
Summary
We present the 5-year results of a new treatment for type B aortic dissection. The method has been published both in the United States (JVS) and in Europe (EJVES) and has generated heated discussion. As this is a hot topic, it seems appropriate that the article should contribute to the ongoing discussions and controversies about effective treatment of aortic dissection.
Introduction
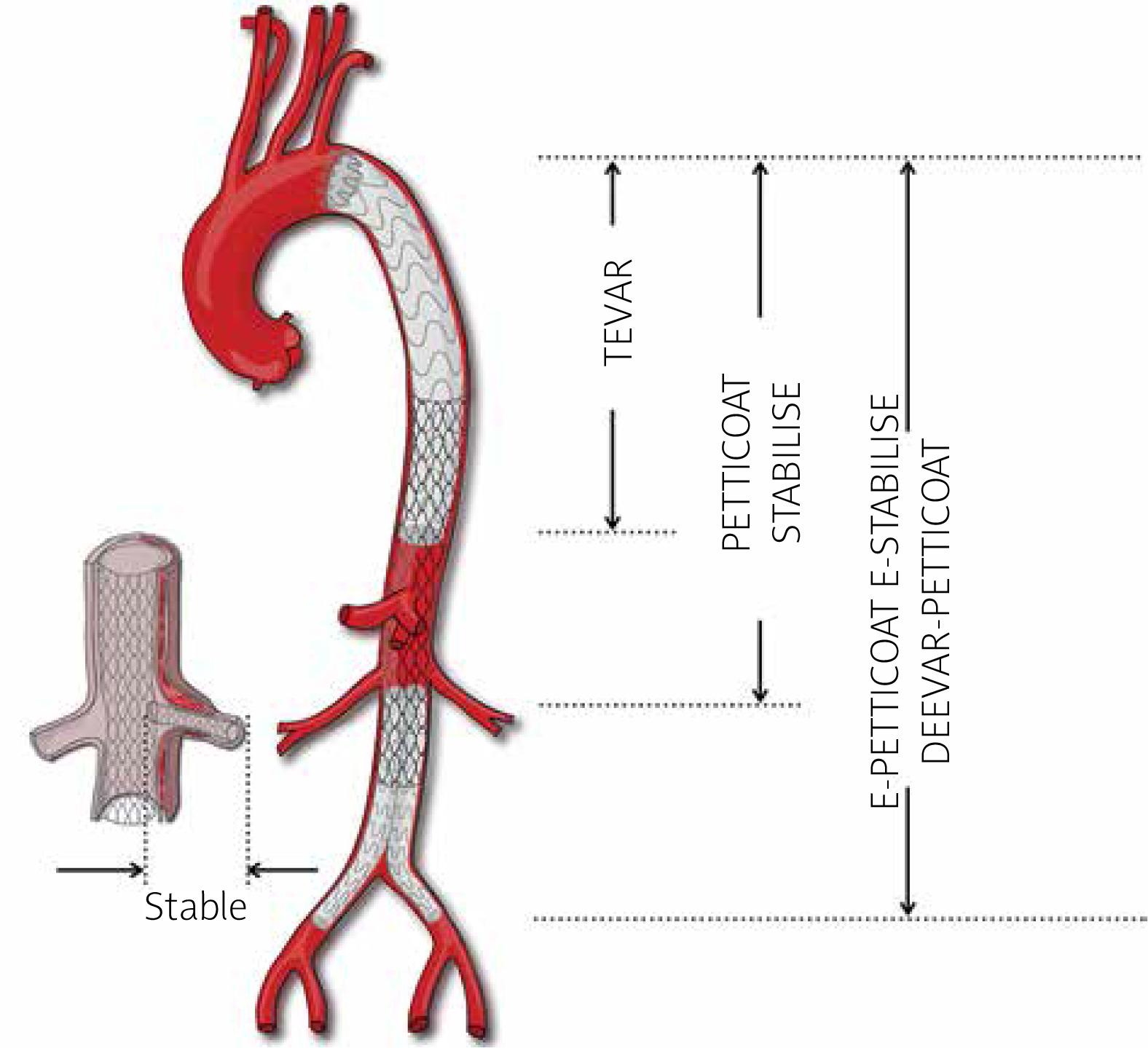
For several decades thoracic endovascular aortic repair (TEVAR) has been recommended as first-line treatment in acute complicated type B aortic dissection (TBAD) [1–3]. However, a simple cover of the primary entry tear with an endograft does not guarantee favorable remodeling [4, 5]. Therefore, more extensive techniques were subsequently introduced, for example: a provisional extension to induce complete attachment (PETTICOAT); stent-assisted balloon-induced intimal disruption and relamination in aortic dissection repair (STABILISE); staged total aortic and branch vessel endovascular repair (STABLE); a distal extended endovascular aortic repair (DEEVAR)-PETTICOAT; and finally an extended PETTICOAT which is moderated with clinical improvement during follow-up [6–11] (Figure 1). The extended PETTICOAT technique, introduced in 2019, presented very encouraging early results [11]. We were therefore expecting an improvement in the long-term remodeling rate.
