
Introduction
Nasopharyngeal cancer (NPC) is reported to be endemic in South China and Southeast Asia, particularly in Indonesia, accounting for 5.2% of all documented cancer cases [1]. Radiation is the primary treatment strategy for NPC, and when combined with chemotherapy, it helps reduce micrometastasis and the tumor’s susceptibility to radiation [2]. Despite radiation technology being a curative treatment of locally progressed NPC, the recurrence rate remains significant [3]. In Indonesia, the 2-year head and neck cancer recurrence rate reached 50%, with 47.69% of patients dying within 2 years after treatment [4].
Overall survival is the gold standard for measuring outcome status in many NPC studies. However, this is often challenging since OS analysis requires a large sample size and a longer monitoring period [5]. By analyzing recurrence as an indication of outcome status, Prentice’s criteria stated that 2- and 3-year progression-free survival (PFS) rates are valid as a substitute for OS [6].
Clinical prognostic factors based on existing tumor-node-metastasis (TNM) assessments are insufficient to stratify patients for the benefit of adjuvant chemotherapy, particularly in patients with complete and partial responses. Vascular endothelial growth factor (VEGF) and osteopontin (OPN) are two biomolecular markers that have been adequately studied for malignancy, including NPC. They are also linked to tumorigenesis capabilities such as tumor cell proliferation, angiogenesis, and the invasive nature of tumor and metastasis. Vascular endothelial growth factor expression was elevated in various solid tumors, including NPC. It was also linked to a poor prognosis due to the greater likelihood of tumor cells spreading to surrounding tissues [7–11]. Snitcovsky et al. [12] reported that OPN expression in NPC patients before therapy was considerably higher in cases with a more advanced stage based on tumor size (T) from TNM classification. Meanwhile, those with lower OPN expression had better survival and therapeutic outcomes. Despite a few studies suggesting a correlation between the two biomarkers and tumor progression, their participation in therapeutic outcome and survival was considered insufficient.
This study, which included a significant number of NPC patients from endemic countries such as Indonesia, was conducted to determine when the relationship of VEGF and OPN with 3-year PFS can potentially be a prognostic predictor. The administration of adjuvant chemotherapy has been shown to improve PFS in NPC. It is hypothesized that these biomarkers can be used to stratify patients who will benefit from post-radiotherapy adjuvant chemotherapy [13, 14]. Individuals with a low PFS may be candidates for neoadjuvant chemotherapy when these biomarkers can predict the PFS of NPC patients. Therefore, this study aims to identify a correlation between VEGF and OPN expression and 3-year PFS as a recurrence measure.
Material and methods
Population and data collection
The targeted population in this study comprised patients with locally advanced nasopharyngeal carcinoma treated in Cipto Mangunkusumo National General Hospital (RSCM) in the period 2015–2017. The location included the Oncology Clinic, medical record center, anatomical pathology laboratory, and radiology center of RSCM. Data were collected from April to December 2020 based on medical records and pathology specimens (paraffin block) obtained from patients with nasopharyngeal carcinoma between January 2015 and 2017. Before collecting data from included individuals, informed consent was obtained, and for the deceased, consent was gained from the rightful relatives. The following are the inclusion criteria:
patients aged above 18 years and not pregnant,
histopathology examination showed locally advanced nasopharyngeal carcinoma without metastasis,
chemoradiation with a platinum-based radiosensitizer was administered over 7 to 8 weeks, and the cumulative dose of cisplatin of 200 mg/m2,
eligible for neoadjuvant or adjuvant chemotherapy,
no history of anti-VEGF treatment,
complete and partial remission after chemoradiation therapy (objective response rate).
The exclusion criteria were incomplete medical record data, inadequate pathological specimens, and multiple malignancies. According to Irawan et al. [4], the sample size for investigating the 3-year PFS was 93.. Furthermore, the size which shows the relationship of VEGF and OPN expression with 3-year PFS was calculated referring to the same study [4, 15].
Z (type I error of 5%) and Z (type II error of 10%) were 1.96 and 1.28. The duration of the observation was 36 months. According to Irawan et al., the estimated 3-year PFS was 40%, and the hazard (λ) was 60%. Therefore, the necessary sample size was at least 152 for both groups. Table 1 shows the results of the subject number calculation.
