
Introduction
Extracorporeal techniques have been present in medicine for over 70 years. Many factors in history have influenced their development and popularisation, in particular the first discoveries of heparin in 1916 [1], the construction of cardiopulmonary bypass machine (CPB) by J.H. Gibbon [2], and finally the activity of J.D. Hill [3], J.C. German and A.B. Gazzaniga [4], and Robert Bartlett [5], who is also the author of the first RCT in perfusion support. In 1989, the Extracorporeal Life Support Organisation (ELSO, Ann Arbor, MI, USA, www.elso.org) was established as a regulatory and supervisory body for extracorporeal techniques, conducting a registry, scientific research, and setting trends and guidelines for extracorporeal life support (ECLS) and extracorporeal membrane oxygenation (ECMO) [6].
One of the breakthrough years was 2009, with the publication of the CESAR study [7] in “The Lancet” and the realisation of the real risk of the new pandemic influenza (H1N1). These 2 events caused extracorporeal techniques that were present in cardiac surgery to enter the framework of modern intensive care and critical therapy. The following years provided time for the structuring and lasting impact of extracorporeal techniques as a support technique in critical conditions in the world. The COVID-19 pandemic has become an accelerating point for the world’s interest in extracorporeal techniques. At its peak in 2022, the number of ELSO-registered centres exceeded 600 worldwide, with an annual number of cases exceeding 22,000 [7–11].
Because the ECMO therapy organisational model is complex and expensive, we developed in 2019 a course about “Artificial Life Support with ECMO” and created the “Centre of Artificial Life Support and Patient Safety” within a University Medical Simulation Centre. The project was awarded funding from a competitive national grant POWER by the Polish Ministry of Health.
The project started in 2019, within the new “Centre of Artificial Life Support and Patient Safety” at Poznan University of Medical Sciences. The centre was equipped with modern simulation education tools and classroom technology. The training program included theoretical and practical components related to advanced ECLS/ECMO techniques, as well as workshops and immersive scenario-based simulations. Such deliverables were part of the requirements for entering the competition. The training program was evidence based and relied on valid national respiratory failure and Extracorporeal Life Support Organisation (ELSO) guidelines. The “Artificial Life Support with ECMO” program was presented for ELSO endorsement, as the first in Poland. The program previously offered to 264 physicians was extended in 2022–2023 for 405 participants.
Aim
The purpose of this study was to assess the value of gaining evidence-based knowledge and improving skills of physicians by means of simulation techniques in the safe use of extracorporeal technologies to support patients in life-threatening conditions due to acute respiratory or circulatory failure. The scope of the training was a theoretical and practical introduction to advanced ECLS/ECMO techniques based on evidence-based medicine (EBM) and cardiopulmonary resuscitation guidelines, practical workshops, and simulations of high fidelity for interested physicians from all over Poland.
