
Introduction
Obesity is a chronic systemic metabolic disease resulting from disturbances in the body energy homeostasis [1]. The energy balance is disturbed in children and adolescents as a result of excessive energy intake and reduced energy expenditure [2].
The World Health Organization recognized obesity as an epidemic of the 21st century [3]. The greatest increase in the prevalence of overweight and obesity is observed in the 5–19-year-old age group. According to world data, in 1975 the prevalence was 4%, and in 2016 the group of overweight and obese children increased to 18% [4]. Similar observations have been made in Poland by Kułaga et al. in the nationwide OLAF and OLA studies in 2007–2012 [5]. The researchers found excess body weight in 18.7% of boys and 14.1% of girls at school age (7–18 years), and in 12.2% of boys and 15% of girls at preschool age (2–6 years). Obesity carries a risk of metabolic and cardiovascular complications, as well as emotional and psychosocial problems [6]. Many environmental factors have been proven to cause excess weight gain in children. As well as lack of physical activity, improper eating habits is one of them. A family history of obesity also plays an important role, and maternal obesity is considered one of the most important factors [7]. This particular role of mothers in the development of childhood obesity manifests itself mainly in influencing the food preferences of their offspring. A strong influence of mothers’ habits on their children’s habits was demonstrated in the case of preferences and consumption of fat [8], variety of eaten vegetables [9], consumption of milk [10], and adherence to dietary restrictions [11]. The diet in the family home determines what habits children will adopt and what their diet will look like in adult life [12]. Due to the prevalence of obesity, the authors designed a study to assess eating habits in families of children with excess body weight.
Aim of the study
The aim of the study was to analyse the relationship between the selected eating habits of mothers and the eating habits of their children with excess body weight before and after dietary intervention.
Material and methods
In the study 94 children with excess body weight were qualified. They were patients of the Department of Paediatrics, Endocrinology, Diabetology, Metabolic Disorders, and Cardiology of Developmental Age of the Pomeranian Medical University in Szczecin, in whom diagnostics was planned due to excess body weight. Because 68 children completed the study, the calculation data apply to this group. For the nutritional analysis, 67 questionnaires of children and mothers before and after dietary intervention were used. One mother did not complete the questionnaire and one child did not give information about the cooking technique. The participation of patients in the study was voluntary. From parents of children under 13 years of age and from study participants over 13 years of age and their parents, informed consent to participate was obtained. The study protocol was approved by the Bioethics Committee at the Pomeranian Medical University in Szczecin (No. KB-0012/34/11 of 16 May 2011).
Children with the following were excluded from the study:
congenital syndromes predisposing to obesity (Down syndrome, Prader-Willi syndrome),
thyroid disorders,
adrenal gland dysfunction,
gonadal dysfunction,
intellectual disability,
chronic illnesses required pharmacological treatment, such as steroid therapy, metformin therapy.
To assess the nutritional status the body mass index (BMI) was used. It was compared to the Polish norms for the population of children and adolescents developed in the OLA and OLAF projects. A BMI ranging from the 85th to 95th percentile was considered as overweight and over the 95th percentile was considered as obese. The cut-off points defining overweight and obesity are consistent with the International Obesity Task Force (IOTF) criteria [13]. The values of body weight and height as well as BMI were standardized according to the mean and standard deviation (SD), obtaining normalized data (in SDS) [14]. Overweight was defined as BMI ≥ 1 SDS and obesity as BMI ≥ 2 SDS.
The study used the dietary survey method and the research tool, which was the author’s questionnaire, for assessing eating habits and intake frequency. The part of the survey on nutrition was preceded by questions relating to the socio-demographic characteristics of the respondents and the anthropometric parameters of mothers and children. The eating habits questionnaire consisted of 30 questions. In the questions about the meal consumption frequency, a 7-point scale was used for evaluation, where the answer ‘several times a day’ received 6 points, ‘once a day’ – 5 points, ‘several times a week’ – 4 points, ‘once a week’ – 3 points, ‘several times a month’ – 2 points, ‘once a month’ – 1 point, and ‘not at all’ 0 – points and a 3-point scale of answers, where the answer ‘with each meal’ received 2 points, ‘not with each meal’ – 1 point, and ‘not at all’ – 0 points. Children under 13 years of age completed the questionnaire with their mothers, and over 13 years of age alone or with their mothers’ help.