Measurement of vascular endothelial growth factor and osteopontin expression
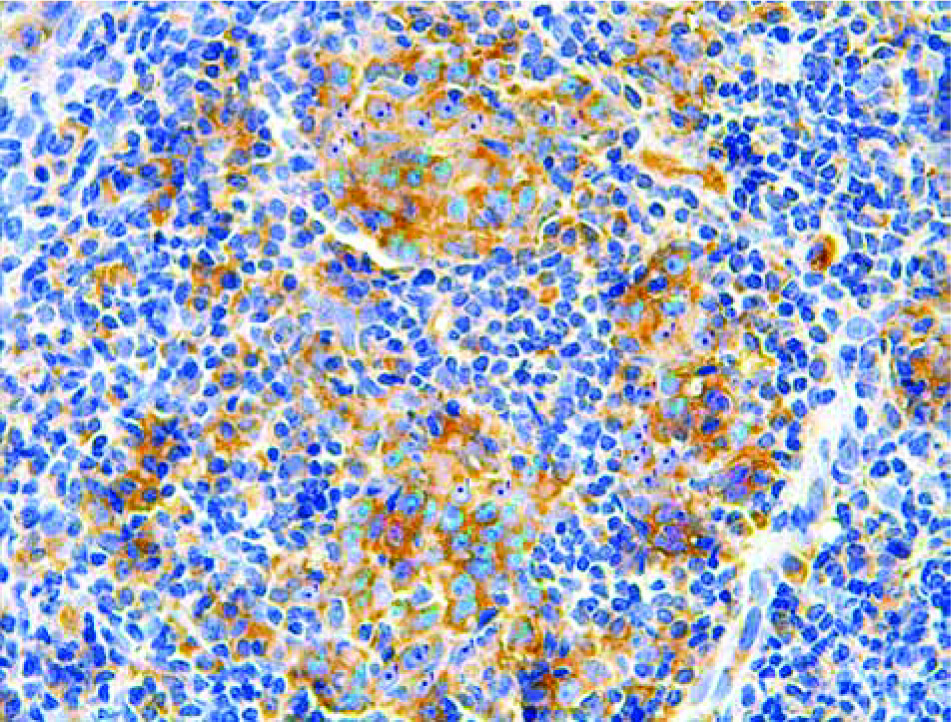
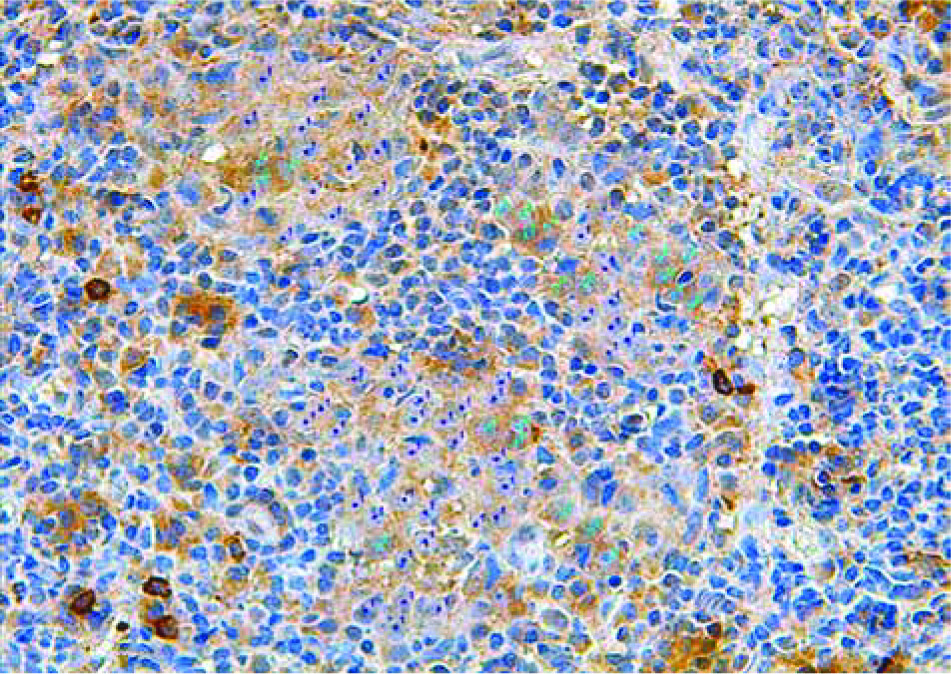
Histopathological slides of eligible samples were stained with hematoxylin-eosin for rechecking. Afterwards, immunohistochemical (IHC) staining for VEGF (Figure 1) measurement was performed with mouse VEGF (C-1: sc-7267 Santa Cruz monoclonal antibody with 1: 100 dilution). It is important to note that IHC staining for OPN (Figure 2) was performed with OPN AKm2A1 Santa Cruz monoclonal antibody (1 : 100 dilution). The observers were two anatomical pathologists blinded to the clinical data of each IHC slide. Using ImageJ 1.50i, the observers calculated the intensity of IHC staining with Allred criteria and the histoscore (h-score) semi-quantitative method. This method of IHC staining was previously conducted by Irawan et al. [4].
Data analysis
Data were analyzed with SPSS software version 20. The association of VEGF and OPN expression with 3-year PFS was presented using the Kaplan-Meier curve and log-rank test. The threshold of statistical significance (α value) was less than 0.05 (p < 0.05).
Ethical approval
Telephone calls or home visits were conducted in patients with previously unknown clinical outcomes. The FKUI-RSCM (Faculty of Medicine Universitas Indonesia-RSCM) Research Ethical Committee approved the study with the reference number KET.869/UN2.F1/ETIK/PPM.00.02/2020. The procedures were conducted according to the Declaration of Helsinki and complied with the ethical regulations. Finally, written informed consent was obtained from every subject.
Limitation of the study
This study was funded by research grant No. NKB-900/UN2.RST/HKP/05/00/2020 by PUTI Prosiding Universitas Indonesia. The authors are grateful to the parties that contributed to the results, including the medical and administrative staff of RSCM.
