical ruler (SECA). Body mass index (BMI) was calculated according to the following formula: BMI = weight [kg]/(height [m])2. Waist circumference was measured using a metal tape measure placed horizontally in the mid-axillary line, midway between the lowest rim of the rib cage and the tip of the hip bone with the patient in a standing position. Blood pressure was measured twice, on the right arm in a sitting position after at least 5 min of rest using an automatic device. The mean of two readings was used for the present analysis. A fasting venous blood sample was taken to measure plasma lipid and glucose levels. Glycated hemoglobin (HbA1c) was not measured in 2006–2007 and was only recorded in half of the participants in the survey in 2011–2013. The blood samples were analyzed in the central laboratory. The same laboratory was used in each survey. For the present report, we used the results of analyses performed no later than 12 h after blood collection.
We analyzed the proportions of patients with risk factors not at recommended goals: smoking, a fasting glucose level ≥ 7.0 mmol/l, BMI ≥ 25 kg/m2, waist circumference ≥ 88 cm in women and ≥ 102 cm in men. In the case of blood pressure and low-density lipoprotein (LDL) cholesterol two approaches were adopted. First, we analyzed the proportions of patients achieving goals recommended at the time of each survey. Second, we also analyzed the proportions of patients with blood pressure and LDL cholesterol levels above the goal values recommended at the time of the final survey.
The secondary prevention coefficient was calculated in the following way: one point was given for each controlled risk factor (non-smoking, blood pressure at goal, LDL cholesterol at goal, glucose < 7.0 mmol/l, BMI < 25 kg/m2) during the follow-up examination. The goal values for blood pressure and LDL cholesterol were based on the ESC guidelines, which were valid at the time each survey was conducted. Additionally, one point was given for taking an antiplatelet agent and an ACE inhibitor or an angiotensin II receptor antagonist. Thus, a patient’s secondary prevention coefficient could vary from 0 to 7.
The surveys protocols were approved by the institutional Bioethics Committee. All the patients signed an informed consent form.
Statistical analysis
Categorical variables were reported as percentages and continuous variables as means ± standard deviation. The Pearson χ2 test was applied to all the categorical variables. Normally distributed continuous variables were compared using Student’s t test or analysis of variance. Variables without normal distributions were evaluated using the Mann-Whitney U test or the Kruskal-Wallis analysis of variance. Generalized linear models as implemented in the Statistica 13 software (TIBCO Software, USA) were used to compare proportions after adjustment for age, sex, procedure, duration of education, professional activity, and period of time from discharge to the examination. Factors independently related to the secondary prevention coefficient were evaluated using multivariable regression analysis. A two-tailed p-value of less than 0.05 was regarded as statistically significant.
Results
We examined 260 patients in 2006-2007 (participation rate 84.1%), 200 in 2011–2013 (60.2%) and 190 patients in 2016–2017 (72.8%). The characteristics of the studied groups are presented in Table I. Participants of the third (2016-2017) survey were older, better educated and more likely to be employed compared to the participants of the first (2006–2007) and second (2011–2013) surveys. There was no significant difference in gender distribution between the surveys. A statistically significant decrease in the proportion of post-CABG patients was observed in each successive study.
Table I
Characteristics of the study group by survey
Mean diastolic blood pressure and LDL cholesterol levels decreased over time, while no significant differences were observed in systolic blood pressure, glucose levels, HbA1c levels, or CO in exhaled air between the surveys (Table II). Differences in the proportion of patients who did not reach treatment goals 6–18 months after discharge from hospital adjusted for a number of co-factors are shown in Table III. The was no significant difference in proportion of patients with fasting glucose ≥ 7.0 mmol/l among those with diagnosed diabetes: 44.3% in 2006–2007 vs. 44.9% in 2016–2017 (p = NS).
