
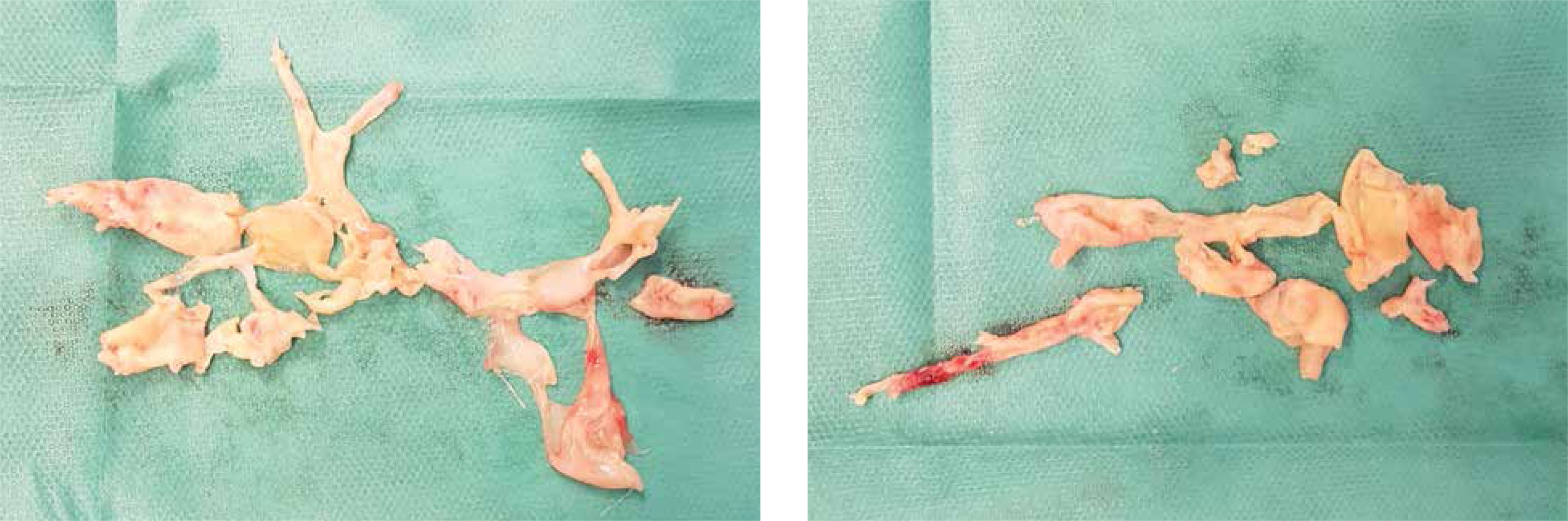
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare disease resulting from stenosis or obstruction of the pulmonary arteries due to organized thrombus with disruption of blood flow and derivative microvascular remodelling in 4% of survivors of acute pulmonary embolism (PE). Computed tomography (CT) angiography and conventional pulmonary angiography remain the gold standard to confirm the presence of fibrotic thromboembolic lesions in pulmonary arteries [1, 2]. Pulmonary endarterectomy (PEA) remains the treatment of choice for CTEPH, but in recent years, there has been significant progress in the development of alternate treatments for patients deemed non-operable such as balloon pulmonary angioplasty (BPA) or targeted drug therapy. Patient eligibility for PEA or BPA requires multidisciplinary evaluation at a specialized centre [1–4]. However, interpretation difficulties exist for CT imaging, especially at the level of segmental and subsegmental arteries. This is crucial in deeming eligibility for surgery versus percutaneous intervention. Here, we present a case of a 69-year-old man admitted with a high likelihood of CTEPH. The patient did not have significant comorbidities and reported gradual deterioration of exercise tolerance and exertional dyspnoea (World Health Organization functional class II) since having an acute pulmonary embolism episode in 2019, despite receiving long-term warfarin anticoagulant therapy. Echocardiography performed 6 months after the incident revealed signs of right ventricular dysfunction with high suspicion of pulmonary hypertension (tricuspid regurgitation pressure gradient (TRPG) 76 mm Hg, right ventricular systolic pressure (RVSP) 81 mm Hg, tricuspid annular plane systolic excursion (TAPSE) 17, with preserved left ventricle ejection fraction of 60%). Pulmonary single photon emission computed tomography (SPECT) performed using albumin macroaggregates labelled with radioactive technetium showed multiple bilateral, diffuse segmental perfusion defects typical of CTEPH. The patient underwent right heart catheterization (RHC) using the transjugular approach, which confirmed elevated mean pulmonary artery pressure (mPAP – 40 mm Hg), normal right arterial pressure (2 mm Hg) and pulmonary wedge pressure (4 mm Hg), with a calculated pulmonary vascular resistance (PVR) of 7.55 Wood units. Rotational pulmonary angiography (with 50 ml of contrast medium administered over 5 s of continuous infusion; 6F pigtail catheter) was performed simultaneously and showed lesions typical of CTEPH (ring-like stenosis, pouches, intravascular webs, subtotal occlusions) in the segmental and sub-segmental arteries of both lungs. Due to the complexity of the anatomy of the pulmonary arteries in patients with CTEPH (Figures 1 A, C), we performed three-dimensional rotational reconstruction with post-processing (Figures 1 B, D) to achieve optimal visualization in the characterization of the lesions. According to current guidelines, to determine operability (PEA), the patient had a consultation with an experienced cardiac surgeon and was qualified for PEA. Thus, the patient underwent uneventful PEA with marked improvement of hemodynamic parameters (mPAP 25 mm Hg, PVR 3.5 Wood units) (Figure 2).