Figure 1
Available endovascular options to reduce false lumen volume, promote membrane relining and increase true lumen flow
TEVAR – thoracic endovascular aortic repair, PETTICOAT – provisional extension to induce complete attachment, STABILISE – stent-assisted balloon-induced intimal disruption and relamination, STABLE – staged total aortic and branch vessel endovascular repair, e-STABILISE – extended STABILISE, DEEVAR-PETTICOAT – distal extended endovascular aortic repair PETTICOAT, E-PETTICOAT – extended PETTICOAT, RA – renal arteries, CT – celiac trunk.
Aim
This is a report of results at 5 years following use of the extended PETTICOAT technique in complicated acute TBAD.
Material and methods
This was a prospective observational study which included patients with complicated acute TBAD who qualified for endovascular treatment with the e-PETTICOAT technique. Complicated acute TBAD was recognized only in cases of clinical manifestation before or at the time of intervention; radiological findings were not enough to recognize complication in our study.
The extended PETTICOAT technique consists of combined implantation of thoracic stent grafts (Valiant Captivia, Medtronic, Santa Rosa, CA, USA; most commonly used size 32 × 200 mm; oversizing in the range of 2–10%) and nitinol self-expandable extra large bare metal stents (BMS-XL; Medicut, Pforzheim, Germany; most commonly used size 28 × 200 mm; since 2020 available only as 130 mm in length; oversizing in the range of 2–10%) in the visceral and infrarenal aorta, plus two parallel kissing iliac stent grafts (Endurant II, Iliac Extension; Medtronic; most commonly used size 16 × 156 mm) below the renal arteries, followed by forced ballooning (Reliant Medtronic, Santa Rosa, CA, USA) of all devices. A 5-year follow-up based on clinical outcome and computed tomography angiography (angio-CT) imaging was performed. Every angio-CT in the study was performed at our medical university with the same protocol using a slice thickness of 0.5 mm.
A prospective analysis of a small cohort with acute TBAD, treated within the first 2 weeks due to complications, was conducted. All patients were treated using the e-PETTICOAT technique. Size and volumetric measurements of true (TL) and false (FL) lumens, risk factors and anatomical conditions were assessed with angio-CT prior to surgery. Volumetric measurements were performed using a region of interest (ROI) tool from Osirix software (Pixmeo SARL, Bernex, Switzerland) in the arterial and late venous phases. Automatic ROI measurements plus manual corrections were performed by a single investigator without assessment of intra-observer variability. Good remodeling was defined by stable aortic size and complete false lumen thrombosis in the thoracic aorta. Persistent flow to the false lumen in the visceral and infrarenal segment was acceptable as long as it did not result in false lumen expansion. Predictions of degeneration rates were based on the Stanford Aortic Risk Calculator proposed by Sailer [12]. Long-term clinical results and remodeling were assessed after completing 5 years of follow-up based on angio-CT.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the Pomeranian Medical University (protocol code KB-0012/15/18, date of approval 05.02.2018).
