
Introduction
The number of elderly individuals with diabetes is steadily on the rise [1]. According to estimates from the World Health Organisation, the global diabetic population aged 20–79 years is projected to reach 700 million by 2045, signifying an annual worldwide health expenditure of approximately $760 billion for diabetes [2]. A study conducted in Iran reveals that, on average, one out of every three individuals over the age of 60 years has diabetes [3]. Type 2 diabetes escalates the susceptibility to various ailments, including cardiovascular diseases, ocular complications leading to blindness, lower limb amputations, and renal and infectious maladies. Among these, urinary tract infection (UTI) is the most prevalent infectious condition affecting people with diabetes [4].
Urinary tract infections can manifest in the urinary tract, kidneys, or bladder [5], and they are a prevalent concern among elderly adults [6, 7]. In the United States, UTIs account for approximately 5% of all emergency department visits by individuals aged 65 years and older [8]. A cohort study indicates that nearly 20% of adults aged 65 years and above experience at least one type of UTI over an average 5-year follow-up period [9]. Research involving approximately 30,000 women in the United States demonstrates that over 10% of women aged 65–85 years have experienced UTIs in the past 12 months, with a 30% increase among women aged 85 years and older [8, 10]. In a study conducted by Sharma et al., bacteriuria was found in 43% of type 2 diabetic patients aged over 60 years, and it was more common among female patients [11]. The higher prevalence of UTIs in females compared to males is probably attributable to the unique anatomical characteristics of the female urinary tract, including the shortness of the urethra and its proximity to the anus [12]. In recent years, there has been growing research to identify the clinical profile of UTIs in diabetic patients [13]. However, such studies on elderly patients are rare [11]. Urinary tract infections complicate blood sugar management in people with diabetes, necessitating increased monitoring, reducing the quality of life, and incurring additional treatment expenses for patients [14].
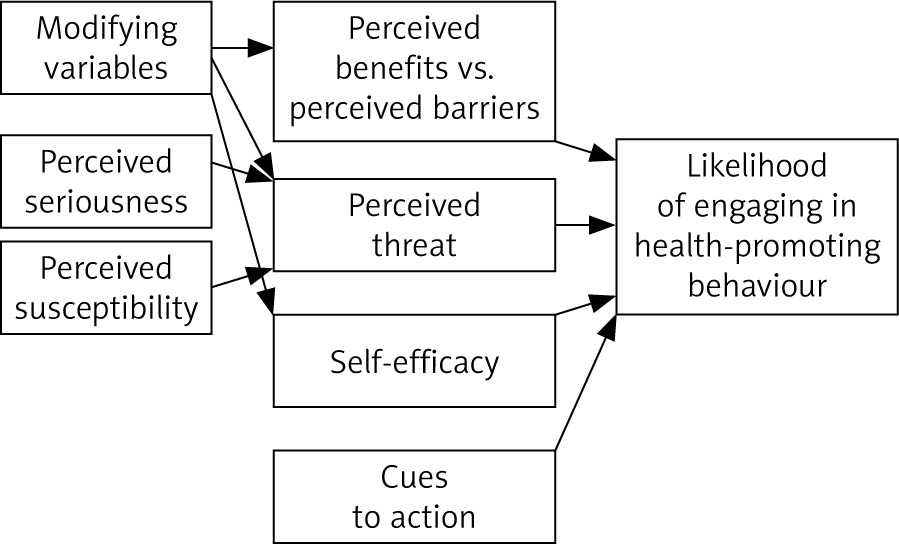
Given the concerns surrounding UTIs and the imperative for education in this domain, the present study assesses the impact of health belief model (HBM)-based education on promoting UTI prevention behaviours among elderly diabetic women. Non-pharmacological interventions and the encouragement of preventative practices for UTIs hold significant importance due to the adverse effects of drug resistance and the associated high treatment costs [15, 16]. Consequently, education and behavioural modification assume a pivotal role [17]. Identifying and fortifying the behaviours above is paramount to fostering effective behavioural change. Health education experts, therefore, leverage behaviour change models [18]. The efficacy of theory-based educational programs surpasses others [19]. The health belief model emerges as the most prevalent model for assessing behavioural transformations and disease prevention in the elderly demographic [20]. According to this model, individuals must perceive a threat (comprising perceived susceptibility and severity) and believe that a particular behaviour leads to a desirable outcome at an acceptable cost to alter their current behaviour patterns successfully. Furthermore, they must feel empowered to overcome perceived obstacles during action [21].
