
Summary
There is evidence to support an association between the clinical status of patients and the bioavailability of clopidogrel, which is still widely used in cases of acute coronary syndrome (ACS). Additionally, clopidogrel bioavailability may be affected by the presence of CYP2C19 or ABCB1 gene polymorphisms. Our study showed that patients with ACS have similar levels of clopidogrel active metabolite as those with stable coronary artery disease. This association was observed both in individuals with ST-segment and non-ST-segment elevation myocardial infarction and was independent of the presence of CYP2C19 or ABCB1 gene polymorphisms.
Introduction
Although ticagrelor and prasugrel have become the standard antiplatelet treatments in acute coronary syndromes (ACSs), a large group of patients still present with indications for the use of clopidogrel. In particular, this refers to patients with stable coronary artery disease who are treated invasively as well as patients with ACS who have contraindications to the use of novel antiplatelet drugs (e.g., due to a high risk of bleeding associated with antithrombotic treatment) [1–3].
Clopidogrel is a prodrug that is metabolized to its active form by cytochrome p450 via complex biochemical processes that occur in the liver. The absorption of clopidogrel is regulated by glycoprotein P [4]. Only the active metabolite of clopidogrel can block the P2Y12 receptor, thus leading to inhibition of platelet activation and aggregation. It is believed that the clinical status of patients may affect clopidogrel metabolism [5, 6], which, in turn, may influence the antiplatelet effect of its active metabolite.
Aim
In the current study, we aimed to assess the levels of clopidogrel active metabolite with liquid chromatography–tandem mass spectrometry (LC-MS/MS) and to evaluate the effect of the drug on platelet inhibition in patients with ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI). To exclude genetic variability that might have affected the drug concentration and activity, patients were also assessed for the presence of the most common genetic polymorphisms that reduce the absorption (ABCB1) and activation (CYP2C19*2 and CYP2C19*3) of clopidogrel.
Material and methods
Study population
This single-center, open-label, prospective study included 199 patients hospitalized due to NSTEMI (n = 91) or STEMI (n = 108), who underwent percutaneous coronary intervention (PCI) with drug-eluting stent implantation. Patients with cardiogenic shock and those with Killip class IV were excluded. All patients provided written informed consent to participate in the study, and the study was approved by the local ethics committee.
The control group included 22 patients with stable coronary artery disease treated with PCI. All participants of the control group were tested to exclude the presence of ABCB1 as well as CYP2C19*2 and CYP2C19*3 gene polymorphisms.
All patients provided written informed consent to participate in the study, and the study was approved by the Wroclaw Medical University Ethics Committee.
Clopidogrel administration, blood collection, and plasma preparation
All participants received a loading dose of clopidogrel containing clopidogrel bisulfate as the active substance (600 mg), followed by a maintenance dose of 75 mg for the next 3 days. On day 3, blood samples were obtained 1 h after drug administration to assess the concentrations of the active metabolite.
Sample preparation
The method used to assess the clopidogrel active metabolite was described in our previous study [7]. Briefly, to stabilize the active clopidogrel metabolite, immediately after blood collection 2-bromo-30-methoxyacetophenone (MPB) was added to the sample. The MPB-derivatized clopidogrel active metabolite hydrochloride and [13C6]-(±)-clopidogrel carboxylic acid (internal standard) were purchased from Alsachim (Illkirch-Graffenstaden, France). Clopidogrel and clopidogrel carboxylic acid were obtained from Pharmaceutical Research Institute (Warsaw, Poland). Liquid chromatography–mass spectrometry (LC-MS) grade water, methanol, and acetonitrile were obtained from J.T. Baker (Deventer, the Netherlands). The formic acid (purity ≥ 98%), trichloroacetic acid (purity ≥ 99.5%), and MPB were purchased from Sigma-Aldrich (Poznan, Poland), while leucine-enkephalin was purchased from Waters (Warsaw, Poland). The serum concentrations of clopidogrel active metabolite hydrochloride, clopidogrel, and clopidogrel carboxylic acid were quantified by stable-isotope dilution LC-MS, according to a modified method adapted from Karaźniewicz-Łady et al. After additional centrifugation, the supernatant was analyzed using LC-MS/MS.