Statistical analysis
Statistical analyses were conducted using Statistica software (version 13, StatSoft; Dell, Round Rock, TX, USA). Data are expressed as percentages, means, ranges and standard deviations. Fisher’s exact test was used to compare quantitative variables. Late survival was assessed by Kaplan-Meier analysis. A p-value less than 0.05 was considered significant.
Results
Eleven patients treated for acute complicated TBAD were included (in the period 2014–2018) in the study group. Table I presents clinical information and a list of complications and risk factors.
Table I
Epidemiology, sizing, risk factors and complications
| Parameter | Median (range) or n (%) | |
|---|---|---|
| Age | 54 (44–80) | |
| Sex | Male (M) | 9 (82%) |
| Female (F) | 2 (18%) | |
| Entry > 1 cm | 9 (75%) | |
| Inner curve entry | 3 (27%) | |
| Fusiform index > 0.65 | 0 (0%) | |
| Partial FL thrombosis | 7 (64%) | |
| Size > 4 cm | 5 (45%) | |
| FL > 22 mm | 11 (100%) | |
| Connective tissue disease | 0 (0%) | |
| Patent intercostal arteries | 9 (4–17) | |
| Dissection angle | 265 (230–360) | |
| Vessel dissection*: | ||
| LSA | 3 (27%) | |
| RRA | 6 (55%) | |
| LRA | 5 (45%) | |
| SMA | 4 (36%) | |
| CT | 5 (45%) | |
| IMA | 2 (18%) | |
| LICA | 9 (82%) | |
| RICA | 10 (91%) | |
| Complications (before surgery): | ||
| NOMI | 7 (64%) | |
| AKI | 2 (18%) | |
| ALI | 10 (91%) | |
| Stroke/paraplegia | 1 (9%)/1 (9%) | |
| Liver failure | 2 (18%) | |
| Rupture | 2 (18%) | |
| Recurrent symptoms | 1 (9%) | |
| Hypertension | 3 (27%) | |
| Shock/hypotension | 3 (27%) | |
| Pleural effusion/hemothorax | 7 (65%)/2 (18%) | |
| Number of damaged visceral branches** | 19 (43%) | |
| Treatment data: | ||
| Procedural time [min] | 112 (65–290) | |
| Intensive care stay [days] | 2 (0–35) | |
| Mechanical ventilation time [h] | 11 (0–840) | |
| Hospital stay [days] | 6 (1–38) | |
| Sizing and volumetry: | ||
| Total aortic maximal size | 35.2 mm (21–43 ml) | |
| CEFLV (before surgery) | 163 ml (18.7–279 ml) | |
| CEFLV (immediately after surgery) | 19.3 ml (0–108 ml) | |
| CEFLV (after 5 years) | 48.3 ml (0–156 ml) | |
| True lumen volume (before surgery) | 71.9 ml (10–139 ml) | |
| True lumen volume (immediately after surgery) | 192 ml (110–269 ml) | |
| True lumen volume (after 5 years) | 194 ml (112–274 ml) | |
* Vessels not departing from the true lumen with or without stenosis/occlusion. FL – false lumen, LSA – left subclavian artery, RRA – right renal artery, LRA – left radial artery, SMA – superior mesenteric artery, CT – celiac trunk, IMA – internal mammary artery, RICA – right internal carotid artery, LICA – left internal carotid artery, NOMI – non-occlusive mesenteric ischemia, AKI – acute kidney injury, ALI – acute limb ischemia – CEFLV – contrast-enhanced false lumen volume.
Five deaths occurred in the whole study group – 3 were reported as early deaths due to complications or failure of the endovascular treatment. The remaining 2 could be considered as distant deaths, with one related to the progression of aneurysmal degeneration (age 55 years old (yo)) and the other one not related to any aortic disease (80 yo). Detailed data for the whole group are presented in Table II.