Material and methods
Project
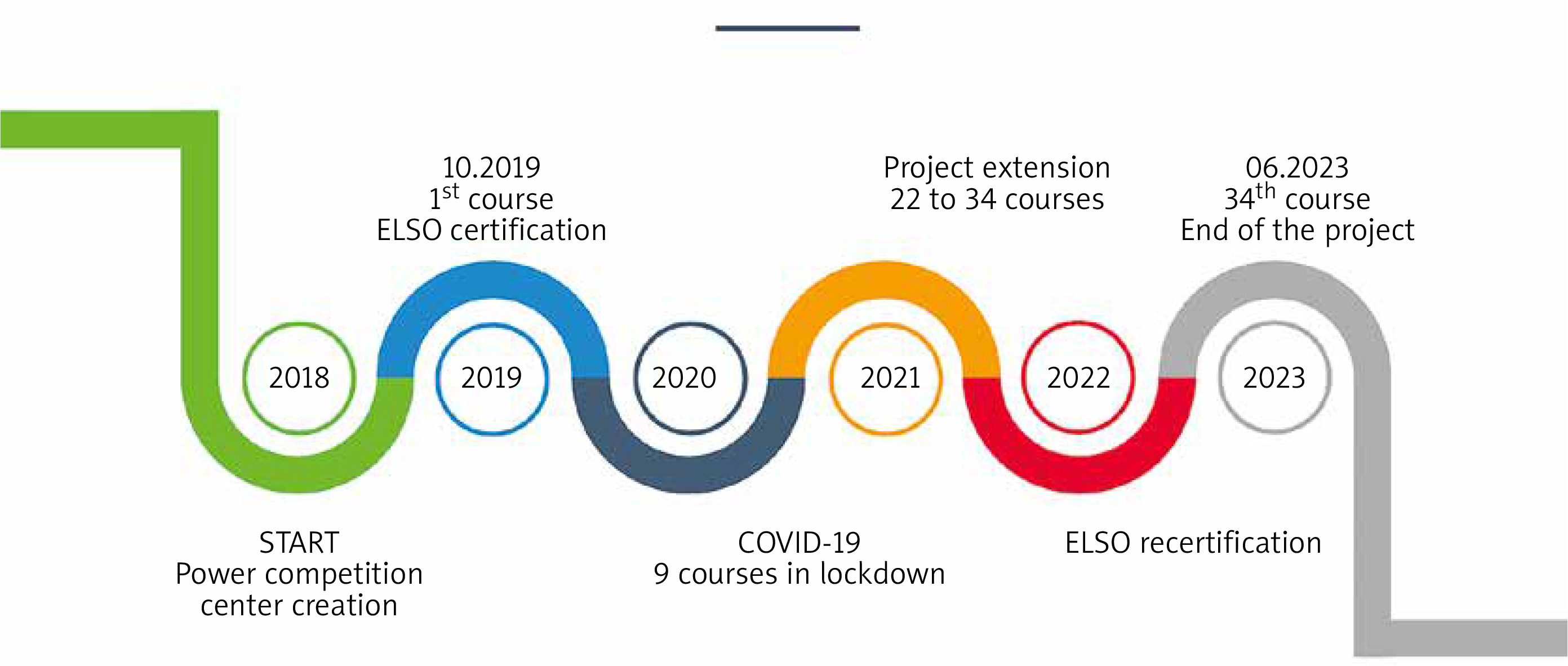
The project was awarded funding in 2018 from a POWER competitive national grant (POWR.05.04.00-IP.05-00-006/18) by the Polish Ministry of Health for a total of 2,750,000 USD (PLN 10,974,708.60). The program was launched in 2019 with 3 editions of the course and ELSO endorsement. However, during the difficult period of the COVID-19 pandemic in 2020-2022, 25 editions were carried out for participants. Finally in 2023 another 6 courses and ELSO re-endorsement were organised (Figure 1). The subject matter of the course clearly corresponded to the epidemiological and training needs of the country. Most of the participants represented centres assuming the primary burden on critically ill patients as a consequence of the COVID-19 epidemic, including extracorporeal life support techniques, high-quality cardiopulmonary resuscitation, and transportation of critically ill patients. Thanks to ELSO’s trust, the project gained recognition from the Organisation, and during the first meeting in 2019 it was positively certified and obtained the status of an ELSO-endorsed course.
Recipients
A group of 405 physicians participated in 34 editions of the course in 2019–2023 – specialists and residents in anaesthesiology and intensive care, cardiology, cardiac surgery, thoracic surgery, vascular surgery, transplantology, and emergency medicine. The recruitment was voluntary and open to all physicians in Poland, and after accepting the application, each candidate completed a study participation form and gave written consent.
Form of education
The postgraduate education was formulated in a 3-day course, where 50% of the educational hours were implemented in the form of workshops and classes in simulated conditions, comprising 25 didactic hours spread over 3 days during a one-weekend meeting (1 month apart). All course details are presented in Table I and are similar to the objectives and scope of knowledge presented by Puslecki et al. [12].
Table I
“Artificial Life Support with ECMO” course details
| Pre-test and pre-forms |
|
| Scope of the program |
|
| ECMO devices | Two different devices for ECMO were used: |
| Post-test and post-forms | Created with ELSO post course forms consisting of 11 questions of cognitive assessment, 4 of behavioural assessment, and 6 of technical assessment. Knowledge test consists of theoretical base of artificial life support with extracorporeal techniques. Additionally, course assessment and educational benefits were provided in 6 areas |
| Practice part | The exam simulation scenario where every participant had 8 min to perform an emergency intervention in a simulated ICU room. The proposed by ELSO forms evaluated cognitive, behavioural, and technical skills: |
| Education materials |
|
Logistic course ELSO requirements [6]
The recommended relationship number of students for participants was a maximum of 6 people per room and one instructor in the theoretical part and debriefing, and 2 instructors (one with formal debriefing training and another with content expertise) for every 6 participants in ECMO technical skills and during simulations.