Liquid chromatography–tandem mass spectrometry
The LC-MS/MS analysis was performed using the nanoACQUITY UPLC system combined with a Xevo G2 QTof mass spectrometer (Waters, Warsaw, Poland). The analyzed compounds were separated in the HSS C18 column with a membrane inline filter (Waters, Milford, Massachusetts, United States) at 45°C. Mobile phase A consisted of 0.1% formic acid in water, while mobile phase B consisted of 0.1% formic acid in acetonitrile with an increasing gradient. The total run time of the method was 4 min, with a flow rate of 45 μl/min. Mass spectra for the analyzed compounds were acquired in positive ion mode electrospray ionization. Data acquisition was performed by means of the MassLynx Software (Waters, Warsaw, Poland), using the characteristic precursor and product ions. A quantitative analysis was performed using the QuanLynx software (Waters, Warsaw, Poland).
Platelet aggregation
Platelet aggregation was assessed on day 3 of clopidogrel treatment. Blood samples were obtained from a venous cannula into 2 tubes containing 0.109-mol/l trisodium citrate. Then, the blood was centrifuged at room temperature (800 × g for 15 min) to collect platelet-rich plasma. The sample was recentrifuged at 2400 × g for 15 min, and platelet-poor plasma was collected. Platelet reactivity was assessed within 2 h after collection by light transmission aggregometry developed by Born, using a single-channel Chrono Log 560CA lumi aggregometer (Chrono-log, Haverton, Pennsylvania, United States). A platelet-poor plasma sample with 100% light transmission was used as a reference. Consecutive platelet-rich plasma samples (light transmission, 0%) were placed in cuvettes and stimulated with adenosine diphosphate (ADP; 5 μmol/l and 10 μmol/l). The results were expressed as percentage of the maximum platelet aggregation (MPA) within 6 min. Calculations and platelet aggregation curves were performed using the dedicated AgroLink software (Chrono-log, Haverton, Pennsylvania, United States). All reagents and laboratory equipment were purchased from Biogenet (Piaseczno, Poland). They were stored and used according to the manufacturer’s instructions. The cutoff MPA values of higher than 46% and 67% were used to identify the high on-treatment platelet reactivity (HPR) to stimulation with 5-μmol/l and 10-μmol/l ADP, respectively.
Genetic studies
To identify ABCB1(rs1045642, c.3435C> T), CYP2C19*2 (rs4244285, c.681 G>A), and CYP2C19*3 (rs4986893, c.636 G>A) polymorphism, genetic material was extracted from 200 μl of whole-blood samples of each participant, using the High Pure PCR Template Preparation Kit (Roche Diagnostics GmbH, Mannheim, Germany). The lysate was centrifuged in a mini-column containing the silica membrane, which was then rinsed twice with a washing buffer. Finally, a mini-column elution buffer was applied to the membrane to recover the purified DNA.
Next, polymerase chain reaction (PCR) was carried out with 3 pairs of specific primers for CYP2C19*3(636 G>A), ABCB1 (C3435C> T), and CYP2C19*2 (681 G>A) using a Multiplex PCR Kit (QIAGEN, Hilden, Germany), according to the manufacturer’s instructions. A single nucleotide polymorphism of CYP2C19*2, CYP2C19*3, and ABCB1 was genotyped using a minisequencing technique, which is a modification of PCR. The SNaPshot Multiplex Kit (Applied Biosystems, Foster City, California, United States) was used for the analysis, according to the manufacturer’s instructions. The minisequencing reaction was performed with specific forward and reverse primers designed to hybridize to the template, ending before the designated polymorphic site. Dideoxynucleotide triphosphates, or fluorescent-labeled terminators, were involved in the reaction. Product detection was performed with capillary electrophoresis, using a 3130 Genetic Analyzer (Applied Biosystems). The results were analyzed with the GeneMapper ID v. 3.2 software (Applied Biosystems) against the internal GeneScan LIZ 120 standard.