Table II
Detailed characteristics of the 11 patients including clinical data, interventions, outcomes, mortality and follow-up
[i] E-PETTICOAT – TEVAR for thoracic + Medicut for visceral and EVAR iliac extensions for infrarenal and iliac segment, Oversizing (proximal for TEVAR – distal for Medicut), STABILISE – forced ballooning with Reliant balloon (Medtronic) along all devices, STABLE – by Zilver Flex self-expandable nitinol stent from COOK (oversizing 0-5%), T-Branch – custom-made five-branch device from COOK, ABP – arterial blood pressure, PICA – posterior inferior cerebellar artery, IH – intramural hematoma, ALI – acute limb ischemia SVS – Society of Vascular Surgery ABP – arterial blood pressure, ICU – intensive care unit. For other abbreviations see Table I.
Six patients from the study group are currently alive. Adverse remodeling was found in 3 patients (which ultimately caused the death of 1 patient). Cumulative chance of primary good remodeling was 38% (Figure 2 A).
Figure 2
A – Primary: good remodeling in the study group. B – Secondary: good remodeling in the study group after branched endovascular aneurysm repair (BEVAR) procedures. (Kaplan-Meier analysis)
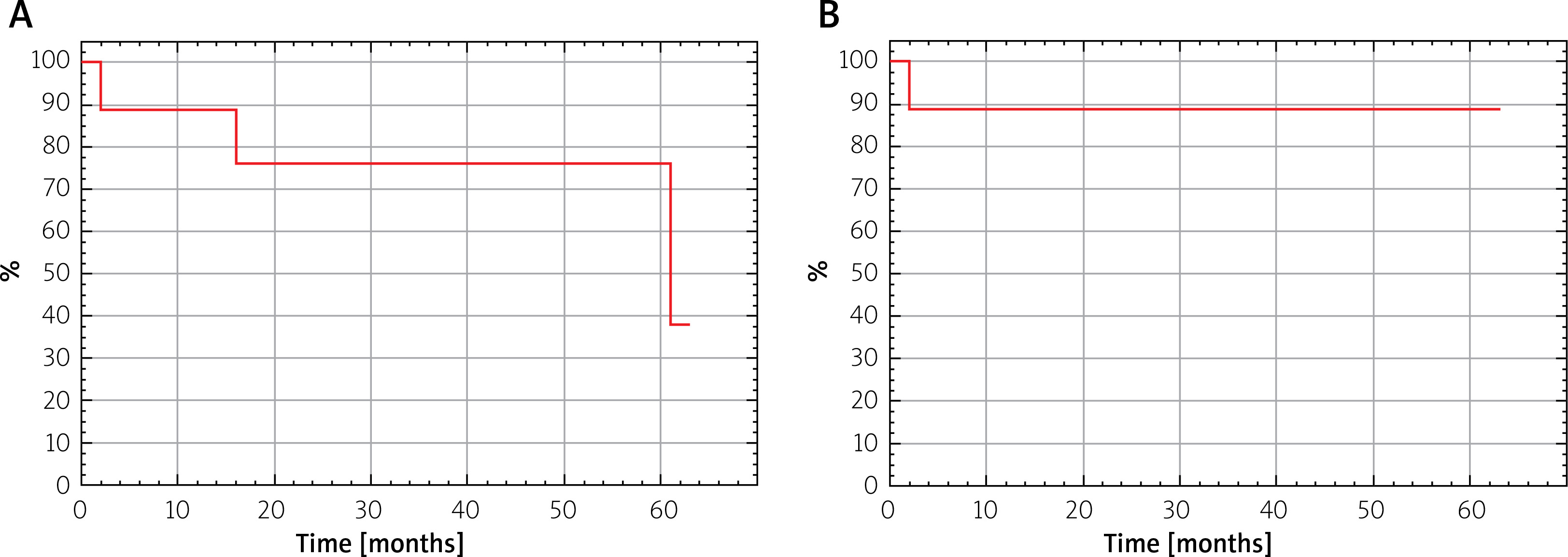
In 1 patient unfavorable remodeling was caused by leakage into the FL with increase in aortic diameter. In another case, despite complete thrombosis of the FL, an increase in aortic diameter of more than 55 mm occurred over 5 years. These patients were treated with a five-sleeve branch stent graft (Figure 3 B). In the remaining 5 patients, good remodeling with fully coagulated FL and stable aortic diameter was maintained. Therefore, overall the whole group had an 88% chance of favorable remodeling (Figure 2 B).