Although this study was the first retrospective cohort study evaluating the relationship of 3-year PFS of locally advanced NPC with VEGF and OPN expression, it was conducted at a national referral hospital in Indonesia. This study has heterogenous therapy regimens including cytostatic agents and radiation techniques, as well as uneven distribution of subjects in each group. There are particularly few individuals in the adjuvant chemotherapy group. However, there are currently no established cut-off values for measuring OPN and VEGF expression, resulting in variable clinical results from VEGF and OPN studies. Other than VEGF and OPN expression in the cancer mass, the serum levels of these biomarkers are additional prognostic factors that were not analyzed. This study only includes samples with a complete and partial response to the therapy (“responder”) evaluated using Response Evaluation Criteria in Solid Tumors. Further study on VEGF and OPN expression in subjects with progressive and stable disease could hold valuable information to complete our understanding of these biomarkers.
Results
Sample characteristics
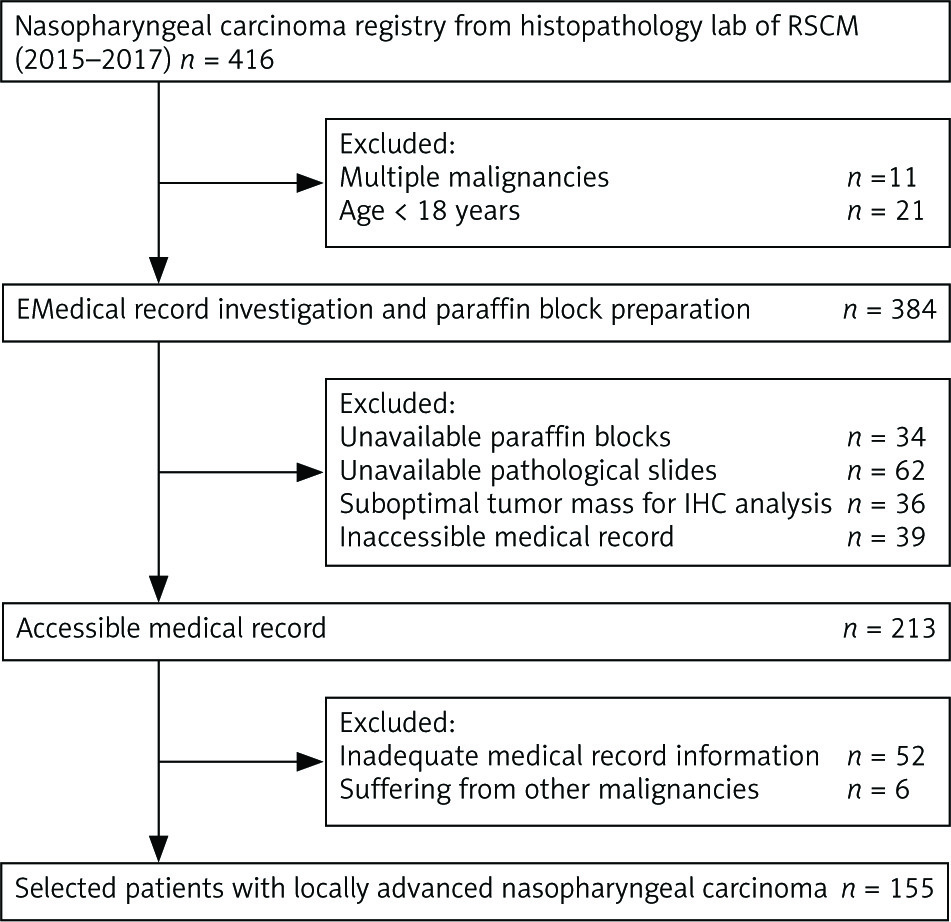
The targeted population included 416 patients registered in RSCM. However, some were excluded for various reasons related to the inclusion and exclusion criteria. Figure 3 shows the sample selection flowchart.
Fig. 3
Sample selection flowchart of the study
IHC – immunohistochemical, RSCM – Cipto Mangunkusumo National General Hospital
The selected samples were 155 patients, but 14 of them could not be contacted. Since events could not be observed in those 14 patients, the analysis was conducted based on the information until their last clinical visit. Loss-to-follow-up information was incorporated into the sensor. In general, the clinical characteristics of the patients are listed in Table 2.
Table 2
Clinical characteristics of study samples
Other clinical and pathological characteristics that potentially became confounding variables were analyzed using bivariate analysis (Table 3), followed by multivariate analysis (Table 4) for the data with p < 0.25, including age and body mass index (BMI). The change in hazard ratio was less than 10%; hence, age and BMI were not confounding variables when analyzing the relationship of VEGF and OPN expression with 3-year PFS in patients with locally advanced nasopharyngeal carcinoma, as well as undergoing platinum-based chemoradiation.