Considering the dangers caused by urinary infections, we find the need to educate diabetic elderly women in this field, because these infections are completely mixed with cultural and traditional and even psychological structures (intercourse methods, patterns of health habits, methods of washing, and use of inappropriate clothing), which can be controlled and prevented, and it is important to pay attention to it economically, socially, and medically. With a simple education or lifestyle change, we can reduce the number of elderly diabetic women with this infection and reduce the high costs of diagnosis and treatment. With these explanations, the researcher can claim that education in this field is the priority for the family, government, hospital, and health care team. Based on the literature review, the team of this study noticed a gap in the knowledge in this field, so they decided to conduct this study. According to the review of the background of the research, the effect of the HBM on the promotion of urinary infection prevention behaviours in diabetic elderly women, the results of the studies showed that most of the foreign studies were conducted on urinary infection in the elderly or urinary infection in the diabetic elderly, and no study was found that investigated the effect of the HBM on the promotion of UTI prevention behaviours in elderly diabetic women. In the literature review of internal studies, the results showed that no study has been conducted on the effect of the HBM on the promotion of UTI prevention behaviours in elderly diabetic women. According to what was described above, the present study aimed to determine the effect of HBM-based education the promotion of UTI prevention behaviours in elderly diabetic women. The hypothesis of this study is that HBM-based education can lead to the promotion of urinary infection prevention behaviours, reducing the incidence of urinary infection in elderly diabetic women as a result.
Material and methods
This study was conducted as an experimental investigation, with the statistical population consisting of elderly diabetic women who sought healthcare services at centres in Miandoab City in the West Azerbaijan province of northwestern Iran from January to May 2022.
Sample size and sampling method
In this study, a multistage random sampling approach was employed. Initially, Miandoab City was segmented into 4 distinct regions: North, South, East, and West. Subsequently, one of these regions was randomly selected. Two centres were randomly chosen within the chosen region among healthcare and health facilities visitors. One of these centres was then randomly designated as the intervention group location, while the other served as the control group location. Eligible participants among the elderly diabetic women who visited each centre were randomly included in the study, provided they met the established inclusion criteria. These criteria included a willingness to participate in the research, an absence of cognitive impairment, and no prior receipt of any training regarding UTI prevention. Exclusion criteria comprised emigration, relocation outside the region, and incomplete questionnaires. This study was conducted on elderly diabetic women regardless of whether they had a UTI. The focus of this study was on UTI prevention behaviours. For a visual representation of the study’s flow, please refer to Figure 1.