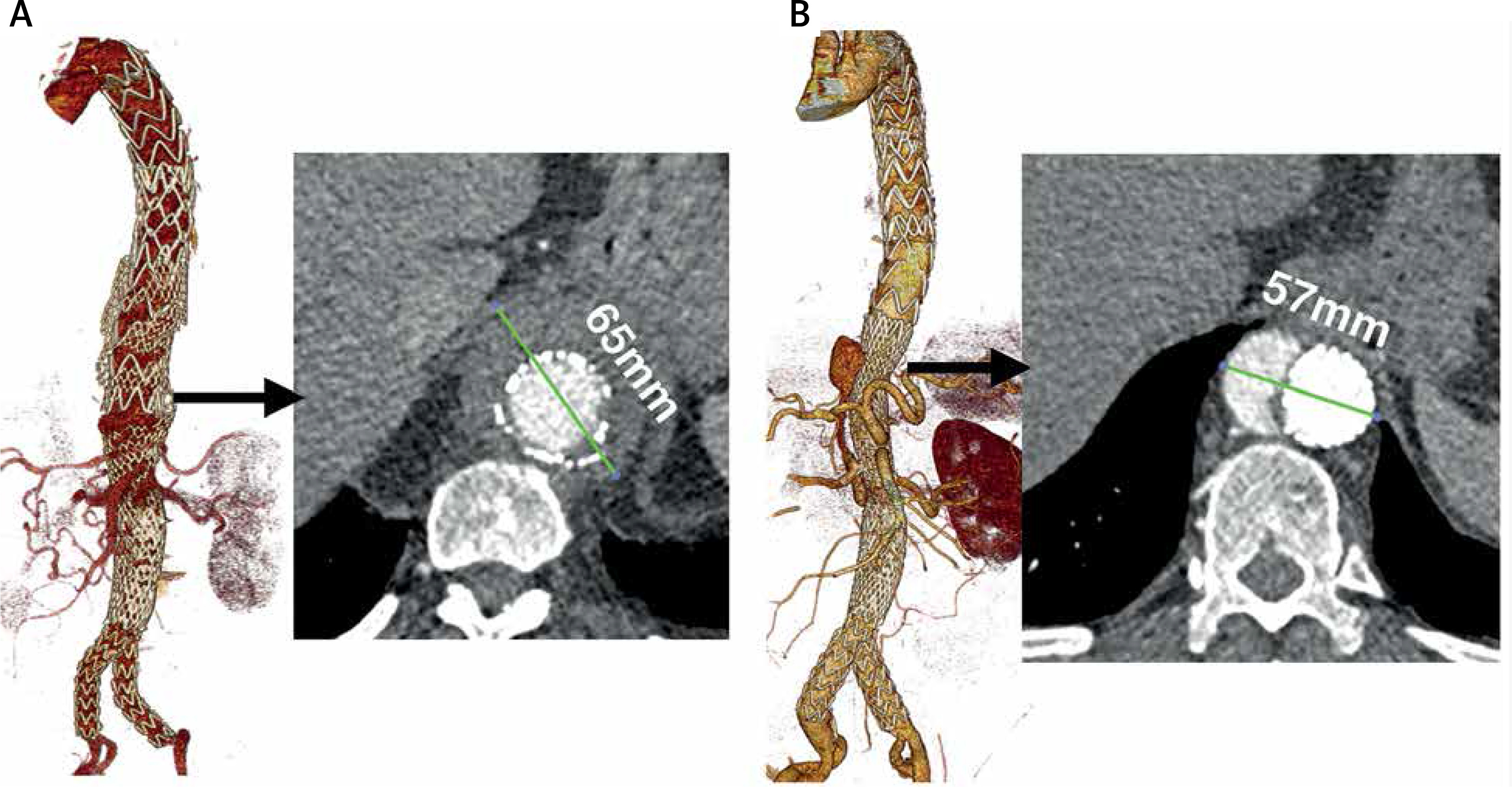
Figure 3
A – Aortic enlargement due to type V endoleak (sac extension) without false lumen perfusion. B – False lumen expansion due to entry from dissected right renal artery and impaired outflow. Values show total diameters of the aorta
The predicted probability of aneurysmal degeneration, as assessed by the Stanford Aortic Risk Calculator, was calculated as 56.55% (range: 16–100%) in survivors. The applied treatment (e-PETTICOAT) did not change the risk of degeneration significantly (48% observed versus 56% predicted, p = 0.56 Fisher’s exact test).