Table 3
Bivariate analysis of potential confounding variables and 3-year progression-free survival
Table 4
Multivariate analysis and change of adjusted hazard ratio for vascular endothelial growth factor and osteopontin expression
Association between vascular endothelial growth factor and osteopontin expression and 3-year progression-free survival
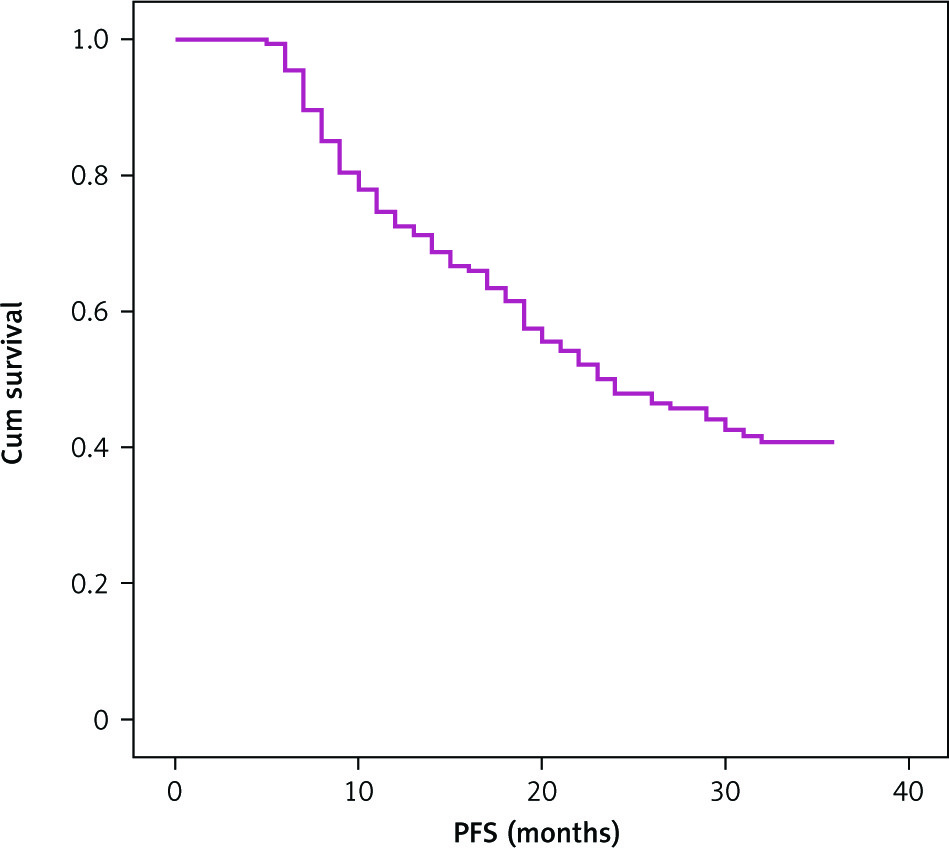
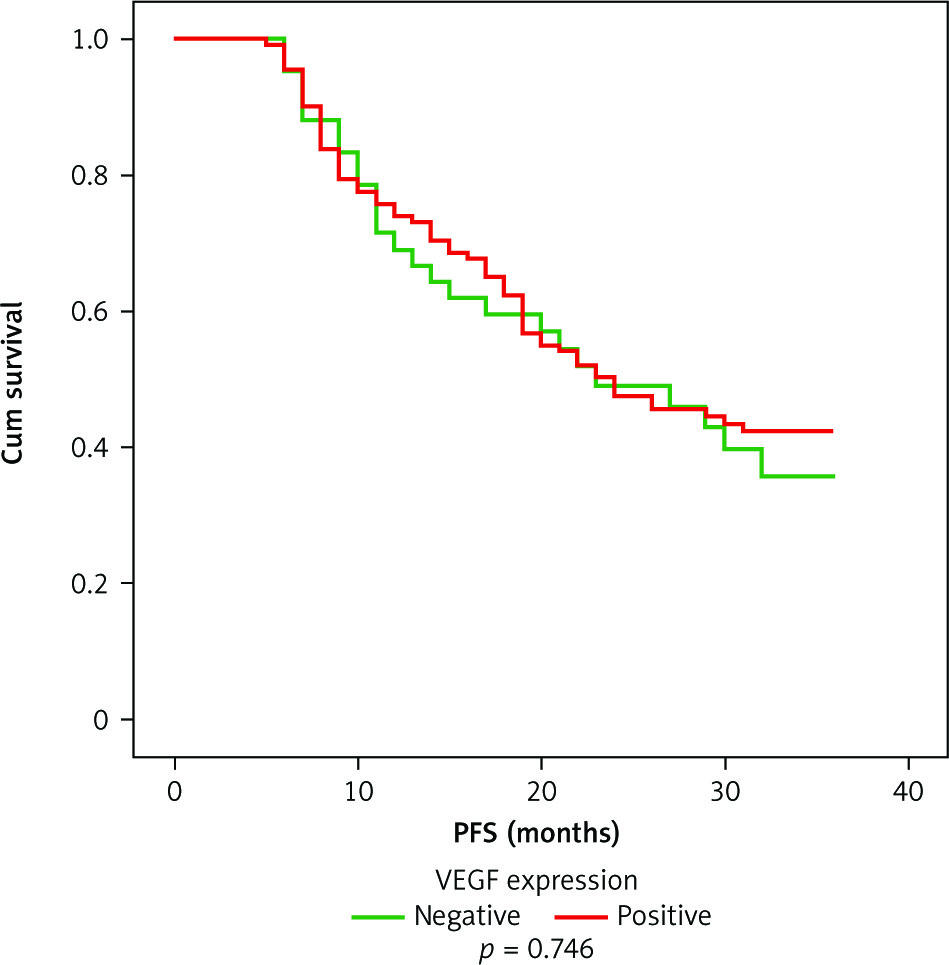
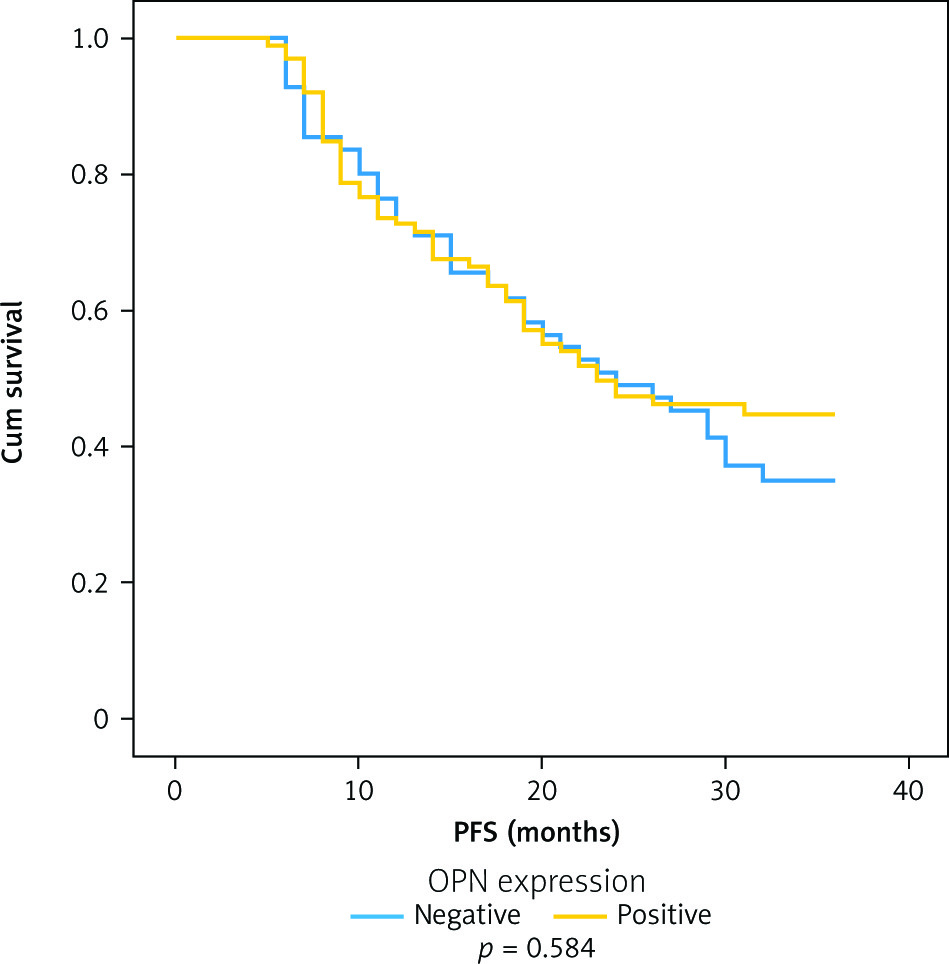
Figure 4 shows that the median 3-year PFS in patients with locally advanced NPC was 23 months. The 3-year PFS and OS were 39% and 49.5%, with standard errors (SE) of 4% and 5.6%, respectively. The proportion of positive and negative VEGF patients was 72.9% (113) and 63.8% (99). According to Figure 5, the Kaplan-Meier curve showed that the 3-year PFS rates of patients with positive and negative VEGF were 40% (SE of 5%) and 36% (SE of 8%), respectively, with a log-rank p-value of 0.746. Meanwhile, those with positive and negative OPN were 41% (SE of 6%) and 35% (SE of 7%), respectively, with a log-rank p-value of 0.584 (Figure 6).
Fig. 4
3-year progression-free survival in 155 patients with locally advanced nasopharyngeal cancer
PFS – progression-free survival
Subgroup analysis
A subgroup analysis was conducted for factors that might affect the 3-year PFS in patients with locally advanced NPC. These factors included stage of the disease, T category, nodal involvement category (N), type of therapy, and therapeutic response. The analysis results are shown in Figures 7 and 8 with VEGF and OPN expression, respectively.