Patients participated in 6 individual educational meetings over a period of 12 months. The first 3 follow-up appointments took place once a month, whereas the fourth, fifth, and sixth follow-up appointments – once every 3 months. For the sixth follow-up visit, patients and their mothers were re-invited to the clinic for check-ups and assessment of their eating habits. At each appointment, mother and child pairs were re-educated, and nutrition errors were corrected based on the established changes in eating behaviour. The eating habits were assessed in children and mothers before and after dietary intervention.
For the nutrition education of the participants, a pattern of correct health-related behaviour was used, resulting from the current recommendations on proper nutrition such as the Healthy Eating Pyramid and the 10 Principles of Healthy Nutrition for Children and Youth by the Food and Nutrition Institute in Warsaw from 2009 [15].
The study which I conducted had some limitations. The lack of a control group on the usual diet made it impossible to compare the effect and strength of the interventions undertaken. On the other hand, all children with both overweight and normal body weight and their families should have the same opportunity to obtain advice on dietary recommendations under current guidelines. In addition, the size of the patient group was limited due to the time-consuming form of individual education.
The parameter values were compared between the groups with the exact 2-tailed Fisher test for dichotomous variables and the Mann-Whitney U test for measurable and rank variables. Correlations between measurable and rank variables, including the frequency of consumption of certain foods and the degree of nutrition, were assessed by calculating the Spearman’s rank correlation coefficient (rs). P < 0.05 was adopted as the threshold of statistical significance. Statistical calculations were made with the use of Statistica 13 software.
Results
The study was completed by 68 (72,3%) children aged 4–17 years (mean 12.4 ±3.7 years) including 37 (54.4%) girls and 31 (45.6%) boys. Before dietary intervention, in 8 children (11,8%) BMI was ≥ 85 percentile – < 95th percentile, and in 60 children (88.3%) ≥ 95th percentile. After dietary intervention, 22 (32%) children had BMI ≥ 85th percentile – < 95th percentile, and 46 (68%) children had BMI ≥ 95th percentile. When assessing SDS BMI before dietary intervention 59 (87%) children were diagnosed with obesity and 9 (13%) were overweight. After completing the nutrition education programme, based on SDS BMI, 45 (66%) children were diagnosed with obesity and 23 (34%) were overweight. A significant improvement in weight reduction was observed in children. Before dietary intervention the mean SDS for BMI was 3.7 ±1.7, and after dietary intervention 2.9 ±1.7 (p ≤ 0.00001).
The level of education of the children’s mothers was varied. Fewer than half of them had secondary education (44.3%), 31.8% completed higher education, and 11.4% and 12.5% had vocational and primary education, respectively. The vast majority of the mothers (77.4%) were economically active whereas 22.6% were unemployed. In the study group, 69.6% of the children lived in a city, and 30.4% in the countryside. Among the mothers participating in the study, 75% had excess body weight and 25% had a good nutritional status. After dietary intervention 69% of mothers has excess body weight and 31% had a good nutritional status. In the present study, the influence of dietary intervention on the BMI found in mothers of overweight and obese children was “close to statistical significance” (p = 0.054).