Discussion
Thoracic endovascular aortic repair has already been proven to be a successful technique (Instead, Adsorb trials), while PETTICOAT has not, due to its unpredictable impact on distal re-entry. Hence trials of the more comprehensive e-PETTICOAT style dissection have been performed. Although early and mid-term results were encouraging [11], after 5 years of follow-up after e-PETTICOAT with complicated TBAD we noted an equally high rate of unfavorable remodeling and requirement for complex repair. With no control group we decided to predict the rate of aneurysmal degeneration using the Stanford Aortic Risk Calculator proposed by Seiler [12]. However, this was created primarily for uncomplicated TBAD treated conservatively and is not well suited for a group with complications due to the disparity in blood circulation between a true and a false lumen (which is an obvious limitation). Nevertheless, the predicted and observed primary degeneration rates were very similar (perhaps one additional case only might gain favorable remodeling after e-PETTICOAT in our group).
Additional comments are needed concerning the high rate of NOMI in our study. This is because we diagnosed NOMI in any case of static or dynamic stenosis of SMA (or in the case of static occlusion with persistent distal flow in n-2) with clinical manifestation of abdominal pain which was usually transient and not present just before surgery. Total occlusion with bowel necrosis was not observed.
The volumetric evaluation of dissection, and in particular the CEFLV, may have some prognostic significance in the cases studied [13, 14]. Sustained inflow into the FL from distal re-entry may ultimately lead to aneurysmal degeneration (Figure 3 B). If the CEFLV is 0 ml after surgery a full recovery can be predicted with some probability. However, this is not a certainty: see the case in Figure 3 A. This patient had a completely coagulated FL but due to STABILISE and disintegration of the primary BMS mesh structure in the visceral segment, the aortic diameter eventually exceeded 6 cm, which qualified the patient for BEVAR. Therefore, patients should be included in permanent surveillance programs. This is suggested from evidence that mechanisms determining aneurysm formation after dissection cannot be fully predicted.