Fig. 7
Subgroup analysis for vascular endothelial growth factor expression
VEGF expression: negative vs. positive
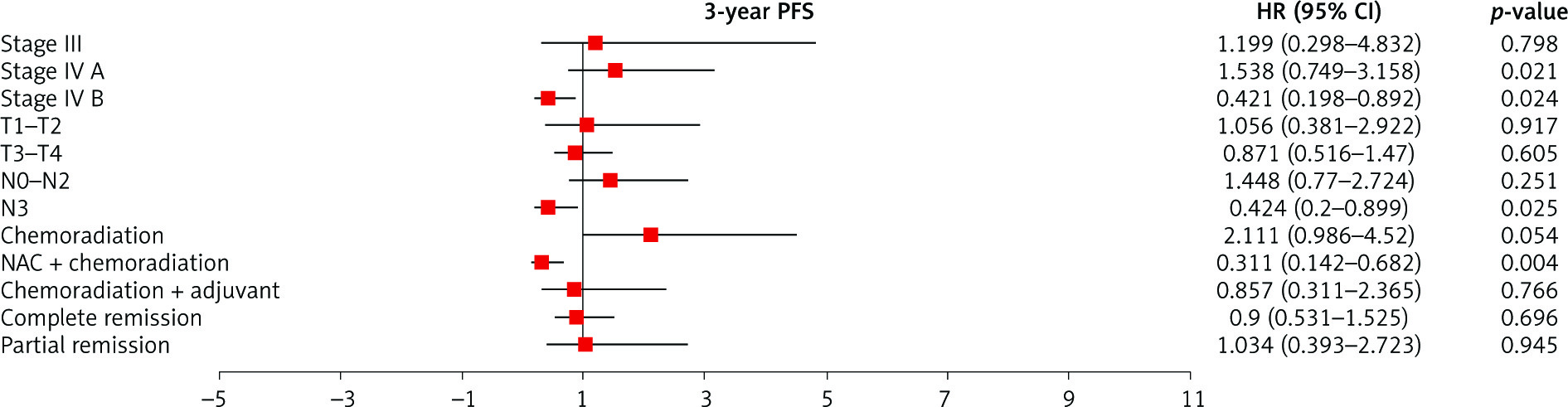
Fig. 8
Subgroup analysis for osteopontin expression
HR – hazard ratio, OPN – osteopontin, PFS – progression-free survival
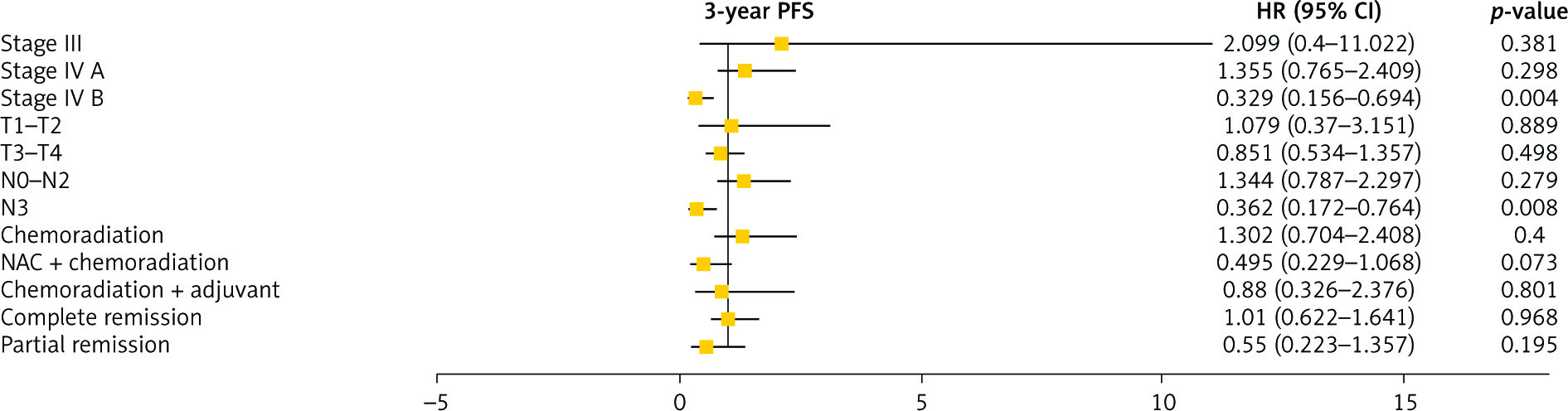
In patients with the N3 nodal involvement category, positive VEGF and OPN expression was significantly associated with improved 3-year PFS compared to those with negative VEGF and OPN expression. Furthermore, the log-rank values for VEGF and OPN were p = 0.025 and p = 0.008, respectively. A similar significant association was also discovered in the stage IVB group with log-rank values of p = 0.024 and p = 0.004 for VEGF and OPN, respectively. Sufferers undergoing neoadjuvant chemotherapy (NAC) followed by chemoradiation showed a significant association (p = 0.004) between positive VEGF expression and improved 3-year PFS compared to those with negative VEGF expression.
Discussion
This retrospective cohort study involved 155 patients with locally advanced NPC, most of whom were male (72.9%). This corresponded to the epidemiological profile of this disease, which is acknowledged to occur more often in males than females, with a ratio of 2–3 : 1 [16, 17]. Furthermore, the factors responsible for the gendered tendency are poorly understood. It might be associated with lifestyle and occupation, with males being more likely to be exposed to carcinogens, such as chemical compounds in cigarettes, ashes, chemical gases, formaldehyde, wood vapor, and burn residues in their working places [18–20].