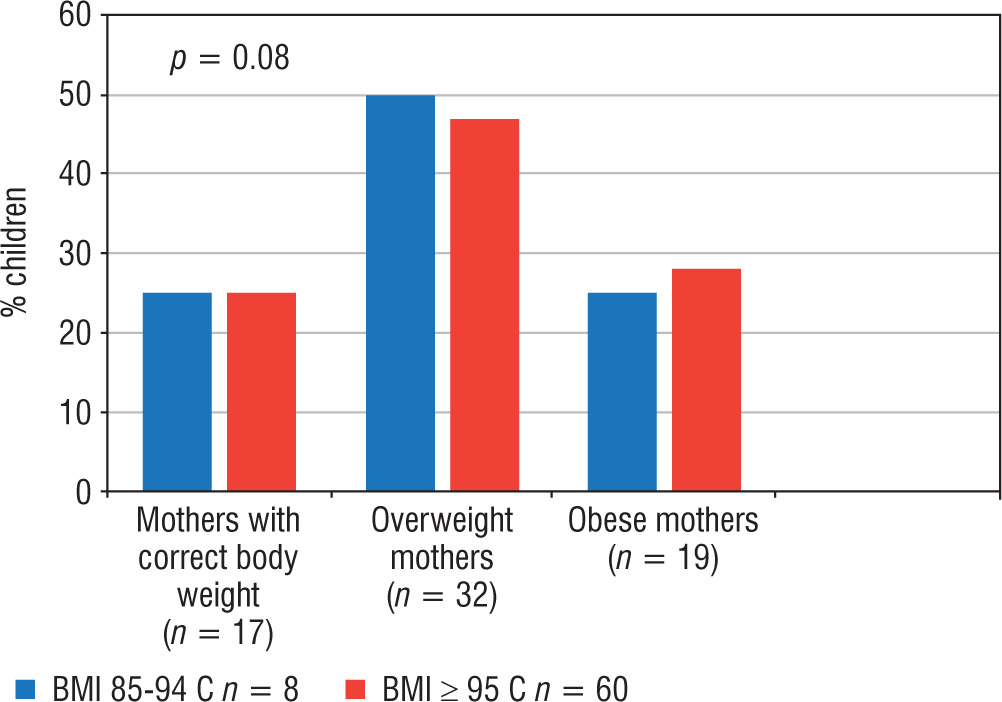
Before dietary intervention, the relationship between the nutritional status of mothers and the prevalence of overweight and obesity in their children was analysed. No correlation was demonstrated (p = 0.08; Figure 1). Moreover, the BMI of mothers of overweight children and the BMI of mothers of obese children were assessed before dietary intervention. The BMI of mothers of obese children was significantly higher than that of mothers of overweight children (respectively: x_ 27.9 ±4.9 vs. x_ 23.7 ±4.9; p = 0.009).
Figure 1
Prevalence of overweight and obesity in children before intervention depending on the nutritional status of their mothers
p – statistical significance
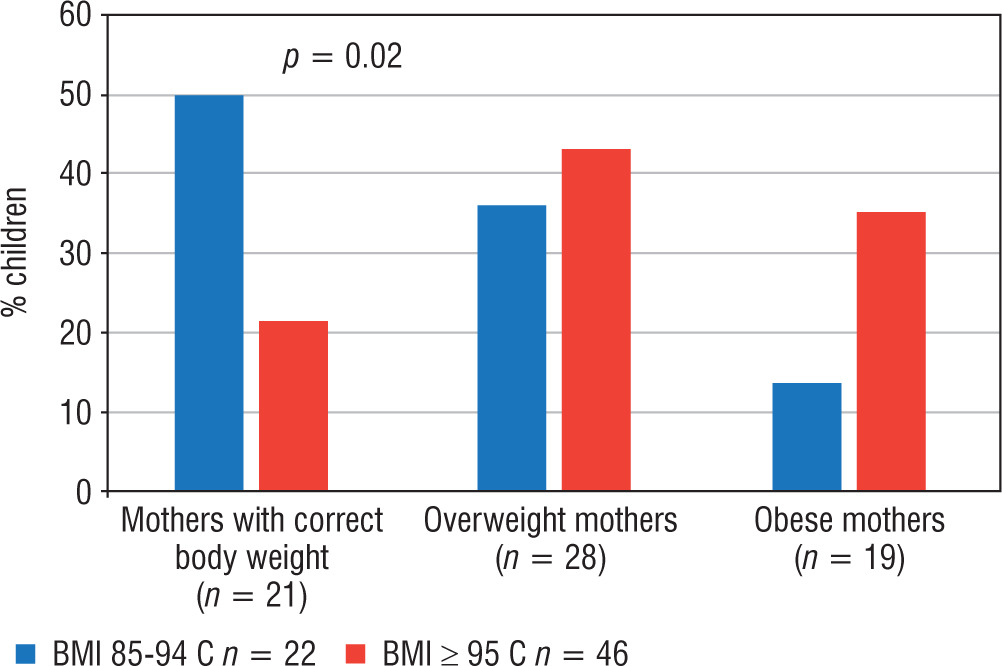
The impact of maternal nutrition on the incidence of obesity and overweight in their children was also assessed. After dietary intervention, more frequently there was a body mass reduction in children of mothers with normal body weight than in children of overweight and obese mothers (p = 0.02). The above data are presented in Figure 2. Moreover, the difference in the BMI of mothers of overweight children and mothers of obese children after dietary intervention was assessed. The BMI of mothers of obese children was higher compared to the BMI of mothers of overweight children (respectively: x_ 28.9 ±4.8 vs. x_ 25.4 ±5.5; p = 0.01).