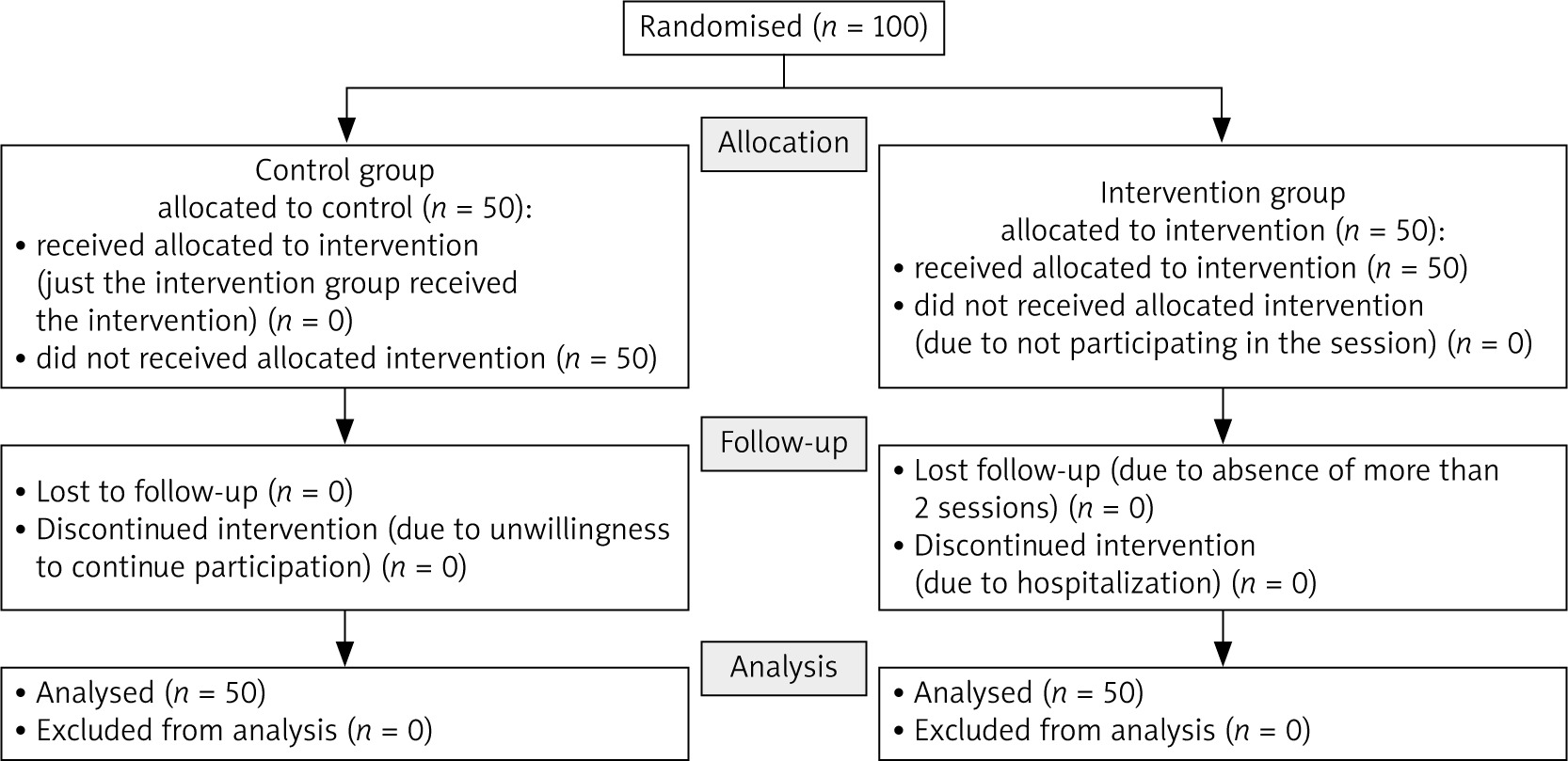
A sample size of 45 elderly individuals per group (intervention and control) was determined based on β = 0.05, β-1 = 0.8, and d = 0.56. Factoring in a 10% anticipated dropout rate, the final sample size was adjusted to 50 participants per group. Notably, the values for S2 and d were derived from previous studies conducted in this specific research domain [22].
Data collection tools and methods
A questionnaire was meticulously crafted based on the HBM to gather data, as recommended by previous studies [22, 23], and the consensus of a panel of experts (Fig. 2). This questionnaire encompassed 8 demographic inquiries: 5 queries on perceived barriers, 3 concerning perceived benefits, 5 on perceived susceptibility, one on perceived severity, 13 on self-efficacy, and 19 on behaviour. Additionally, 4- and 2-choice questions (yes or no) were employed to assess awareness, while a 3-choice Likert scale was employed to measure the dimensions of HBM attitude. Questions concerning self- efficacy and behaviour were adapted to include responses such as “always”, “sometimes”, “rarely”, and “never”.