The respondents’ mean age was 47 years, with 79.4% (123 patients) below 60 years. In low-prevalence areas, NPC incidence increases with age. Meanwhile, in high-prevalence areas, it rises significantly after 30 years and peaks at 40–59 years. This is due to the long latent period of Epstein-Barr virus (EBV) infection as one of the most predominant risk factors [21, 22]. The latent, asymptomatic period could be 20–25 years, and the malignant transformation involving oncogene activation and reduced tumor suppressor gene occurs thereafter [23].
Most of the respondents had T4, followed by T2, T3, and T1, consisting of 112, 26, 13, and 4 patients, respectively. The majority came with lymph-node involvement, and most of the cases were N2, followed by N3, N1, and the fewest N0, comprising 77, 47, 21, and 10 patients, respectively. Clinically, most patients (88.4%) had stage IV. This result is consistent with Meidani et al. [24], who stated that most of the subjects had stage IVA and IVB, representing the presence of delayed diagnosis and therapy. This could be due to the long asymptomatic period, nonspecific symptoms, and lack of awareness regarding the early symptoms of NPC. Fles et al. [25] found that the average delay of therapy was 6 months, attributable to environmental, cultural, religious, and socioeconomic factors.
It was reported that most patients (76.8%) had complete remission, while the rest had partial remission. This is in contrast to Dwijayanti et al. [26], who reported that the rates of complete remission, partial remission, and progressive disease of locally advanced NPC patients undergoing neoadjuvant chemotherapy followed by chemoradiation were 33.7%, 45.2%, and 21.2%, respectively. This is due to the different therapeutic schemes, including the adjuvant chemotherapy and radiation technique. It was observed that the patients experiencing complete remission were mostly treated with the most recent and well-established intensity-modulated radiation technique (IMRT). However, the lower proportion of patients in this study with partial remission occurred because only a few patients underwent systemic therapy as an addition to the primary treatment.
This study showed that the 3-year PFS in patients with locally advanced NPC was relatively low at 39% (SE 4%). Furthermore, half of them experienced cancer-related events within 23 months. Irawan et al. [4] also reported a similar result, the 2-year PFS in head and neck cancer being 50%. However, the PFS rate in this study was significantly lower than in another high-prevalence country, namely China, where the 5-year PFS in 332 NPC patients was 85.8% [27]. This might be related to the difference in therapeutic regimens, schemes, and radiation techniques involving those using 2D/3D techniques and IMRT. The intensity-modulated radiation technique was recommended to minimize the side effect of radiation to the surrounding tissues so that the optimal dose could attain the primary tumor location [28]. In this study, not all patients with T of N3 or T4 underwent neoadjuvant chemotherapy. Meanwhile, Peng et al. [29] and Liu et al. [30]. stated that stage T3 or N4 patients benefited from induction chemotherapy or neoadjuvant. This implies that systemic therapy is required to control the recurrence of PFS, specifically distant metastasis.
A more objective approach was used to detect VEGF and OPN expression. Various methods can be used to identify VEGF and OPN. Vascular endothelial growth factor can also be determined with the quantitative enzyme-linked immunosorbent assay (ELISA) method or the chemiluminescence enzyme-linked immunosorbent assay (CL-ELISA) in addition to the technique used in this study [31, 32]. Osteopontin, on the other hand, can be detected using a tissue microarray with a manual tissue arrayer or by measuring its plasma levels with an ELISA [33, 34]. Some studies have used a qualitative approach, interpreting VEGF and OPN expression as low and high. In contrast, others have only used immunoreactive scores, calculating the percentage and intensity of the stained cells. This study used a semi-quantitative approach, scoring the intensity and percentage of stained cells with an h-score. The method could represent the VEGF and OPN expression more objectively in samples [24]. The proportion of patients with positive VEGF and OPN was 72.9% (113 out of 155 patients) and 63.8% (99 out of 155 patients), respectively, according to previous studies. Krishna et al. [9] reported that high positive VEGF expression was discovered in 67% of cases. Meanwhile, Qin et al. [35] reported high positive OPN expression in 97% of nasopharyngeal aspirate specimens.