Table II
Temporal changes in the risk factors 6-18 months after discharge
Table III
Temporal changes in proportions of patients who did not reach treatment goals 6–18 months after discharge from the hospital
[i] HDL – high-density lipoprotein, BP – blood pressure, LDL – low-density lipoprotein. *BP goal of < 140/90 mm Hg (< 130/80 mm Hg in diabetics) in 2006–2007 and 2011–2013; < 140/90 mm Hg (< 140/85 mm Hg in diabetics) in 2016–2017. **LDL cholesterol goal of < 2.5 mmol/l in 2006–2007; < 2.0 mmol/l in 2011–2013; < 1.8 mmol/l in 2016–2017.
After multivariable adjustments we did not observe any statistically significant difference in the use of antiplatelets (91.8% in 2006–2007 vs. 96.3% in 2016–2017), β-blockers (90.3% in 2006–2007 vs. 92.6% in 2016–2017), or lipid-lowering drugs (88.7% in 2006–2007 vs. 93.7% in 2016–2017) 6–18 months after discharge from hospital (Table IV). In the same time, the proportion of patients reporting the use of calcium antagonists, diuretics, antidiabetics agents and anticoagulants increased significantly.
Table IV
Temporal changes in proportion of patients taking cardioprotective drugs 6–18 months after discharge from the hospital
The mean secondary prevention coefficient was 4.79 ±1.07 (median value: 5; first quartile: 4; third quartile 6) in 2006–2007, 4.42 ±1.14 (median value: 4; first quartile: 4; third quartile 5) in 2011–2013 (p < 0.001 vs. 2006–2007), and 4.67 ±1.04 (median value: 5; first quartile: 4; third quartile 5) in 2016–2017 (p = 0.26 vs. 2006–2007). Its value was equal to 7 in just 2.4% of patients in 2006–2007, 1.7% in 2011–2013, and 1.6% in 2016–2017, while 25.4% of survey participants in 2006–2007, 18.0% in 2011–2013, and 22.3% in 2016–2017 had a secondary prevention coefficient of at least 6 (p = 0.20). Figure 1 presents the mean secondary prevention coefficient values according to myocardial revascularization procedure and survey. Age, education and participation in second survey as compared to the first survey were related to the value of the secondary prevention coefficient in multivariable analysis (Table V).
Figure 1
Mean values of the secondary prevention coefficient to myocardial revascularization procedure and survey
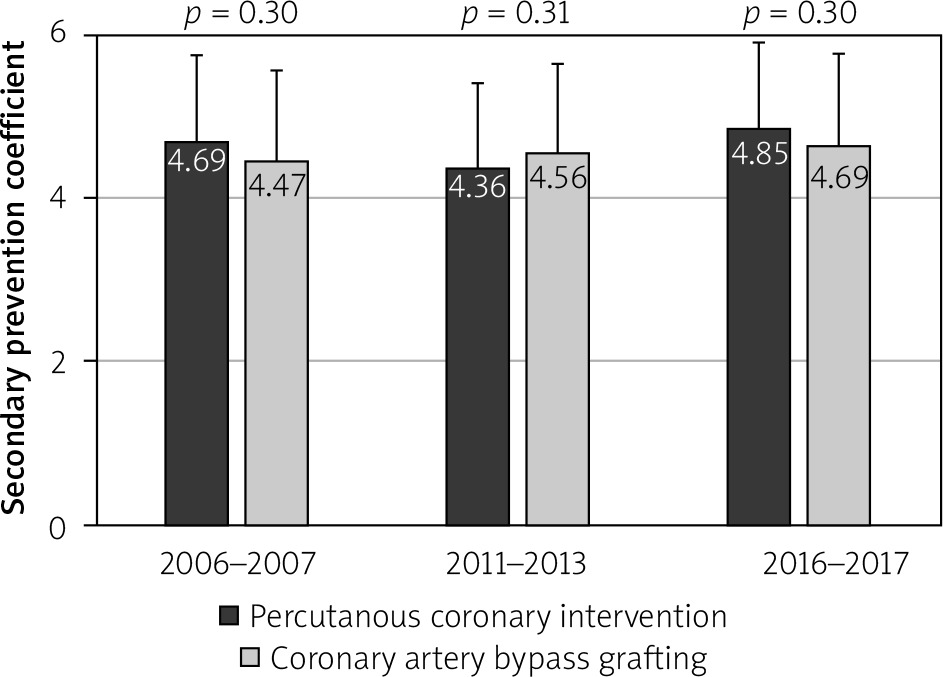
Table V
Factors related to the value of the secondary prevention coefficient in multivariable regression analysis
Discussion
Results of the EUROASPIRE surveys demonstrated the potential for further improvement in cardiovascular risk in patients with CAD [6, 8]. Lifestyle changes, control of risk factors and appropriate pharmacotherapy are major factors reducing the risk of cardiovascular events in CAD patients. The goal of elective myocardial revascularization is to alleviate symptoms in patients with angina and improve prognosis [12–14]. Although recently published results of the ISCHEMIA trial showed no significant influence of myocardial revascularization on cardiovascular event risk in patients with stable CAD, it showed a significant influence on angina, quality of life and physical performance [15, 16]. Several previous studies have also shown that myocardial revascularization is not only more effective in reducing angina and the need for antianginal drugs, but also improves physical performance and quality of life compared to the conservative treatment strategy both in a short- and long-term follow-up [17, 18]. However, the failure to properly implement lifestyle changes may contradict the benefits arising from the rapid development of pharmacological and invasive treatment of coronary artery disease observed in recent years [8, 19, 20].