In this research endeavour, health education experts and the elderly were solicited to provide feedback on the questionnaire’s appearance, evaluated against 3 conditions: entirely appropriate, appropriate, and inappropriate. This evaluation process served to establish the face validity of the questionnaire. Consequently, the face validity of the questionnaire was duly confirmed.
Furthermore, the content validity of the questionnaire was determined through the content validity ratio (CVR) and content validity index (CVI). The questionnaire was distributed to elderly and health education specialists to assess content validity, resulting in a CVR of 0.92 and a CVI of 0.95, both attesting to the questionnaire’s strong content validity.
To gauge the reliability of the questionnaire, Cronbach’s β coefficients were computed, yielding values ranging from 0.77 to 0.91. These coefficients indicate commendable internal consistency among the questionnaire’s items. Additionally, the intraclass correlation coefficients (ICC) of the questionnaire items ranged 0.71–0.74, affirming the desirable ICC values of the questionnaire.
Data collection transpired in 2 stages: prior to the educational intervention and one month after it. For the comfort of the elderly participants, data were collected by a trained interviewer who posed the questions and recorded their responses in the questionnaire. When elderly participants felt fatigued during the questioning process, they were provided a brief respite. It is imperative to note that, at the outset of the study, participants were comprehensively informed about the research objectives, their voluntary participation, the confidentiality of their information, and their voluntary involvement in the study.
Educational content
The educational content was organised based on the HBM constructs using scientific sources, then the contents of pamphlets, booklets, and meetings were prepared. The evaluation team (elderly and health education specialists) reviewed the educational content and made the necessary modifications (Table 1).
Table 1
Comprehensive overview of educational content aligned with health belief model constructs
Conducting the intervention
The educational program comprised 5 weekly sessions, each meticulously designed to focus on a distinct facet of the HBM. The first training session was held, during which the participants were asked about the duration of each session, and accordingly, the duration of the next sessions was set to one hour. It should be noted that the research team found this length of time appropriate for each session because they thought that the duration of each session should be such that the elderly do not get tired and also have the ability to learn the educational material. These sessions encompassed various pedagogical techniques, including lectures, interactive group discussions, dynamic question-and-answer segments, practical demonstrations, and immersive role-playing exercises. All sessions were conducted within the confines of healthcare centres.
The content of the pamphlet and booklet, including the definition of UTI, its types and symptoms, the necessity to pay attention to UTI, ways to prevent it (clothing style, eating habits, urinary habits, and hygiene habits), treatment method, and follow-up.
Furthermore, the educational materials underscored the imperative of vigilance about UTIs, elucidating various preventative measures, encompassing sartorial choices, dietary habits, urinary hygiene practices, and personal hygiene regimens. Additionally, the materials delved into the methodologies for UTI treatment and the subsequent course of follow-up.
Upon completing the questionnaires during the second stage, educational sessions were administered to the elderly participants in the control group, to comply with the ethical principles. They were also provided pamphlets and booklets, adhering to ethical principles. It is noteworthy that, given that more than half of the elderly women (constituting 50.5% of the cohort) were illiterate, their relatives were thoughtfully engaged to assist in conveying the contents elucidated within the booklets and pamphlets.
Data analysis
The scoring of questions and grouping of the points were based on previous research [22]. This investigation exhibited a complete absence of missing data because data acquisition was executed by a proficient interviewer, who diligently posed inquiries to elderly participants and meticulously recorded their responses within the structured questionnaire. Moreover, to facilitate the comprehensive data analysis, various statistical measures, including absolute and relative frequency distributions, mean values, and standard deviations, were deployed for descriptive data analysis. In pursuit of inferential data analysis, the Shapiro-Wilk test was used to scrutinise the normality of the dataset, while analysis of covariance (ANCOVA) with baseline adjustments was employed to make comparisons between pre-intervention and post-intervention phases. Additionally, the χ2 test was utilised to assess categorical data differences. Furthermore, the data was processed and visualised using SPSS version 28.0 software. Lastly, a significance threshold of p < 0.05 was adopted for all statistical analyses.