According to the Kaplan-Meier analysis, the expression levels of VEGF and OPN were not significantly associated with 3-year PFS in patients with locally advanced NPC. This is in contrast to Pan et al. [9], who stated that high VEGF expression was a worse prognostic factor for survival, disease-free survival, and locoregional control. Hou et al. [34] also reported that OPN expression was associated with high recurrence in bone, a high metastatic rate, and low survival. The difference between this result and those previous studies was due to variations in several aspects, including the clinical staging of NPC, clinical outcomes evaluated, the measurement method of VEGF and OPN expression, and therapy regimens. The samples only involve locally advanced NPC patients, and most have positive OPN and VEGF expression. Variability of these expression levels in early-stage NPC results in a different relationship with 3-year PFS. This study’s measurement of VEGF and OPN expression using the h-score is a more objective approach and could be one of the reasons for obtaining different results from others. Types of radiation techniques and cytostatic regimens also contribute to therapeutic outcomes and PFS. The majority, 77 patients (49.7%), received chemoradiation therapy, while the remaining 54 (34.8%) were administered the combination of chemoradiation and neoadjuvant chemotherapy, and only 24 (15.5%) were treated with adjuvant therapy. Cisplatin, fluorouracil (5FU), or carboplatin was used in chemotherapy, while cisplatin paclitaxel was employed in induction. These chemotherapy dosages are calculated based on patients’ body surface area. The dose of cisplatin used was 100 mg/m2 and that of fluorouracil (5FU) was 1000 mg/m2. The majority of patients (55.5%) underwent chemoradiation with IMRT, but in the remaining 33 (21.3%) and 36 (23.2%), 3D and 2D technique, respectively, was used. A meta-analysis showed that IMRT resulted in significantly better overall survival, local recurrence-free survival, and PFS compared with 3D/2D technique [36]. Therefore, it is necessary to conduct a further study involving early-stage NPC, a more homogeneous group of therapy regimens, and a more objective and standardized measurement method of VEGF and OPN expression.
The subgroup analyses showed that positive VEGF and OPN expression was significantly associated with improved 3-year PFS compared with those with negative expression in subjects with T of N3 and clinical staging of IVB. This is due to the therapy regimen administered in each group, in which those with more advanced stages were treated more aggressively. Furthermore, positive VEGF expression also had a significant relationship with more favorable 3-year PFS in a subgroup of those undergoing neoadjuvant chemotherapy followed by chemoradiation. These findings were not significantly different from other studies, showing that induction or neoadjuvant chemotherapy could improve disease-free survival [37–39]. A meta-analysis by Chen et al. [37] also proved that neoadjuvant chemotherapy improved distant-metastasis survival [39].
Some patients, such as those with a tumor stage of T4, benefited from neoadjuvant chemotherapy followed by chemoradiation due to the reduced risk of distant metastasis. This is similar to Peng et al. [29], who stated that tumor response to neoadjuvant chemotherapy could be a strong prognostic predictor and help to develop an individual therapeutic strategy for patients with locally advanced NPC. In addition to the standard therapy applied in Indonesia, and the availability of cytostatic agents for NPC, the low PFS in the country could also be attributable to the limited medical access as some cytostatic regimens are not covered by the national health insurance.
The other subgroup benefiting from neoadjuvant chemotherapy was those with the nodal status of N3. Liu et al. [30] reported that in 412 patients, there was an improvement in clinical staging from N2–N3 to N0–N1 after neoadjuvant chemotherapy. Furthermore, the 3-year PFS was significantly better in those receiving this therapy [34]. Evaluation was performed after a therapeutic scheme and is essential to determine the next treatment. However, some aspects that need to be considered include cost, diagnostic modalities, and the hospital queue management system related to national health insurance.
Based on the analysis, neoadjuvant chemotherapy could predict the 3-year PFS in those with positive VEGF expression compared with the scheme without this treatment (log-rank p = 0.036). This could increase the potential for targeted therapy in NPC patients with PFS as the clinical outcome parameter. The reason adjuvant chemotherapy failed to predict PFS might be due to the limited number of subjects.
To determine the effect of VEGF and OPN expression in patients with partial remission, a Kaplan-Meier analysis was conducted on 28 subjects after excluding those without adjuvant chemotherapy. The results were p = 0.815 and p = 0.155 for VEGF and OPN expression, respectively. However, the curve trend showed that positive VEGF expression was less steep in the 20th month than the negative counterpart. The less steep curve was discovered in the chemoradiation sub-group in the partial remission groups. This leads to the consideration of more suitable therapy regimens.
Conclusions
This study provided inconclusive evidence for a relationship between VEGF and OPN expression and 3-year PFS. Employing biomolecular markers in conjunction with PFS to stratify individuals with NPC might not be as straightforward as one might assume. However, the results from the subgroup analysis showed significantly improved 3-year PFS in N3, stage IVB, and subjects receiving neoadjuvant chemotherapy. This suggests that further research utilizing these two biomarkers in more controlled subjects’ environments will yield more clarity on patient survival. Furthermore, other studies investigated additional biomarkers such as CD3+ tumor-infiltrating lymphocytes and peripheral blood hemoglobin, EBV DNA copy number, ratios of albumin-to-alkaline phosphatase ratio, neutrophils, or platelets-to-lymphocytes, and Ki-67 [40, 41].
In addition to VEGF and OPN having essential utility as prognostic biomarkers in patients with NPC, an alternative treatment strategy for the disease was also offered. Since VEGF is abundantly expressed in nasopharyngeal cancer, inhibiting its binding may be a viable treatment. Alternative treatment for NPC includes drugs such as bevacizumab, targeted at the anti-VEGF antibody. On the other hand, OPN is overexpressed in many cancers, and such expression contributes to metastasis, progression, and drug resistance. It appears encouraging that there is a way to increase sensitivity to chemotherapeutics by inhibiting the generation of OPN through tumor cells or blocking the signaling cascades it induces. Research involving both serum biomarker concentrations and other dependent factors deepens the comprehension of their potential as prognostic prediction tools and therapeutic approaches.