Patients with at least one allele that negatively affects clopidogrel metabolism (CYP2C19*2, *3), were assigned to the loss-of-function (LoF) group, as opposed to the normal-function group (NoF), which included patients with CYP2C19*1. The study population was also divided into “good absorbers” (the GA group homozygous for the wild-type allele at position 3435CC) and “poor absorbers” (the PA group with heterozygous (TC) and homozygous (TT) mutations of the ABCB1 gene).
Statistical analysis
The statistical analysis was performed using the Statistica 9.0 PL program. The type of variable distribution was determined by the Shapiro-Wilk test. For the comparison of quantitative variables between two groups, depending on the distribution of the variable, the Mann-Whitney U or Student t test was used. For more than two groups and variables with an abnormal distribution the ANOVA rank Kruskal-Wallis test was used. The χ2 test was used to compare the frequency of the occurrence of the qualitative variable between the groups.
Results
There were no significant differences in the demographic data between the study and control groups (Table I). The results of exact genotype distributions are briefly summarized in Table II.
Table I
Demographic data
Table II
Genotype distributions in the study population
| Genotype frequency | ||||
|---|---|---|---|---|
| NA | CYPC19*2, n (%) | |||
| 199 | NoF | LoF | ||
| GG | GA | AA | ||
| 49 (24.6) | 147 (73.9) | 3 (1.5) | ||
| 199 | CYPC19*3, n (%) | |||
| NoF | LoF | |||
| GG | GA | AA | ||
| 199 (100) | 0 (0) | 0 (0) | ||
| 199 | ABCB1, n (%) | |||
| GA | PA | |||
| CC | TC | TT | ||
| 32 (16) | 115 (57.9) | 52 (26.1) | ||