Strengths and limitations
Concerning the strengths of this study, the design of an educational intervention for preventing UTIs in elderly diabetic women was grounded in a comprehensive needs assessment (baseline), and it integrated the constructs of the HBM. However, the study also encountered certain limitations, the most prominent being a reliance on self-reported data. This limitation was mitigated through diligent data collection via interviews, clearly defined research objectives, and a one-month follow-up period. Extending the follow-up duration would potentially yields more precise results.
Research outcomes
The findings of this study hold implications for guiding policymakers. At the national level, it assumes paramount significance for governments to address health concerns and prioritise the well-being of older women.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The study was approved with the ethical code IR.BHN.REC.1400.011 at Behbahan Faculty of Medical Sciences. All the methods were performed in accordance with the relevant guidelines and regulations. Informed consent was obtained from all the subjects and their legal guardians.
Results
A cohort of 100 elderly women with diabetes participated in the study. Their average age was 62.30 ±7.63 years. Importantly, no statistically significant distinctions in mean age were observed between the experimental and control groups (p > 0.05). Detailed demographic information is presented in Table 2.
Table 2
Descriptive statistics of qualitative demographic variables
Table 3 presents the descriptive statistics of the indices and relevant sub-indices according to the follow-up period for the groups.
Table 3
Descriptive statistics of the indices according to the follow-up period
Comparison of knowledge scores, health belief model constructs, and urinary tract infection prevention behaviour in diabetic elderly women: experimental vs. control groups before and after intervention
The analysis of covariance, with baseline adjustments, was employed to compare the scores of various constructs before and after the intervention. This analysis used the partial eta squared (η2) to indicate effect size. Specifically, η2 > 0.0099 denotes a small effect size, η2 > 0.0588 signifies a medium effect size, and η2 > 0.1379 suggests a large effect size (26). This coefficient provides insights into the extent to which the independent variable explains the variance of the dependent variable. Additionally, a post hoc test using Tukey’s Least Significant Difference method was employed when significant differences were detected.
Based on the findings presented in Table 4, a notable discrepancy in mean knowledge scores between the experimental and control groups, with baseline adjustments, was observed (F [1.96] = 159, p < 0.001). Specifically, after adjusting for baseline in the experimental group (19.13), the mean knowledge score was significantly higher than in the control group (10.53). In essence, the intervention had a significant and substantial impact on enhancing knowledge related to UTI prevention among elderly diabetic women, and this effect demonstrated a large effect size (η2 = 0.62).
Table 4
Comparative analysis of knowledge scores, health belief model constructs, and behaviour in experimental and control groups about urinary tract infection prevention
In line with the results displayed in Table 4, a significant difference emerged between the experimental and control groups in terms of mean perceived barriers scores, accounting for baseline adjustments (F [1.96] = 32.45, p < 0.001). More precisely, the mean score of perceived barriers after baseline adjustments in the experimental group (3.56) was notably higher than in the control group (1.69). Consequently, the intervention significantly amplified the perception of barriers to UTI prevention in elderly diabetic women, and this effect exhibited a large effect size (η2 = 0.24).
Examining the outcomes presented in Table 4, it is evident that a significant difference existed between the experimental and control groups regarding mean perceived benefits scores while considering baseline adjustments (F [1.96] = 10.58, p < 0.001). Specifically, the mean score of perceived benefits after adjusting for baseline in the experimental group (2.34) was significantly higher than in the control group (1.68). This underscores the intervention’s substantial impact in augmenting the perceived benefits associated with UTI prevention in elderly diabetic women, with a medium effect size (η2 = 0.13) observed.