Figure 2
Prevalence of overweight and obesity in children after intervention depending on the nutritional status of their mothers
p – statistical significance
The impact of mothers’ nutritional behaviour and diet on their children’s nutritional behaviour and diet was statistically analysed before and after dietary intervention. The study group showed a number of significant correlations between mothers’ and their children’s habits in the analysed period. The results are shown in Tables I–VI. The presented data show that the maternal influence on the nutritional behaviour of children was slightly more visible before dietary education. This influence concerned both incorrect and correct nutritional behaviour. Before dietary education, there was a significant relationship between mothers’ correct habits and children’s habits of eating breakfast, drinking water (Table II), consuming milk (Table III), and using fat of plant origin in preparing meals (Table VI). The significant influence of mothers on subsequent correct nutritional behaviours of children, such as liking vegetables, choosing natural dairy products, or eating wholemeal pasta, was visible after dietary education (Tables II–IV). As for the consumption of multigrain cereal products, i.e. oatmeal, brown rice, or buckwheat, the correct nutritional choices of mothers before dietary intervention continued to influence their children’s nutritional choices after dietary education (Table IV). The same was observed with the habit of using fat-free culinary techniques and choosing the right type of meat in terms of nutritional value (Table VI). However, mothers’ incorrect food choices before dietary education, which still influenced the incorrect food choices of their children after dietary intervention, concerned, among others, the frequency of eating sweets and fast-food (Table I), consumption of sweetened breakfast cereals (Table IV), choosing an inappropriate type of meat in terms of the nutritional value, and choosing culinary techniques with the use of fat (Table VI). Additionally, before dietary intervention, an incorrect influence of mothers’ habits on their children’s habits was noted in the case of eating wheat bread and white rice (Table IV). It is worth noting that despite the dietary intervention, the influence of negative mothers’ habits on the habits of their children regarding snacking after dinner, drinking sweet beverages, and using animal fat in preparing meals was still observed (Tables II, IV, V). Before and after dietary meetings, there was a significant relationship between mothers’ habits and children’s habits in terms of the number of meals eaten, the frequency of eating fruit, cereal products, and fish as well as the self-assessment of the adherence to healthy eating habits (Table I). In the present study, only one habit showed a negative relationship between the mother’s habit and the child’s habit. It was related to the consumption of sweetened dairy products before dietary intervention (Table III). No significant relationships were found for other eating habits.
Table I
The relationship between the number of meals, frequency of consumption of selected products, and self-assessment of mother’s and child’s eating habits
Table II
The relationship between mothers’ habits and the habits of children with excess body weight before and after dietary intervention
Table III
The relationship between mothers’ consumption of selected dairy products and the consumption of the same prod- ucts by their children
Table IV
The relationship between the habit of consuming selected cereal products by mothers and the habit of consuming these products by their children before and after dietary intervention
Table V
The relationship between the habit of consuming selected types of meat by mothers and the habit of consuming these products by their children before and after dietary intervention
Discussion
Obesity and overweight in the paediatric population remains an unresolved problem, and due to the risk of secondary metabolic complications, mainly in the area of lipid and carbohydrate metabolism, it cannot be ignored.