There were no CYPC19*3 allele carriers in the entire population.
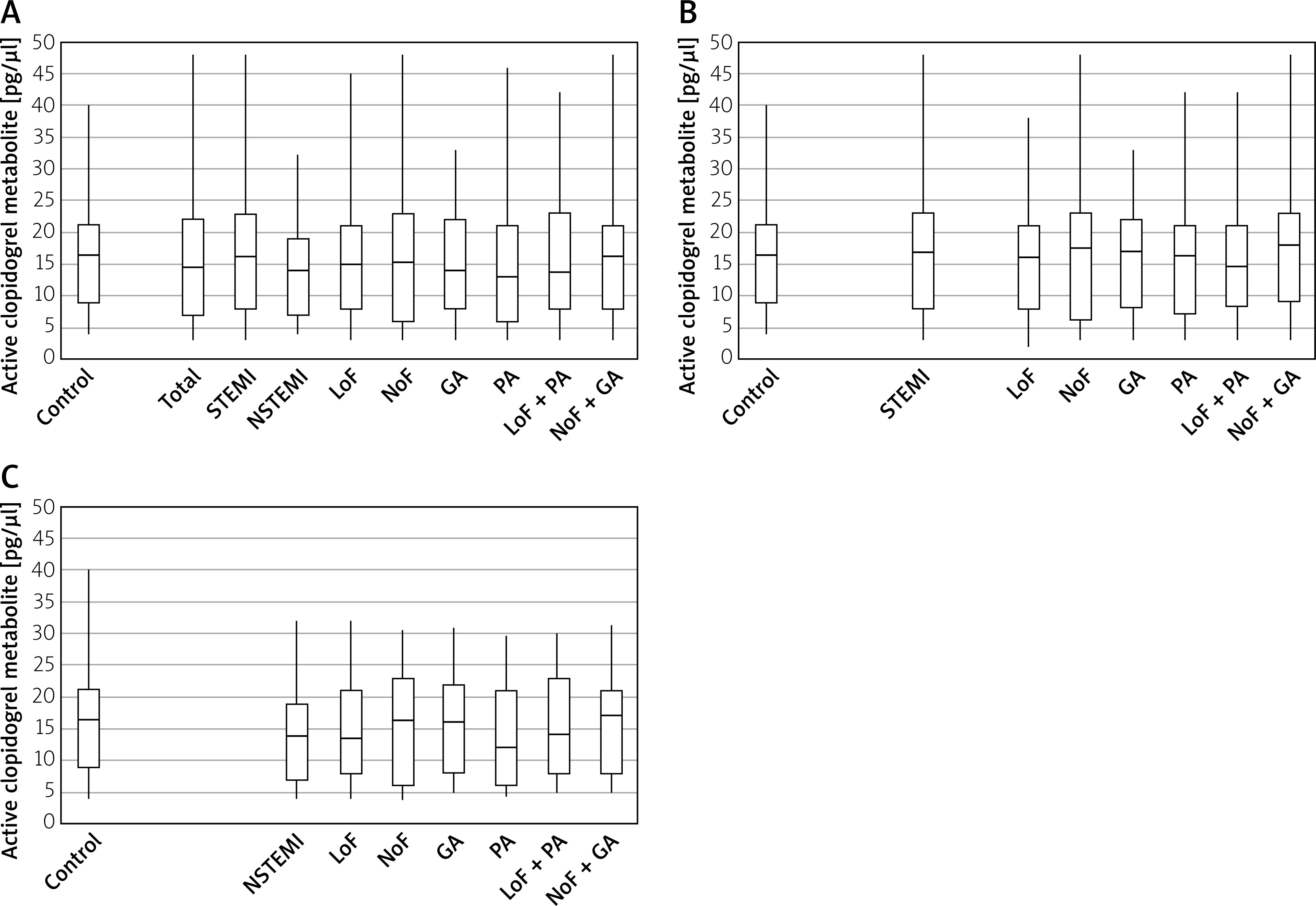
The median (IQR) level of active clopidogrel in 22 controls was 16.7 (9.0–21.1) ng/ml, as compared with 14.9 (6.9–21.9) ng/ml for the whole study group (p < 0.59). A subgroup analysis revealed no differences in the levels of active clopidogrel between patients with STEMI and those with NSTEMI (median (IQR): 16.1 (7.8–23.4) ng/ml and 13.6 (9.5–19.1) ng/ml; p < 0.32). No differences were also noted between patients with STEMI and controls or between those with NSTEMI and controls (p < 0.33 and p < 0.54, respectively). Moreover, the levels of active clopidogrel did not differ between the NoF and LoF groups (p < 0.47) or between the PA and GA groups (p < 0.71). The simultaneous presence of the ABCB1 and CYP2C19*2 polymorphisms (PA + LoF) was not associated with lower drug levels in comparison with the GA+NoF group (p = 0.28). There were no significant differences between the individual genetic subgroups in the whole study population (Figure 1 A) or separately in patients with STEMI and NSTEMI (Figures 1 B, C).
Figure 1
Levels of clopidogrel active metabolite in: A – the whole study group and subgroups; B – patients with ST-segment elevation myocardial infarction (STEMI) and STEMI subgroups; C – patients with non-ST-segment elevation myocardial infarction (NSTEMI) and NSTEMI subgroups
Control – control group, GA – good absorbers, PA – poor absorbers, LoF – loss of function alleles, NoF – normal function alleles, NSTEMI – non-ST-segment elevation myocardial infarction, STEMI – ST-segment elevation myocardial infarction, Total – whole population.