Logistic course rearrangement during the COVID-19 pandemic
To adapt to COVID-19 pandemic restrictions and the lockdown in 2020-2021 we offered simultaneous knowledge-sharing and division into smaller teams (internal innovations in COVID-19 pandemic during 9 courses in 2020 and 10 in 2021). The relationship number of students for participants was changed: during the COVID-19 pandemic there were a maximum of 4 people per room and one instructor in the theoretical part, 2 instructors (both with content expertise) for every 2 participants in ECMO technical skills, and 2 (one with formal debriefing training and another with content expertise) for 4 during simulations in separated rooms. This was possible thanks to simultaneous simulations and debriefings in three 4-person subgroups with innovative audio-visual solutions.
Statistical analysis
Statistical analysis was performed using Statistica software version 13 with the ELSO database. Descriptive statistics of measurable variables were performed during the analysis. Due to the non-normal distribution among the variables, nonparametric tests were used. Data were presented as mean ± SD if normal distribution, and median (interquartile range) if non-normal distribution. To check the significance of differences the Mann-Whitney U test and Wilcoxon pairwise rank test were used as appropriate. A value of p < 0.05 was considered as statistically significant.
Results
Participants
In 2019–2023 the total number of participants was 405, and the same number both pre- and post-course documents were completed. In physicians the dominant motivation to participate in course was the necessity of self-improvement, in 25 other persons it was due to a recommendation, and in the last 2 it was due to orders from a superior. The participant demographics, specialty, and hospital settings with clinical practice and ECMO experience are included in Table II.
Table II
Participant demographics, specialty, and hospital settings with clinical practice and ECMO experience
ECMO cognitive assessments
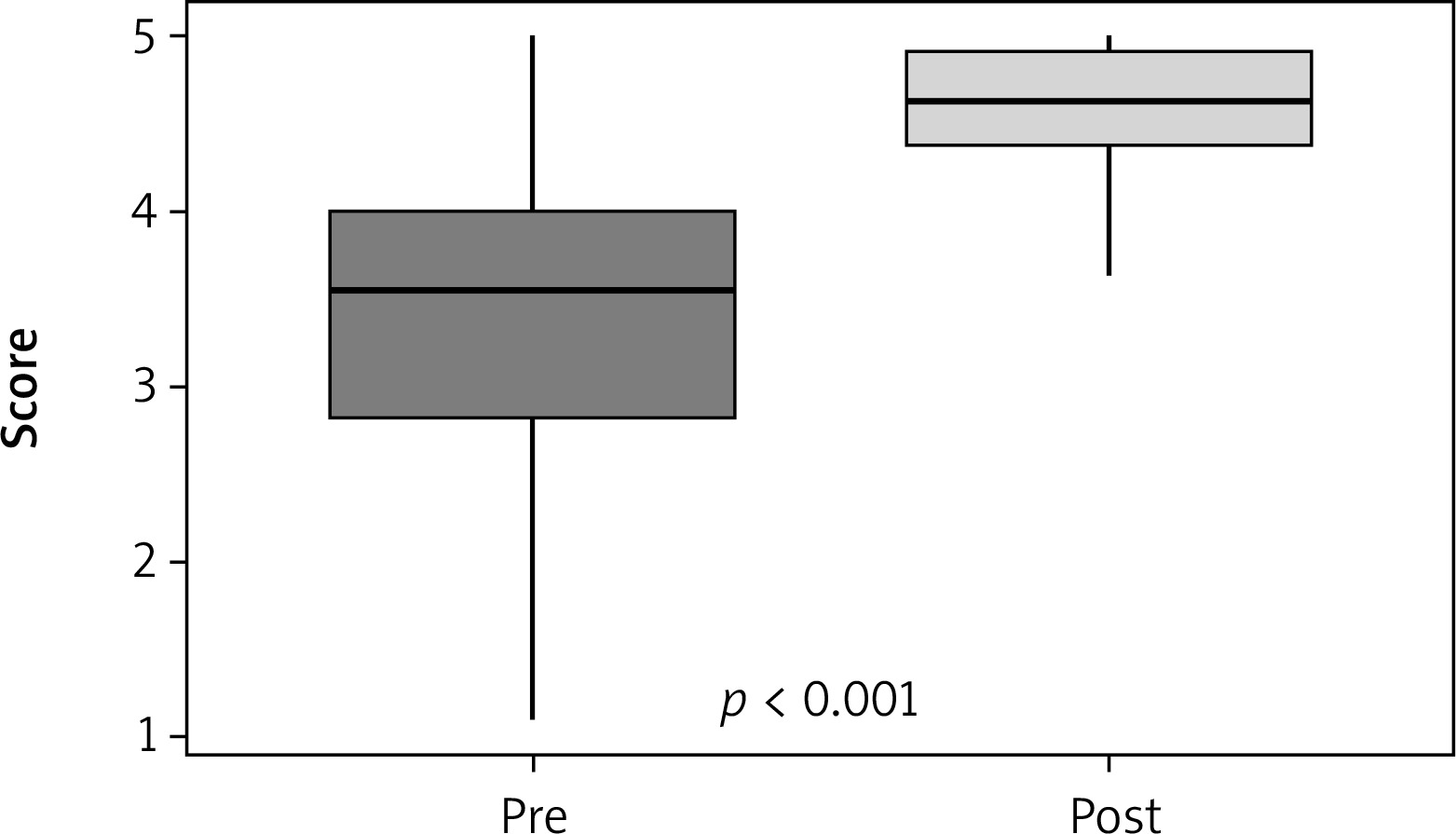
In all detailed aspects of cognitive assessment marked improvement was observed after the course. The mean value was significantly lower before (less than 4.0) than after the courses (more than 4.5) (p < 0.001) – Figure 2.
Figure 2
Mean pre- and post-course cognitive assessments. Box and whisker plots of the mean cognitive self-assessment scores across all cognitive categories. There was a statistically significant increase in the mean post-course scores compared to the precourse period by Wilcoxon signed-rank test (p < 0.001)
ECMO behavioural assessments
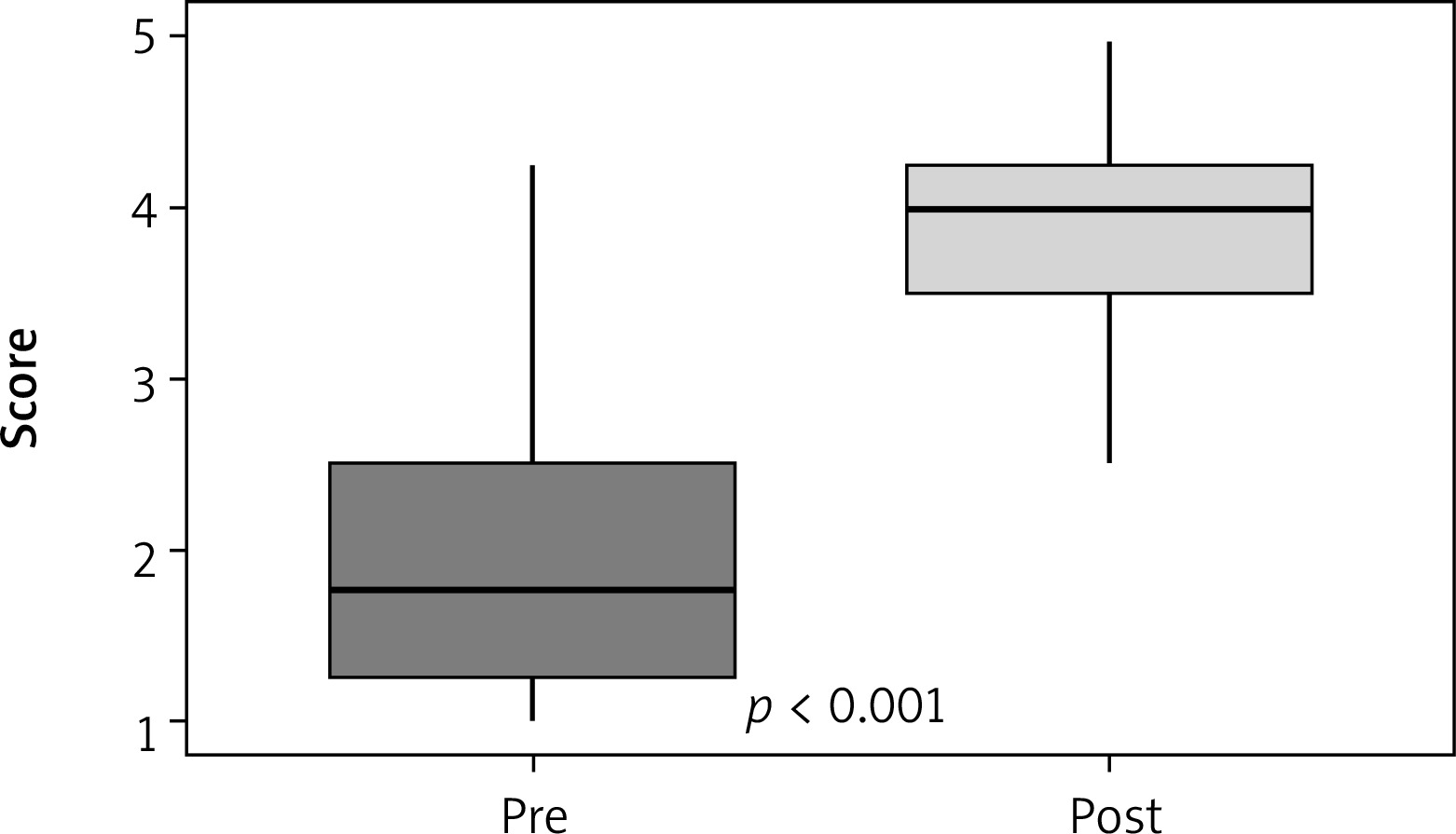