The present analysis shows no significant improvement in the control of the main CAD risk factors and no significant change in the proportion of patients reporting the use of antiplatelets, β-blockers, and lipid-lowering drugs 6–18 months after discharge from the hospital. Importantly, when we used the LDL cholesterol goal as recommended in the ESC guidelines at the time of each survey, the proportion of patients reaching their LDL cholesterol goal decreased significantly [21–23]. This finding could be explained by the insufficient increase in doses of lipid-lowering drugs. In addition, an increased waist circumference could also play a role. In addition, the increase in BMI and waist (especially prominent among females) could also influence the effectiveness of treatment of hypertension and diabetes. Furthermore, the comparison of the secondary prevention coefficient across the surveys likewise failed to provide any evidence of an improvement in the quality of medical care in the field of secondary prevention of CAD. Moreover, the multivariable analysis of the secondary prevention coefficient suggests even a decreased coefficient in the second as compared to first survey. Taking all these factors into consideration, the present results suggest that there is still a considerable potential for reducing cardiovascular risk in patients after myocardial revascularization.
Traditional cardiac rehabilitation programs are less effective for patients with a lower level of education and tend to be less efficient in patients after non-emergency myocardial revascularization compared to subjects with acute coronary syndromes [24, 25]. Indeed, several recent initiatives have aimed at improving cardiovascular risk through education-based secondary prevention programs [26–28].
The present analysis presents a considerable change in the characteristics of patients undergoing myocardial revascularization, including the difference in age and education, as well as a shift in the management of coronary patients. Indeed, although we used the same inclusion criteria 62% of analyzed patients underwent PCI and 38% CABG in 2006–2007 whereas the corresponding proportions of patients undergoing PCI and CABG in 2016–2017 were 90% and 10%.
In summary, our results suggest decreasing mean LDL cholesterol and blood pressure, but increasing mean fasting glucose and waist circumference in patients with established CAD. Among participants of the last survey 17% were smokers, 39% had high blood pressure, 62% high LDL cholesterol, 20% high fasting glucose, 41% were obese and 57% had central obesity.
Our analysis has some limitations. Firstly, the participants were limited to those who had experienced an elective myocardial revascularization procedure. As a consequence, our results should not be directly applied to other CAD patients. Secondly, the participants of the surveys lived in a defined geographical area. Although the applicability of our results to other regions is uncertain, the observed trends accord with changes over time in the general population in Poland as well as in patients with CAD in other European countries [6, 29]. Thirdly, we could not analyze the dosages of prescribed drugs and lifestyle habits of the surveys participants, which could even increase the impact of the present results. Further studies should aim at estimating individual drug doses and lifestyle factors.