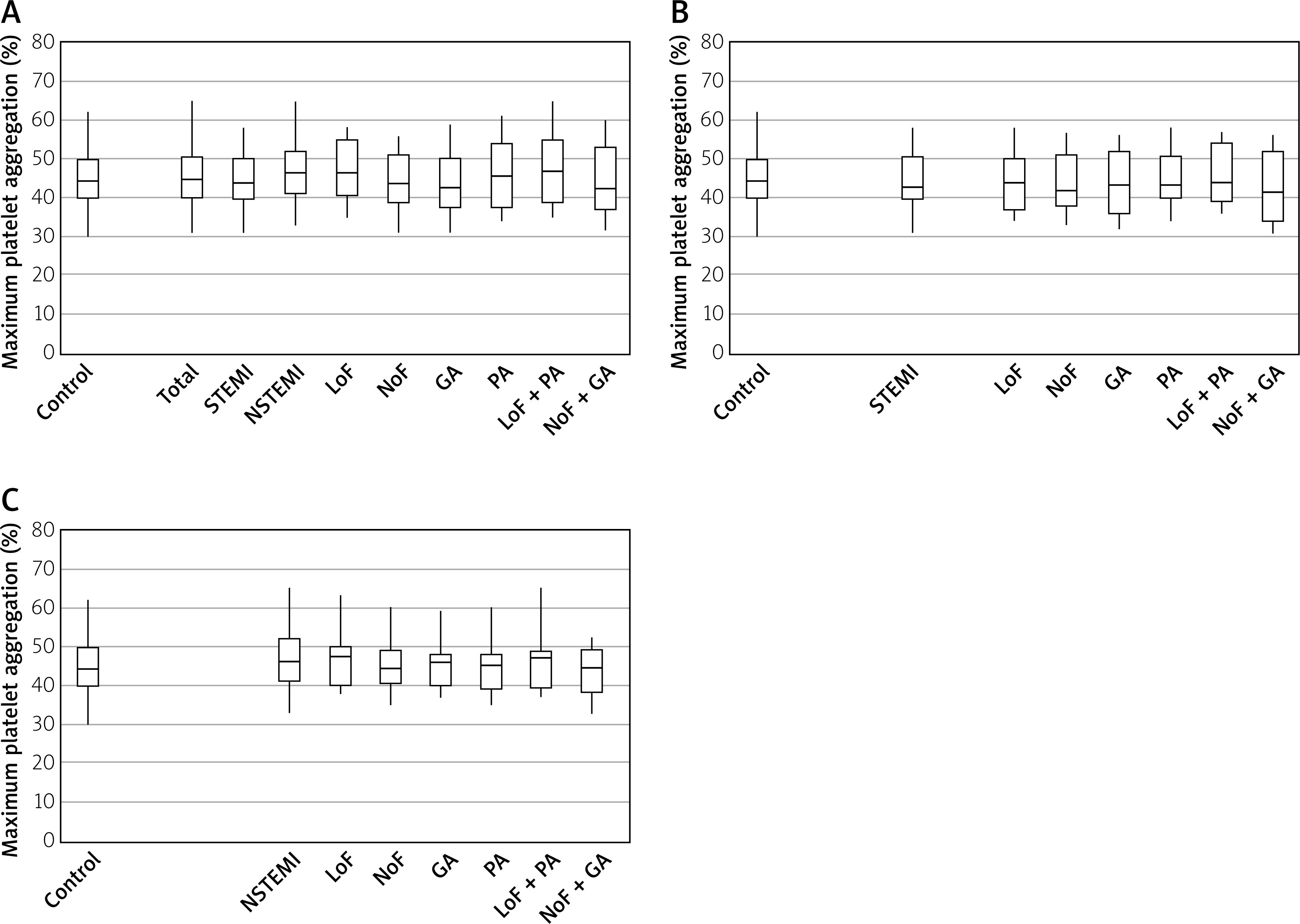
Platelet inhibition, after stimulation with either 5-μmol/l or 10-μmol/l ADP, was similar in all study subgroups as well as controls (Figures 2 A–C, 3 A–C).
Figure 2
Maximum platelet aggregation after stimulation with 5-μmol/l adenosine diphosphate in: A – the whole study group and subgroups, B – patients with ST-segment elevation myocardial infarction (STEMI) and STEMI subgroups, C – patients with non-ST-segment elevation myocardial infarction (NSTEMI) and NSTEMI subgroups
Control – control group, GA – good absorbers, PA – poor absorbers, LoF – loss of function alleles, NoF – normal function alleles, NSTEMI – non-ST-segment elevation myocardial infarction, STEMI – ST-segment elevation myocardial infarction, Total – whole population.
