
Introduction
Hypertension was defined by Geoffrey Rose as blood pressure values at which the benefits of treatment clearly outweigh the risks [1]. According to current guidelines of the European Society of Cardiology (ESC) and the European Society of Hypertension (ESH) those values are ≥ 140 mm Hg and/or ≥ 90 mm Hg, respectively for office systolic and diastolic blood pressure [2]. Epidemiological data indicate differences in prevalence of hypertension in men and women depending on age. On the Figure 1 we present the results of polish population study WOBASZ II [3].
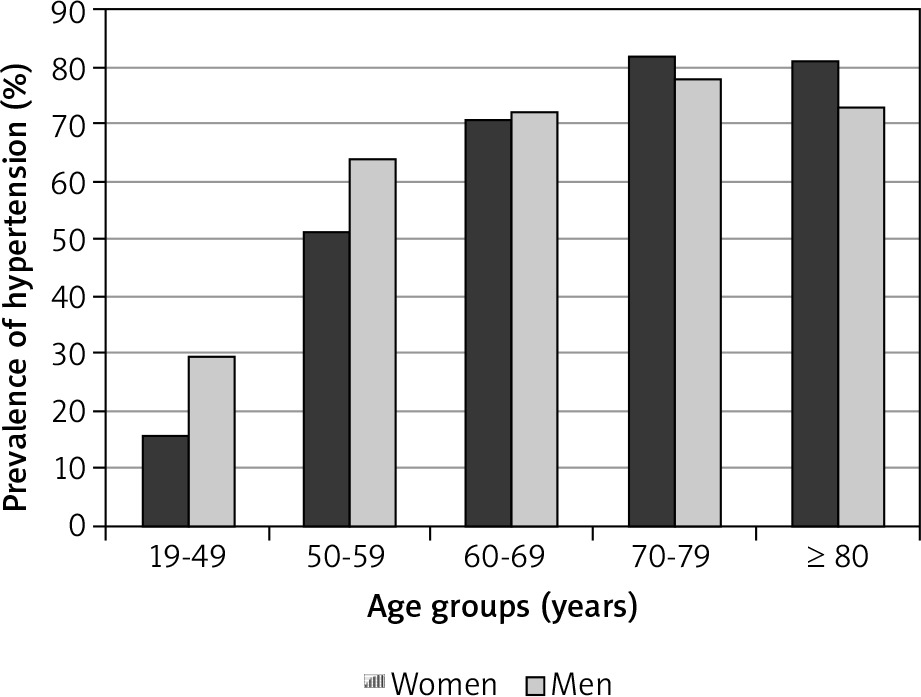
In women, a remarkable increase in blood pressure is observed after the menopause [4]. Hormonal changes are indicated as one of the factors that contribute to onset of hypertension in this group. The decrease in estradiol concentration and estrogen/testosterone ratio affects endothelial function. Menopause is also associated with:
However, the confounding effect of aging and comorbidities should be taken into account [4, 8].
Current guidelines do not recommend any specific treatment of post-menopausal hypertension [2]. Despite the known activity of sex hormones the short terms studies do not confirm the efficacy of hormonal replacement therapy (HRT) in hypertension [8]. In consequence HRT is not recommended for primary or secondary prevention of cardiovascular disease [2].
This study aimed to assess the influence of gender on the outcome of hypertension treatment in patients above 40 years old.
Material and methods
Data for this retrospective, single-center study were collected from the disease cards of hypertensive pharmacologically treated patients hospitalized on the cardiological ward. 268 patients, aged over 40 (41-90), were divided into two groups: women and men. Basic characteristic of studied groups of patients (194 women, 74 men; p < 0.001) is presented in Table 1.
Table 1
Basic characteristic of the studied groups of patients
| Parameter | M | Me | SD | Min | Max | |
|---|---|---|---|---|---|---|
| Age | Women | 66.01 | 66 | 11.19 | 41 | 90 |
| Men | 62.51 | 63 | 9.23 | 42 | 83 | |
| BMI | Women | 29.35 | 28.73 | 5.74 | 15.99 | 47.18 |
| Men | 30.84 | 30.35 | 4.75 | 21.95 | 44.71 | |
In Table 2 are presented the mean values (±SD) of blood pressure and heart rate.
Table 2
Blood pressure and heart rate in studied groups of patients
| Parameter | Women | Men | p |
|---|---|---|---|
| Systolic pressure (mm Hg) | 143.95 ±19.65 | 147.39 ±17.11 | 0.14 |
| Diastolic pressure (mm Hg) | 80.19 ±11.5 | 86.94 ±14.3 | < 0.001 |
| Heart rate (beats/min) | 74.2 ±10.32 | 76.9 ±12.21 | 0.06 |
Concentrations of lipids and triglycerides in blood of studied patients are presented in Table 3.
Table 3
Serum concentrations of cholesterol and triglycerides in studied groups of patients
Additional data regarding compliance and efficacy of treatment one year after hospitalization were obtained in phone interview.
Statistical analysis was performed using the IBM SPSS Statistics 25 package. In order to check if there are statistically significant differences between two independent groups of people, the Mann-Whitney U test was used. The chi-square test analysis was performed to check whether the compared groups of people are equal, as well as to check whether there is a statistically significant relationship between nominal variables. The results were considered statistically significant when the probability value (p) was below 0.05.
Results
We analyzed the collected data in term of comorbidities. The significant differences between studied groups were noted only in the frequency of hyperlipidemia, that was more often in men. The results are presented in Table 4.
