
Thymoma is a neoplasm arising from the population of thymic epithelial cells. It is the most commonly found primary entity in the anterior mediastinum, comprising up to 50% of all mediastinal tumors in adults and 82% of thymus tumors. However, thymomas constitute only about 1% of mediastinal masses in children, making them exceedingly rare in this age group. They usually occur in patients between 40 and 80 years of age, approximately equally often in men and women [1]. Clinically, thymomas are slow-growing, encapsulated neoplasms that tend to invade adjacent tissues, especially the pleura, pericardium and lung. Extrathoracic metastases are rare; they may occupy the kidney, liver, bone and brain. The majority of patients remain asymptomatic and the tumor is detected incidentally during chest imaging for other comorbidities. Symptoms, if present, are diverse, ranging from general and nonspecific to virtually pathognomonic. Compression of adjoining structures, such as the trachea, recurrent laryngeal nerve, or esophagus, may cause chest pain, neck mass, dysphagia, dysphonia, laryngeal spasm, Horner’s and superior vena cava syndrome. Myasthenia gravis is the most characteristic intercurrent phenomenon, observed in 30% of patients with thymoma. Other autoimmune or paraneoplastic syndromes may include red cell aplasia, hypogammaglobulinemia, endocrine disorders, cutaneous disorders and connective tissue disorders.
Due to infrequent occurrence of thymomas in childhood, and the rarity of studies focused on children, diagnosis, prognosis and treatment guidelines are remarkably challenging and not unequivocally established for pediatric patients [2].
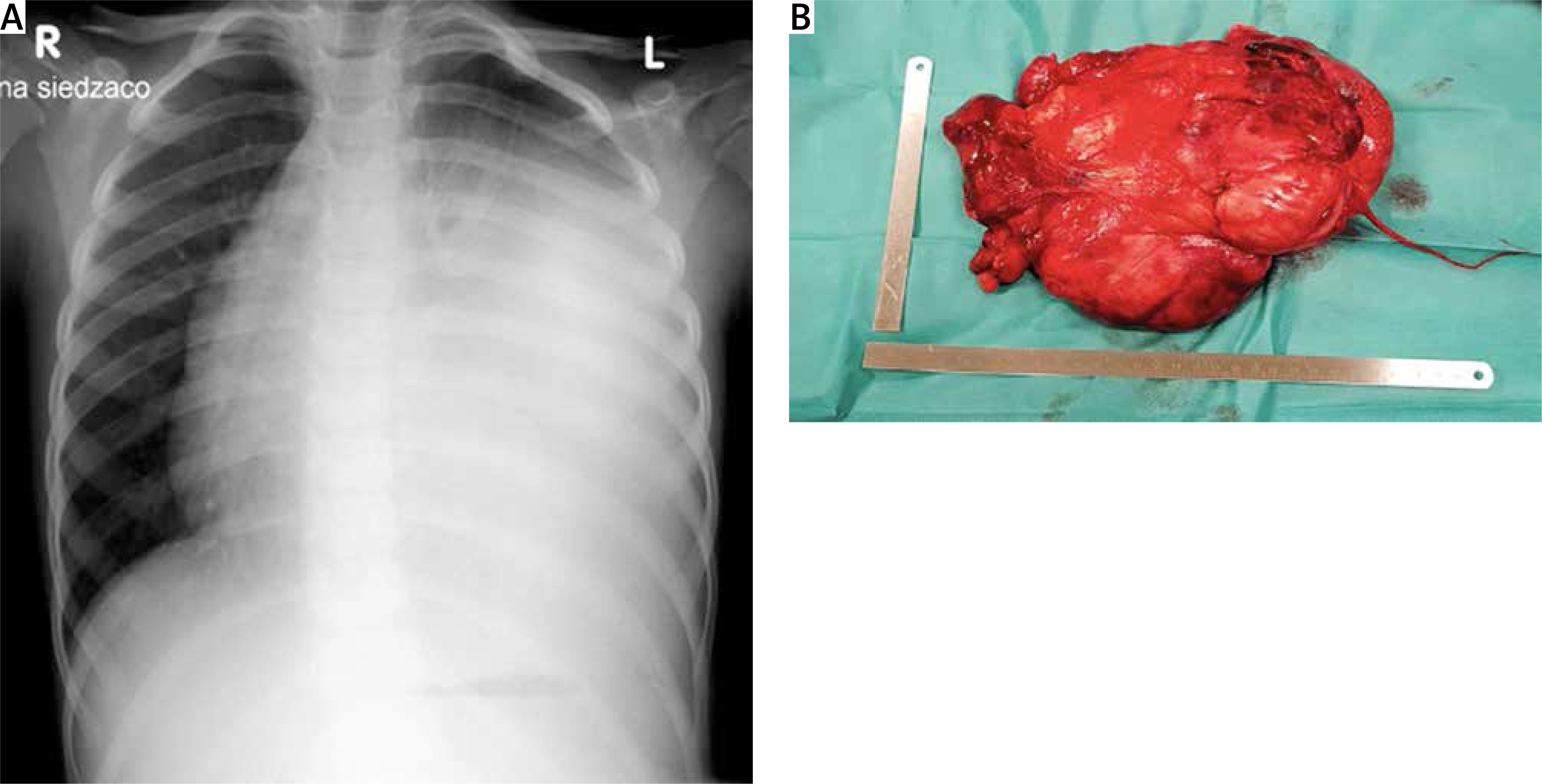
A 6-year-old boy (weight: 19 kg – 25th centile, height: 120 cm – 60th centile) was admitted to the hospital in 2018 with month-long night sweats, nonspecific conjunctival hyperemia and fatigue. The patient was observed with lymphadenopathy since he was 2 years old. Family history of hypertension and lymphoblastic leukemia was noted. Prior to admission, abdominal ultrasound was performed and enlarged, soft, mobile, nontender lymph nodes in the left parotid gland, along the left sternocleidomastoid muscle and in the left axilla, were revealed. Thoracic ultrasound showed a pathological mass that occupied the left side of the upper body. Chest X-ray detected consolidation in the middle and lower zone of the left lung, displacement of the left hilar region and pleural effusion (Figure 1). The patient underwent a median sternotomy followed by an extended cut along the left rib arc in order to perform total gross resection. During the surgery, the child was intubated with a simple endotracheal tube (size 5.5). The stage II tumor in Masaoka-Koga criteria with the left pleura was resected (Figure 1). Later histopathologic examination demonstrated two distinct patterns of the tumor: the predominant one was spindle cell thymoma with papillary or pseudopapillary features (type A thymoma according to the WHO classification); other areas were composed of micronodular thymoma with lymphoid hyperplasia. The procedure was finished with a chest tube inserted into the left pleural cavity, while the second one was reaching to the right pleural cavity and was placed under the sternum.