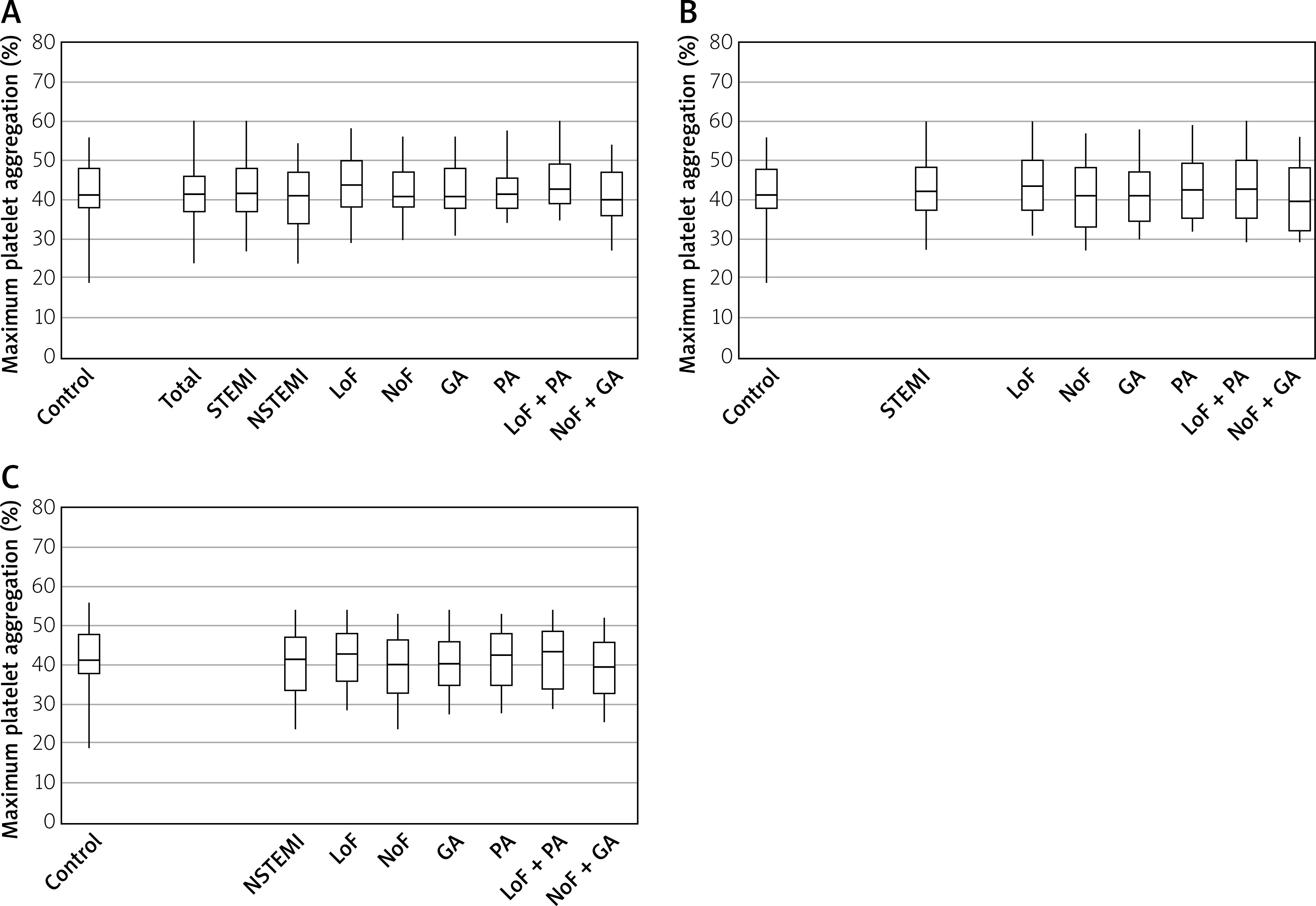
Figure 3
Maximum platelet aggregation after stimulation with 10-μmol/l adenosine diphosphate: A – the whole study group and subgroups, B – patients with ST-segment elevation myocardial infarction (STEMI) and STEMI subgroups, C – patients with non-ST-segment elevation myocardial infarction (NSTEMI) and NSTEMI subgroups
Control – control group, GA – good absorbers, PA – poor absorbers, LoF – loss of function alleles, NoF – normal function alleles, NSTEMI – non-ST-segment elevation myocardial infarction, STEMI – ST-segment elevation myocardial infarction, Total – whole population.