We know that children’s diet is related to their parents’ diet [16–18]. Many authors emphasize the special role of mothers in shaping children’s nutritional behaviour [19]. A European study involving 8 countries assessed the relationship between parents’ and children’s eating patterns and showed that children mostly followed the same eating patterns as their mothers [20]. In the present study, a lot of children’s eating habits were related to their mothers’ habits. It was noted that there was a significant influence of mothers’ unhealthy eating habits regarding the consumption of, e.g., sweets, fast food, drinking sweet beverages on the consumption of these products by their children. Similar observations were made by Fernando et al. [21], who noted that the availability of unhealthy food at home became a strong factor contributing to obesity in children, even if their mothers had relatively high nutritional knowledge.
The degree to which the diet of caregivers affects the diet of children can be seen in the consumption of cereal products. The authors’ own study showed that mothers who more frequently ate cereal products also gave them to their children. Mothers’ nutritional preferences regarding the quality of cereal products were not always consistent with the principles of healthy eating. Apart from the influence of the correct maternal habit on the children’s habit of eating buckwheat, wholemeal pasta, and brown rice, it was also shown that there was an influence of mothers’ habits which were inconsistent with the principles of healthy eating on the children’s habits of eating white rice, wheat bread, and sweetened breakfast cereals. Despite their education, mothers continued to establish or did not change their children’s habits of consuming refined or flavoured cereal products. Whole grain cereal products take an important position in the food pyramid and in a child’s diet. They should be permanently included in the daily menu. Low consumption of whole grain cereal products was noted by Okręglicka and Bawa, who analysed the habits of obese children aged 7–13 years [22]. Whole grain cereal products are a better source of B vitamins, zinc, magnesium, and fibre, which delays glucose absorption, lowers the caloric content of the diet ,and has a positive effect on lipid metabolism, which is of key importance for the studied group of children [2The occurrence of eating errors and the repetition of incorrect habits by parents who have a certain amount of knowledge about proper nutrition may most often be the result of parents’ reluctance to change their own attitudes [24, 25]. Despite the dietary education, in the discussed study, such behaviour can be seen in the habit of snacking after dinner. It is worth noting that snacking is a frequent, incorrect eating habit not only in overweight and obese children [26]. This is a highly undesirable phenomenon because children who frequently snack between meals, including after dinner, do not recognize the signals regulating their appetite and often do not experience the feeling of fullness during the day or hunger after waking up [27].
The study by Brown and Ogden [28] showed how parents’ eating behaviour influences their children’s eating behaviour. Parents and children with normal body weight were assessed in the context of eating healthy and unhealthy snacks and the impact of parents’ eating behaviour and attitudes on children’s eating behaviour and attitudes. A strong relationship between the studied features was demonstrated, and a conclusion was drawn that a positive attitude of the parent towards changing eating habits is a better method of improving the diet than just trying to control it. It is worth noting that the effectiveness of the therapy of children with excess body weight increases if their parents also decide to improve their own diet. Similar observations were made by Patrick et al. [29], who assessed the eating style of caregivers and preschool children. They proved that interventions aimed at increasing children’s consumption of milk, fruit, and vegetables should be aimed at increasing the authoritative nutritional behaviour of caregivers. In my study, the parents’ eating habits of consuming refined cereal products, drinking sweet drinks, not eating fish, or using animal fat-based frying techniques were stronger than knowledge of their negative or health-promoting effects on the body.
On the basis of the conducted research, it was found that only a few eating habits of mothers improved after dietary intervention. There was a significant and beneficial change in mothers and children after dietary intervention in terms of consuming the right number of meals and amount of fruit throughout the day as well as choosing natural dairy products. Probably mothers who consumed the right number of meals and the appropriate amount of fruit during the day and who also more often chose natural dairy products, made sure their children also ate meals with the right frequency and consumed a sufficient amount of fruit.