Figure 1
Posterior-anterior chest X-ray in preoperative period (A). Image of a 15 × 25 cm resected tumor mass (B)
The patient did not develop any complications during the operation and both chest tubes were removed on the 2nd postoperative day (POD). Post-surgery chest decubitus X-ray showed decreased density in the apex of the left lung and lack of vascular pattern, which suggested left-sided pneumothorax. Pleural effusion in the left pleural cavity manifested as opacity in the lower and middle fields of the left lung with streaky opacities above the fluid level suggesting atelectatic changes. Three hundred milliliters of fluid was collected with a 12F drainage catheter, which was placed into the left pleural cavity accessed from the 5th intercostal space. The catheter was removed the next day. The cardiomediastinal contour was normal. The child was discharged from the hospital on the 9th POD in good general health.
In children, most of the tumors encountered in the mediastinum are those of lymphatic or neurogenic origin and thymomas represent a minority of cases (< 1%) [2]. Diagnosis may be challenging due to the heterogeneity of thymic lesions, rarity of cases and lack of established and standardized guidelines for pediatric patients. Staging and grading in children patients are determined on the basis of the Masaoka-Koga classification (established based on tissue infiltration) (Table I) and WHO staging (based on cells’ microscopic appearance), which are both the same scales used with adult patients [3–5].
Table I
Masaoka-Koga criteria of staging
I.V. contrast-enhanced computed tomography (CT) remains the method of choice for diagnosing thymoma. Preoperative biopsy is not mandatory if the diagnosis of a thymic tumor is highly probable [2, 6]. Choice of treatment is based on the staging of the tumor and can include surgical resection, chemotherapy and radiotherapy [4, 6]. All patients with resectable lesions should undergo radical thymectomy as a first step of treatment [5, 6]. Oncological follow-up examinations should last up to 10–15 years and consist of radiological evaluation such as a thoracic CT scan in 3–4 months after surgery. Afterwards, according to Masaoka-Koga staging, a CT scan should be performed every year for 5 years, then every 2 years in completely resected stages I/II. Regarding stages III/IV, CT is recommended every 6 months for 2 years and subsequently once a year [6].
This case is noteworthy not only due to the presence of a thymoma in a child, but also due to its size. According to an analysis by Fukui et al. the median size of thymoma and thymic carcinoma were 4.8 and 5.7 cm respectively [7]. Another article states that most thymomas range from 5 to 10 cm in size, which makes the resected tumor mass (15 × 25 cm) exceedingly large, especially in a 6-year-old child [8].