Furthermore, the results from Table 4 indicate a significant distinction between the experimental and control groups concerning mean perceived susceptibility scores following baseline adjustments (F [1.96] = 69.04, p < 0.001). Notably, the mean score of perceived susceptibility after adjusting for baseline in the experimental group (3.58) significantly exceeded that in the control group (1.91). In essence, the intervention significantly elevated the perceived susceptibility to UTI prevention in elderly diabetic women, and this effect demonstra- ted a large effect size (η2 = 0.37).
According to the findings presented in Table 4, a statistically significant difference emerged between the experimental and control groups concerning the mean scores related to perceived severity when adjusting for baseline values (F [1.96] = 0.74, p < 0.003). Specifically, the mean score for perceived severity, following adjustment for baseline measures, was notably higher in the experimental group (0.61) than in the control group (0.43). This signifies that the intervention significantly influenced the perceived severity of UTI prevention in elderly diabetic women. Furthermore, it is noteworthy that this effect was characterised by a medium effect size, estimated at 0.089.
Turning to the results of Table 4 once more, a noteworthy distinction was observed between the experimental and control groups concerning the mean scores related to self-efficacy when adjusting for baseline (F [1.96] = 36.8, p < 0.001). More specifically, the mean self-efficacy score, post-adjustment for baseline values, was substantially higher in the experimental group (39.83) than in the control group (32.53). This suggests that the intervention was pivotal in enhancing the self-efficacy associated with UTI prevention in elderly diabetic women. Notably, the magnitude of this effect was characterised by a large effect size, amounting to 0.51. It is worth noting that the effect size was large for all the sub-indices relating to the self-efficacy construct, encompassing aspects such as clothing style (0.29), eating habits (0.30), urinary habits (0.22), and hygiene (0.15).
Continuing to explore the results depicted in Table 4, a substantial difference was observed between the experimental and control groups in terms of mean scores related to prevention behaviour once baseline adjustments were applied (F [1.96] = 46, p < 0.001). In this context, the mean score for prevention behaviour, post-adjustment for baseline values, exhibited a significant elevation in the experimental group (60.1) compared to the control group (47.6). This underscores the noteworthy impact of the intervention on bolstering UTI prevention behaviour among elderly diabetic women. Significantly, the effect size associated with this effect was large, measuring 0.32. Remarkably, the effect size remained consistently large across all sub-indices associated with prevention behaviour, encompassing elements such as clothing style (0.22), eating habits (0.51), urinary habits (0.28), and hygiene (0.15).
Suggestions
This research advocates for educating healthcare system personnel, encompassing innovative training methods such as peer training and mass media education, augmented by telehealth services. Furthermore, it is recommended that this study be replicated on a larger sample size and in diverse settings to enhance the generalisability of the results. Future investigations should investigate the determinants of UTI prevalence among elderly diabetic women. Future studies are also advised to incorporate UTI laboratory tests in conjunction with questionnaires to assess the impacts of health behaviours more comprehensively.
Discussion
Urinary tract infections, as essential health ele-ments, pose significant challenges among elderly diabetic women. Therefore, a well-structured educational program substantially influences the mitigation of these issues [16]. This study aimed to ascertain the impact of HBM-based education on promoting UTI prevention behaviours in elderly diabetic women. It is imperative to highlight the innovative nature of this study within this specific domain.
During this study, the intervention exhibited a noteworthy effect on enhancing the examined variables. The research findings conclusively validate the efficacy of the HBM-based intervention in elevating UTI prevention behaviours among elderly diabetic women.
The demographic data and research variables, measured before the intervention, ensured the comparability of the sample populations in the 2 groups and minimised the potential impact of intervening variables on the research outcomes. All research variables were comprehensively examined as follows.
Knowledge
Based on the research findings, the HBM-based intervention significantly enhanced the knowledge score related to UTI prevention among elderly diabetic women. This outcome aligns with the findings of previous studies [18, 24]. The research outcomes underscore the pivotal role of health behaviours and habits in the aetiology of UTIs. Consequently, a pragmatic approach to reducing UTIs, particularly in women, involves acquiring knowledge about predisposing factors for UTIs and implementing alterations in health behaviours [22]. In the HBM context, knowledge about a specific ailment is a structural variable, functioning as a modifying factor [25]. According to the HBM framework, modifying variables indirectly influences health-related behaviours by influencing perceptions of severity, susceptibility, benefits, and barriers [25, 26].