The course significantly improved the self-confidence of participants in different roles in ECMO teams as well as their reaction in emergency situations. The mean value of all aspects of behavioural assessment increased 2-fold, from 2 to 4 (p < 0.001) – Figure 3.
Figure 3
Mean pre- and post-course behavioural assessments. Box and whisker plots of the mean behavioural self-assessment scores across all cognitive categories. There was a statistically significant increase in the mean post-course scores compared to the pre-course period by Wilcoxon signed-rank test (p < 0.001)
ECMO technical assessments
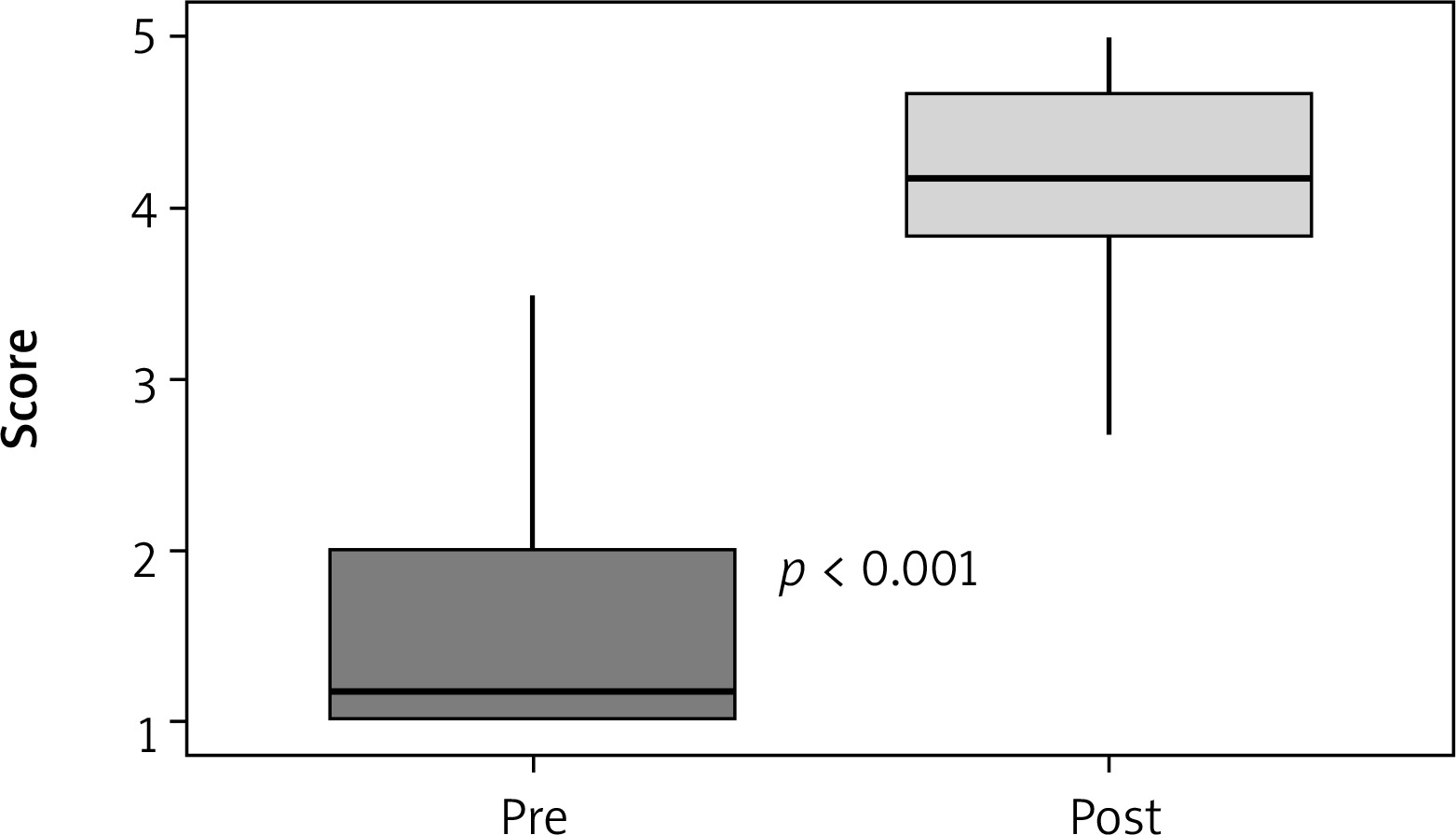
An enormous improvement in technical skills was observed after the course. Only single physicians had any experience with ECMO devices, and the median values in experience were minimal. Following 2 days devoted predominantly to developing practical abilities, post-course technical assessment revealed a more than 4-fold increase in expertise level in this area (Figure 4).
Figure 4
Mean pre- and post-course technical assessments. Box and whisker plots of the mean technical self-assessment scores across all cognitive categories. There was a statistically significant increase in the mean post-course scores compared to the precourse period by Wilcoxon signed-rank test (p < 0.001)