High on-treatment platelet reactivity was noted in 26.7% of controls, as compared with 28.1% of the whole study population (p = 0.89). Moreover, there were no differences in HPR between the STEMI group (29.6%) and controls (p = 0.76) or between the NSTEMI group (27.1%) and controls (p = 0.83).
In a linear regression model including clinical data and genetic analysis, no relationship was found between these variables and the concentration of clopidogrel active metabolite.
Discussion
A short half-life of active clopidogrel complicates the quantitative assessment of its blood levels. To date, only a few high-performance liquid chromatography assays have proved sensitive enough to measure active clopidogrel levels in human plasma [8]. In our study, we used modified methods that allowed us to stabilize the clopidogrel active metabolite in blood [7]. To assess its concentrations, we decided to use LC-MS/MS because it can determine the drug concentrations in blood with high sensitivity and selectivity [9, 10].
The cutoff values for defining clopidogrel nonresponsiveness using aggregometry are often arbitrary. In 2010, Bonello et al. [11] published a consensus statement in which they proposed a 5-μmol/l ADP-induced MPA of 46% as a cutoff value to identify HPR. In our study, we accepted this recommended threshold for MPA induced by 5-μmol/l ADP, while for 10-μmol/l ADP, the cutoff value of more than 67% was used to identify an inadequate response to clopidogrel, similarly to a study by Cuisset et al. [12].
Multiple data suggest that insufficient active metabolite generation is a significant reason for variability in clopidogrel response. High on-clopidogrel platelet reactivity has been reported to be associated with a significantly higher incidence of ischemic adverse effects in patients undergoing PCI. There is evidence suggesting that the severity of the patient’s clinical status significantly affects clopidogrel metabolism, which consequently influences the concentrations and antiplatelet effects of its active metabolite. Among patients admitted to intensive care units, the number of poorly responding individuals was reported to range from 65% to 80% [5]. Generation of the clopidogrel active metabolite was markedly lower than in healthy volunteers or other patient groups [13–15]. In a study by Součková et al. [6], including patients undergoing successful cardiopulmonary resuscitation who received clopidogrel because of a PCI, clopidogrel bioavailability and platelet inhibition were lower than in patients in a stable clinical condition [6].
Our findings show that in patients with lower cardiovascular burden (i.e., patients with STEMI and NSTEMI but excluding those with cardiogenic shock and those with Killip class IV), ACS is not associated with changes in the blood levels of clopidogrel active metabolite or platelet aggregation in comparison with patients with stable coronary artery disease. No differences in the analyzed parameters were also found between patients classified according to the type of ACS (STEMI vs. NSTEMI).
Our data on the incidence of HPR are in line with previous studies, which reported the occurrence of HPR in about 30% of the population [16, 17].
Considering the available data on the possible effect of the CYP2C19 and ABCB1 polymorphisms on the bioavailability of clopidogrel and its antiplatelet effects, we decided to assess platelet aggregation and the levels of clopidogrel active metabolite in combination with genotyping. Precise data on ABCB1 and CYP2C19 genotype distribution observed in our population (summarized in Table II) were published previously [7]. The results were very similar to previous observations in a Caucasian population [18, 19] and confirm poor inspection of the CYP2C19 *3 polymorphism in this part of Europe.