Perceived susceptibility
Based on the present results, the HBM-based intervention exhibited a pronounced effect in augmenting the perceived susceptibility score concerning UTI prevention in diabetic elderly women. This outcome aligns harmoniously with findings from several studies [18, 23, 27, 28]. In contrast to the current investigation, Hashemi Parast’s research failed to document any significant impact of HBM-based education on perceived susceptibility as a means of preventing UTIs [29]. According to scholars, mere knowledge of disease proves inadequate in fostering preventive behaviours, whereas one’s mindset and attitude assume pivotal roles in adopting preventative measures [30]. The health belief model is a guiding framework that empowers individuals to comprehend their disease vulnerability and elect risk-mitigating behaviours [31]. Perceived susceptibility, within this context, denotes the subjective evaluation of the risk associated with developing a health issue [2, 3, 6]. The health belief model posits that individuals who perceive susceptibility to a specific health problem are inclined to engage in behaviours to minimise their risk of contracting that health issue [3]. When individuals acknowledge their susceptibility to a symptomless disease, this awareness can precipitate preventive behaviours [32].
Perceived severity
Based on the present results, the HBM-based intervention demonstrated a moderate impact on enhancing the perception of the severity of UTI prevention among elderly diabetic women. This outcome aligns with findings from several previous studies [28, 33, 34]. The perceived severity and susceptibility amalgamation is the perceived threat [6]. Perceived severity and susceptibility to a specific health condition depend on one’s knowledge base [3, 35]. Perceived severity encompasses the potential complications of developing or neglecting a disease without treatment. This encompasses medical and social consequences such as mortality, disability, pain, alterations in occupational circumstances, family dynamics, and social relationships [27]. Carmal conducted a comprehensive review of 46 HBM studies and concluded that perceived susceptibility was pivotal in predicting behavioural responses [36]. To enhance the level of perceived severity in this context, it is imperative to raise awareness regarding the gravity of UTIs, the ramifications of the disease, and the associated treatment costs [33, 37].
The health belief model is a valuable framework for comprehending societal responses to infectious diseases [38]. As society accentuates the severity of a given situation, individuals tend to perceive themselves as being at a heightened risk, potentially prompting them to undertake health-related measures [39, 40]. In a study by Bazargani et al., parents in the experimental group developed a newfound perception of their children’s vulnerability to UTIs, prompting them to take risk-reduction measures more seriously [28]. It is essential to note that individuals exhibit both cognitive and emotional responses to perceived severity. These responses independently influence their actions concerning seeking diagnosis and treatment. Cognitive responses tend to encourage individuals to pursue necessary behaviours, while emotional responses, acting as barriers, may deter individuals from seeking diagnosis and treatment due to the fear of receiving an unfavourable diagnosis. Consequently, it is advisable to evaluate, modify, or mitigate emotional barriers in conjunction with addressing the rational aspects of severity enhancement [41].
Perceived barriers
Based on the current findings, the HBM-based intervention exhibited a substantial impact on elevating the scores associated with perceived barriers to UTI prevention among elderly diabetic women. These outcomes align consistently with previous research [42–44] but exhibit disparities compared to other investigations [18, 29]. The escalation in the mean score of perceived barriers suggests an enhanced awareness among individuals regarding impediments hindering their engagement in preventative behaviours and their subsequent efforts to address these barriers [45]. Numerous studies have underscored the pivotal role of perceived barriers in articulating and prognosticating health-protective behaviours [46]. A study conducted by Jones et al. substantiates this perspective, as perceived barriers consistently mediated the correlation between exposure and behaviour across all models [47]. An individual’s perception of the obstacles surrounding a specific behaviour holds paramount significance in adhering to health practices – an aspect that can be effectively cultivated through educational programs introducing behaviour facilitators [48]. Scholars such as Zeigheimat et al. [40] and Bazargani et al. [28] have underscored the importance of addressing perceived barriers during educational interventions. Identifying and understanding perceived barriers to adopting health-conscious behaviours can instil motivation and bolster self-assurance [39]. Karimy et al. [49] reported a noteworthy decrease in mean scores related to perceived barriers within the intervention group both before and after the intervention. The divergence between the outcomes of the current study and the study by Karimy et al. could be attributed to different scoring systems applied to the construct of perceived barriers. In the present study, higher perceived barriers received lower scores, while lower perceived barriers garnered higher scores [18].