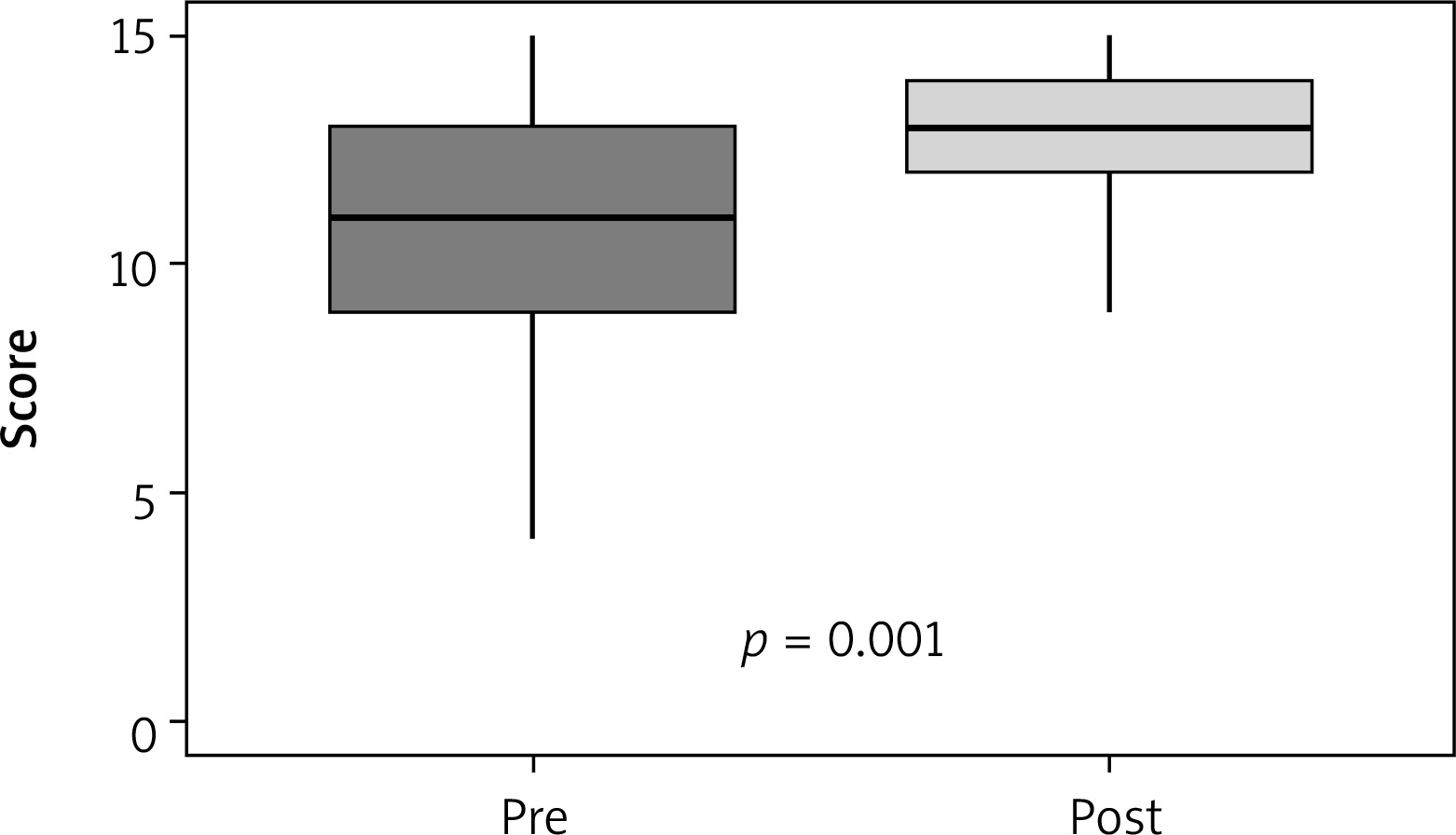
ECMO knowledge assessments
Pre-course knowledge regarding ECMO theory was more than satisfying – the mean score in the pre-course test was 10.97 out of 15 (73.1%). Despite a relatively high level of baseline knowledge, the results of post-course test were significantly higher than before training, and the mean score increased to approximately 13 points (85.3%) – Figure 5.
ECMO simulation assessments
In the group of 405 participants, 210 completed a VA pump failure sim, and the rest underwent a VV gas failure scenario. In the pump failure scenario the mean time to change the power supply to a hand crank was 220 s (80 : 480). In the gas failure sim the mean time to recognise a gas supply problem was 45 s (30 : 185). The main negative observation was the lack of proper patient support in both scenarios – emergency ventilator settings and proper CPR with ALS guidelines.
Discussion
ECMO in Poland before 2019
The extracorporeal techniques in VV configuration in Polish intensive care units were not routine procedures, except for a few centres that tried to use the Hub and Spoke concept: Krakow, Lublin, Warsaw, Poznan, and Opole. There were no systemic solutions that would ensure universal access to this support because there was no dedicated ECMO transportation. Additionally, there was a lack of epidemiological data regarding the use (exact numbers and places) of VV-ECMO systems. More information was available on VA-ECMO support in paediatric and adult cardiac surgery centres (more than 45 centres).
ELSO endorsement overview
ELSO course endorsement was developed because of the dramatic increase in the number of ECMO centres worldwide associated with numerous ECMO educational offerings [6]. While ongoing education and training are desirable to ensure familiarity and comfort in caring for ECMO patients and providing high-quality patient care, no universal consensus on the structure and delivery of these programs has been performed. Moreover, as ECMO technology advances, ongoing quality assurance of these educational programs presents a challenge. A centralised endorsement process is confirmation for standardisation of educational content and quality assurance.
In 2010, the Extracorporeal Life Support Organisation (ELSO) released guidelines outlining requirements for education of ECMO specialists [13, 14]. According to the ELSO endorsement document, “ELSO offers ECMO courses in the USA and internationally; numerous external ECMO courses and workshops also exist [6]. It is not known what proportion adhere to these recommendations, and it is likely that significant variability in content and delivery exist” [6, 13].