Table 4
Comorbidities in studied groups of hypertensive patients
The evaluated groups did not differ significantly in the occurrence of left ventricular hypertrophy (54 women (28.1%) vs. 20 men (28.2%), p = 0.55) and edemas (20 women (10.4%) vs. 10 men (13.5%), p = 0.3). Regarding medical history of cardiological interventions the only significant difference was observed in the frequency of coronary artery bypass graft (CABG), that was more often in men. The collected data are presented in Table 5.
Table 5
Cardiological interventions in studied groups of patients
| Parameter | Women | Men | p |
|---|---|---|---|
| PCI | 13 (6.7%) | 10 (13.5%) | 0.08 |
| CABG | 2 (1%) | 7 (9.5%) | 0.001 |
| Pacemaker | 5 (2.6%) | 0 (0%) | 0.19 |
We compared the pharmacological treatment of hypertension in the studied groups. There were no differences in the classes of taken medications between the sexes except alpha-blockers, which is associated with the use of this group of drugs also in prostate diseases. The classes of medicines used by the females and males are summarized in Table 6.
Table 6
Pharmacological treatment of hypertension in the studied groups
We performed also additional analysis of hypertensive treatment in subgroups aged 41-65 (96 women and 47 men) and over 65 (98 women and 27 men). In the age group 41-65 years significantly more women than men are taking thiazide-like diuretics. Other significant differences are observed in intake of loop diuretics, calcium channel blockers and alpha-blockers, that are taken more often by men. The classes of medicines used by the females and males aged 41-65 are summarized in Table 7.
Table 7
Pharmacological treatment of hypertension in the studied subgroups of women and men aged 41-65
In the age group above 65 years there were no differences in the classes of taken medications between the sexes except alpha-blockers. The classes of medicines used by the females and males aged over 65 are summarized in Table 8.
Table 8
Pharmacological treatment of hypertension in the studied subgroups of women and men aged over 65
Significantly more men than women in studied groups have been using combined products (24 men, 32.4% vs. 40 women, 20.6%; p = 0.03) and statins (54, 73% vs. 118, 60%; p = 0.04).
The results of the usage of antiplatelet/antithrombotic and cholesterol lowering medications are presented in Table 9.
Table 9
Usage of antiplatelet/antithrombotic and cholesterol lowering medications in the studied groups
| Class of medicine | Women | Men | p |
|---|---|---|---|
| Antiplatelet/antithrombotic | 121 (62.7%) | 52 (70.3%) | 0.16 |
| Statin | 118 (60.8%) | 54 (73%) | 0.04 |
| Other cholesterol lowering | 8 (4.1%) | 5 (6.8%) | 0.27 |
To collect additional data regarding compliance and efficacy of treatment after hospitalization we have conducted phone interviews one year after hospitalizations. We did not observe any significant difference in the willingness to participate in follow-up between women and men (146, 75.3% vs. 57, 77%, respectively; p = 0.45). There were also no differences in percent of patients with strict and mild control of hypertension, compliance and CV hospitalizations between males and females. The results of the follow-up are presented in Table 10.
Table 10
Follow-up results in studied groups of patients
Discussion
We focused on the role of gender in the treatment of hypertension in patients aged over 40. Medicines used in studied groups were mainly beta-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, diuretics and calcium channel blockers. It is consistent with current guidelines on management of arterial hypertension [2]. The only significant difference was observed in the frequency of alfa-blocker use. This is obviously caused by the usage of this drug class in men in the pharmacotherapy of prostatic hyperplasia [9]. We observed also the significant more frequent use of statins in group of men, that is consistent with higher prevalence of hyperlipidemia in studied group of men.
Although the combined products are strongly recommended by the guideline [2] less than 1/3 of studied patients have been using such preparations. We also observed the significant difference between women and men in this aspect. Significantly more men than women have been using combined products. There are evidences that use of the combined products improves compliance [10, 11], however we failed to observe this effect in our study.
We did not observe any statistically significant differences in term of compliance and efficacy of treatment between women and men. Previous studies on the influence of gender on patients compliance gave inconsistent results [12].
Based on the data from the National Health and Nutrition Examination Survey, Bautista found that male gender predisposes to non-persistence with antihypertensive therapy (OR 1.52; 95% CI: 1.23-1.89; p < 0.001). Lack of persistence increase also significantly with younger age. Comparing the data of patients over 40, those aged 40-49 are 2.25 times more likely to be non-persistence than those over 50 [13] In another study Ambaw et al. confirmed the correlation between male gender and lower adherence to antihypertensive treatment (AOR 0.48; CI: 1.19-3.43). The overall adherence in the studied group was 64.4%. Among 142 men 87 adhered to treatment, while among 242 women adherence were observed in 161 cases [14].
Whereas Angell et al. investigated factors affecting the control of hypertension in treated patients, aged over 20. They found that gender does not have significant effect on efficacy of therapy. In group of treated patients 65.5% (56.2-73.7%) of men and 64.3% (56.0-71.8%) of women had the hypertension controlled. Instead age was the factor that had negative impact on controlling blood pressure. In the group of patients over 65 years was reached significant lower probability to have controlled hypertension than in adults aged 20-44 years. In the group of patients 45-64 the probability was also lower than in younger patients but the difference was not statistically significant [15].
This discrepancies may be a result of different investigation strategies. Efficacy of treatment is related to many factors including compliance. In clinical trials conducted to confirm the effect of medication on lowering blood pressure studied group is homogenous and intake of medicines is strictly controlled. In data obtained from the observational studies it is not possible to eliminate some confounding factors, so there is the risk of bias related to selected participants.
When formulating the conclusion the limitation of the phone interview should be taken into account. Probably more patients declare compliance than really adhere to the treatment. However the answers to the first two questions of interview, regarding the obtained blood pressure values, show more objective that efficacy of pharmacotherapy in studied groups is similar.