Perceived benefits
Based on the present results, the HBM-based intervention significantly increased the perceived benefits score for UTI prevention in elderly diabetic women. This finding aligns with the outcomes reported in several studies [18, 33, 50, 51]. In this context, perceived benefits denote individuals’ perceptions of the advantages of engaging in the targeted behaviour [52]. These studies suggest that perceived benefits are crucial in fostering health-related behaviours [33]. Education significantly contributes to enhancing perceived benefits [28].
Concerning enhancing UTI prevention behaviours in women, perceived benefits emerged as the second most influential predictor of behaviour, following perceived barriers [53, 54]. Davati et al. [55] observed that the “perceived benefits” construct strongly correlated with women adopting sun-protective behaviours. In a study by Hu et al., diabetic individuals with elevated levels of perceived benefits exhibited a greater inclination to engage in improved self-care practices [56].
Moreover, in a study conducted by Noroozi et al., no significant relationship was found between perceived benefits and behaviour. According to Schwarzer, perceived benefits within the health performance process primarily operate during the motivation stage but exert a limited influence during the performance stage [48]. The health belief model, which relies on educational initiatives, the dissemination of relevant brochures and books, the conduct of face-to-face classes, the cultivation of personal and social motivation, and the bolstering of self-confidence, exerts a crucial impact on perceived benefits and cements its favourable position [21, 57]. In a study by Farahmand et al., lectures, question-and-answer sessions, group discussions, educational slides, and pertinent handouts were instrumental in enhancing subjects’ perception of “perceived benefits” [58].
Self-efficacy
Based on the present results, the HBM-based intervention exhibited a pronounced effect in elevating the self-efficacy scores concerning UTI prevention in diabetic elderly women. This outcome aligns consistently with the findings of previous studies [24, 59]. Self- efficacy is a fundamental determinant in maintaining or modifying health behaviours. The higher the level of self-efficacy, the greater the propensity for acceptance, continuity, and dedication to healthy behaviours, bolstering one’s self-care prowess [60]. Cognitive decline, prevalent among elderly patients, can significantly influence their self-efficacy and self-care capabilities.
In the context of specific ailments, patients can nurture and fortify their self-efficacy and self-care competencies solely through active intervention, reconstructing their self-assurance to surmount challenges, and engaging in continuous learning [61]. In a study by Yu et al., self-efficacy emerged as a predictive factor for medication adherence in elderly individuals living with HIV (PLWH ) [62]. According to Naeemi et al., self-efficacy was identified as the primary predictor of hypertension self-care behaviours in the elderly [63]. In a study by Niama et al., self-efficacy was the chief predictor of physical activity in the elderly [64]. In conclusion, self-efficacy can anticipate self-care behaviours in chronic conditions such as diabetes [65].
Behaviour
Based on the present results, the HBM-based intervention substantially impacted elevating the scores of behaviour associated with UTI prevention in diabetic elderly women. In a study by Jiang et al., knowledge significantly but indirectly influenced chronic diabetes complication screening behaviours through perceived susceptibility, perceived benefits, perceived barriers, and self-efficacy [66]. In a study by Yazdanpanah et al., the HBM enhanced medication adherence in older individuals with hypertension by inducing changes in their beliefs [67].