The Extracorporeal Life Support Organisation was established as a regulatory and supervisory body for extracorporeal techniques, and ELSO is the largest consortium of ECMO centres. The organisation has developed educational and clinical practice guidelines for ECMO provision and provides quality assurance for clinical use of ECMO via the ELSO registry [6]. ELSO plays a crucial role in providing minimum standards for ECMO education and developing processes that facilitate course and workshop development and endorsement. An endorsement process will ensure that a given course or workshop achieves an educational quality as set by ELSO while ensuring standardisation and consistency across courses. Furthermore, the endorsement process can provide valuable constructive feedback to ECMO centres and educators looking to develop ECMO educational activities.
ECMO in Poland during the pandemic
Despite the lack of dedicated solutions in VV support centres and in the developing pandemic, some casual solutions were prepared: firstly, 5 dedicated centres for VV ECMO support in COVID patients were created, and in the following months this was expanded to more than 15 centres, with a total of more than 800 procedures during the pandemic. Moreover, the air transportation concept was performed (HEMS – Helicopter Emergency Medical Service – helicopters and planes) in Poland, and for several months transport by helicopter was available 24 h a day in 5 Polish HEMS stations. During the pandemic months a lot of ground and air transportations of COVID-19 patients with ECMO support were performed [12, 15].
From 14 March 2020, a state of epidemic emergency was in force in Poland, and from 15 March a sanitary cordon and lockdown was introduced in the whole country, terminating all human gatherings. From May 2020, in accordance with the regulation of the Ministry of Health, a state of epidemic was in force in Poland with liberalisation of previous restrictions. In 2020 and 2021 our centre was the only one in the world, despite COVID-19 pandemic, offering courses in a stationary model. Only 3 courses in 2020 (March, April, May) were postponed during that year, and these were carried out in the following years. To adapt to COVID-19 pandemic restrictions, we offered simultaneous knowledge sharing and division into smaller teams (internal innovations in COVID-19 pandemic). This provided a valuable contribution to the development of highly qualified personnel and filled the gap in the field of extracorporeal techniques in Poland. Fifteen of the participants represented the national HEMS, which, with the weak specialist transport systems from ECMO, created a system of air transportation of patients with ECMO support.
The sudden COVID-19 pandemic and its dynamics in 2020 accelerated the implementation of extracorporeal techniques in many countries where it had not been widely used thus far. We noticed a significant improvement after the course in all cognitive, behavioural, and technical self-assessments and knowledge assessment in a group of 405 participants. An education centre makes it possible to improve the existing procedures, monitor individual ECMO cases, and constantly improve the qualifications of ECMO team participants. The Polish example confirmed the necessity of active training in the areas of application of extracorporeal techniques including patient transportation. During the pandemic years more than 10 dedicated mobile teams in the country were created. The small changes in the use of human and rooms resources in the Medical Simulation Centre during sanitary restrictions and lockdown did not affect the programmatic and substantive value of the meetings. The entire program planned at ELSO was implemented each time. It is worth emphasising that the changes made were dictated by the epidemiological safety of participants and trainers. It can be concluded that the use of the resources of the Medical Simulation Centre allowed for full program implementation even during such difficult changes as in the pandemic and with necessary epidemiological restrictions. Moreover, courses based on simulation techniques are generally resistant to threats such as global problems, but they are also characterised by a certain and acceptable flexibility that allow their adaptation to the introduced legal/sanitary regulations.
After the recertification in February 2023, the Poznan ECMO “Centre of Artificial Life Support and Patient Safety” is the fourth in Europe and one of 19 (in 12.2023) ELSO-endorsed education centres in the world with E-AEC certification (ELSO Adult ECMO Certification) [12, 15].
Limitations
The short-term results of the developed concept in “Centre of Artificial Life Support and Patient Safety” with ELSO cooperation are very promising. After the end of the project, the authors plan, together with ELSO, a prospective assessment of the long-term impact on the number of new ECMO centres in Poland, the number of supported patients, and the number of ECMO transportations.
Conclusions
The development of simulation-based education centres was found to be an invaluable achievement that enabled not only successful standardised training and testing of novel or previously accepted procedures, but also upgrading of technical skills, even in the challenging COVID-19 pandemic period.