Relationships between the correct habits of mothers and children may suggest that the ability to communicate, solve problems, and positively reinforce was well developed, which influenced a change in eating behaviour. In my study, positive relationships were found for most eating habits, but not all of them were consistent with the principles of healthy eating. A similar relationship has been presented in other studies [30, 31].
There was no effect of the mother’s habit on the child’s eating habits regarding the frequency of consuming vegetables before and after dietary intervention. Researchers claim that the reason for this is excessive parental pressure on children to eat vegetables, which may generally arouse reluctance to eat them [32].
What is interesting is that some of the mothers’ correct eating habits, which influenced the dietary habits of their children before dietary intervention, such as eating breakfast, drinking water, using vegetable fat, or consuming milk, did not affect the children’s habits after dietary intervention. A family similarity in the consumption of dairy products (including milk) was observed by Sobaś et al. [33]. They showed that low consumption of dairy products by mothers was strongly associated with low consumption of dairy products by daughters. Reluctance to consume milk seems to be widespread not only in the population of obese children, but also in the healthy weight group. Łaboda and Gawęcki [34], while examining eating habits among junior high school students, demonstrated that an average of 80% of the respondents showed a reluctance to consume milk. The likely cause of this disturbing fact was the increase in consumption of sweetened drinks by children [35]. In my study, children whose mothers consumed sweetened beverages more often after dietary intervention were also found to consume sweetened beverages more frequently.
Parents play a key role in the diet of their children in the early stages of their lives. Children rely on caregivers for food choices and availability. Thanks to their parents, they learn a taste for certain foods by accepting them, and reluctance to others by rejecting them. In the process of slimming, self-confidence is one of the most difficult variables, especially in children [36]. The role of parents in shaping correct eating habits, as well as in supporting, motivating, and demonstrating correct eating behaviour by their own example is very important. The present study proved that combined parent-child intervention is possible and effective. Working with overweight and obese parents as well as parents with healthy body weight can bring the expected results. The expected effect is a statistically significant in children but also a change in incorrect eating habits of mothers and their children
Educational activities should focus on parental involvement and not only on recommendations given to the child. Joint educational programs, which are part of the so-called behavioural intervention, give positive results, which is confirmed by the opinion of mothers and children who positively assessed their diet after dietary intervention. Researchers also underline the role of all family members, including fathers and grandparents, in the increase in obesity in children [37–39], thus pointing to the need to conduct studies that analyse not only the role of mothers in shaping children’s eating habits.
Table VI
The relationship between selected eating habits with regard to cooking techniques and the type of fat used by mothers and cooking techniques and the type of fat used by their children before and after dietary intervention
During the intervention, a group of 26 patients (28%) withdrew from participating in the study at various stages of its duration. High rates of resignation from participation in the body mass loss programme are well documented in the literature, ranging from 27% to 73%, and family factors are considered the reasons for resignation [40]. Similar observations were made in this study. The fact that not all the patients completed the program probably resulted from the need for a huge time commitment of children and parents, and frequent checks during the 12-month study period. It was noticed that people who resigned were characterized by a lower degree of motivation to change eating habits and reduce body weight compared to those who stayed in the study until its end.
The example of the participants who completed the dietary education programme showed that educational activities aimed at family change of eating habits have a positive effect on their improvement. In addition, the conducted study found that not all children’s habits were related to their mothers’ habits, and the dietary education showed an unequal effect on their change.
Conclusions
The influence of selected correct and incorrect mothers’ eating habits on shaping the eating habits of their children with excess body weight before and after dietary intervention was demonstrated. Before and after dietary intervention, this concerned the number of eaten meals, the frequency of consuming sweets, fast food, fruit, fish, oatmeal, sweetened breakfast cereals, buckwheat, brown rice, pork, and beef as well as the choice of culinary techniques used for preparing meals.
No relationship was found between mother and child in the frequency of consumption of vegetables, both before and after dietary intervention.
It is necessary to provide thorough and comprehensive dietary education to mothers of obese children.
Dietary education with the use of the nutritional patterns such as the Healthy Eating Pyramid turned out to be an effective tool used to change mothers’ and children’s eating habits and body mass reduction in children.