Our study revealed no correlations between ABCB1 and CYP2C19*2 polymorphisms and the drug concentrations or platelet aggregation. Available data on the effect of ABCB1 and CYP2C19 polymorphisms on the concentrations of clopidogrel active metabolite and platelet aggregation are contradictory [20]. The ABCB1 C3435T polymorphism has been associated with changes in the intestinal efflux of drugs and thus their bioavailability [21]. A clinical study in patients undergoing PCI reported that peak plasma concentrations and area under the curve of clopidogrel active metabolite following administration of a loading dose of clopidogrel were significantly lower in 3435T/T homozygotes than those in 3435C/T heterozygotes or 3435C/C (wild-type) homozygotes [22]. However, these results were not confirmed by subsequent studies for the maintenance clopidogrel doses of 75 mg or 150 mg [23, 24]. Our findings are in line with the results of 2 meta-analyses showing that the ABCB1 C3435T polymorphism is unlikely to play a major role in between-subject variability in response to clopidogrel [25, 26].
The available data on the CYP2C19 polymorphism on the blood levels of clopidogrel active metabolite were mostly derived from studies on young healthy volunteers. A major study on the effect of genes on the hepatic metabolism of clopidogrel, conducted in a group of healthy volunteers, demonstrated that the carriers of a mutant allele of the CYP2C19 gene had 32.4% lower plasma levels of clopidogrel and 25% higher platelet aggregation as compared with noncarriers [18]. Similar findings were reported by Kelly et al. [27], who studied 90 healthy young Chinese subjects. We lack big data in an older population with high cardiovascular burden. Only Wang et al. reported that the genetic polymorphisms of CYP2C19*2 and ABCB1 affect the pharmacokinetic and pharmacodynamic responses to clopidogrel in patients with ACS [14]. More convincing data refer only to the effect of the CYP2C19 polymorphism on the clinical course of ACS in patients receiving clopidogrel. However, there is no information on how the polymorphism affects drug concentrations and platelet aggregation. In the TRITON-TIMI 38 trial (Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel–Thrombolysis in Myocardial Infarction 38) the carriers of the CYP2C19 reduced-function allele had an increased risk of ischemic adverse events [18]. Similarly, studies reported that CYP2C19 reduced-function alleles were associated with worse clinical outcomes, including cardiovascular death, myocardial infarction, and stroke [28–31]. This observation has been confirmed by several meta-analyses [32–34].
Importantly, also in our research healthy volunteers without CYP2C19*2 and ABCB1 polymorphisms had higher levels of clopidogrel active metabolite (p < 0.001) and reduced platelet aggregation (p < 0.05), as compared with ACS patients (in press). This may suggest that the effect of genetic polymorphism on drug concentrations and platelet aggregation is much more notable in younger and more homogeneous populations, while other factors, such as age, diabetes, renal insufficiency, and the use of multiple medications, including other cytochrome p450-metabolized drugs [18], have a significantly greater effect on reduced bioavailability and antiplatelet effects of clopidogrel in older and more heterogeneous groups, thus masking the possible influence of genetic variability. This may partially explain why prospective randomized trials have failed to demonstrate the efficacy of personalized antiplatelet treatment based on platelet function in reducing the frequency of ischemic events [35–39].
Our study has several limitations. First, we included a relatively small cohort of participants from a limited geographic region. We have to admit that the study’s sample was not powered sufficiently to formulate final conclusions, and thus our findings need to be corroborated with more statistically powerful studies. Second, we did not assess other genetic polymorphisms or other factors (diabetes, smoking, drug use) that might have affected the drug concentrations. Moreover, considering that the we did not find any CYP2C19*3 allele carriers, and homozygous carriers of the CYP2C19*2 allele constituted only 1.5% of our study population [8], it was difficult to assess the effect of this genetic variant on the analyzed parameters. Therefore, the relationship between these genotypes and exposure to the active metabolite of clopidogrel and the corresponding pharmacodynamic effects should be confirmed in larger cohorts.
Conclusions
Our study showed that ACS is not associated with the levels of clopidogrel active metabolite or platelet inhibition in patients with Killip class I-III, and this lack of association was not affected by the presence of ABCB1 and CYP2C19*2 gene polymorphisms. This suggests that clopidogrel may be safely used in this population in the presence of contraindications to prasugrel or ticagrelor treatment.