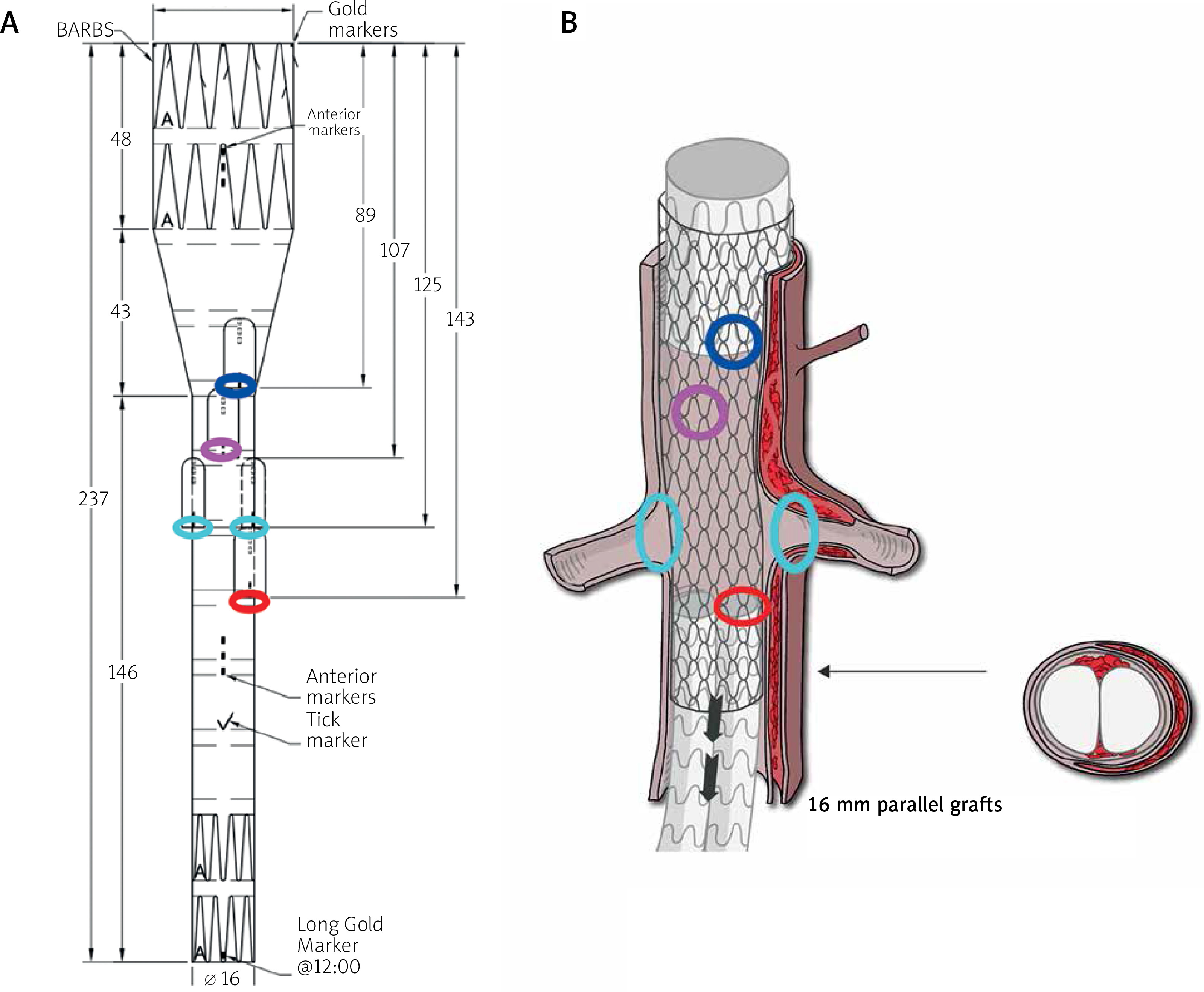
From the beginning of the study there were technical issues as follows. Any previous intravascular interventions, other than standard TEVAR, made further treatment with branched or fenestrated stent grafts more difficult, due to the presence of mesh (PETTICOAT, STABILISE or e-PETTICOAT) or high aortic bifurcation (Nelix as in e-PETTICOAT) [15]. This confirmed that branched stent grafts (T-Branch type, COOK) with five sleeves are required for repair after e-PETTICOAT (Figure 4). An additional challenge was the need to connect an 8 mm BEVAR branch with a 16 mm diameter parallel stent graft in an infrarenal segment, for which the 9 × 80 mm VBX (GORE), flared into an iliac leg artery diameter, is most suitable.
Figure 4
Five-branched BEVAR device, with color-marked target vessels, to repair a failed e-PETTICOAT
Therefore, it seems that extensive procedures of this type should be approached with caution in the acute phase of dissection, because there is no guarantee that this will be the last procedure for a particular patient.
An obvious limitation was the small patient population. Additionally, there was a lack of direct comparison between TEVAR and e-PETTICOAT. Possible bias arose from the heterogeneous nature of complications qualifying for primary intervention.