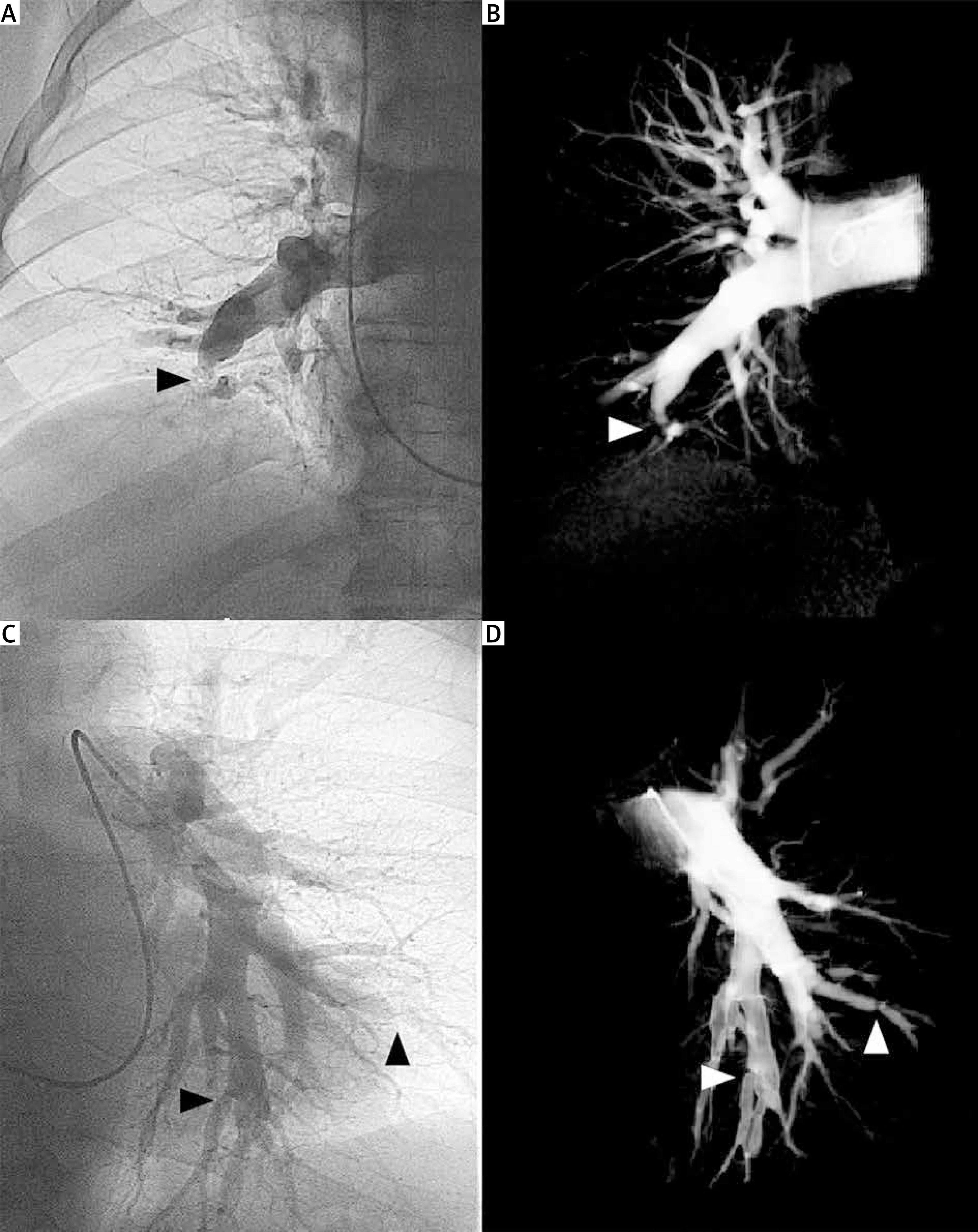
Figure 1
A – Right pulmonary artery angiography, AP-view; lower lobe pulmonary artery occlusion – pouch lesion (arrow). B – Three-dimensional rotational angiography reconstruction of right pulmonary artery, AP-view; lower lobe pulmonary artery occlusion – pouch (arrow). C – Left pulmonary artery angiography, AP-view; ring-like stenosis (arrow). D – Three-dimensional rotational angiography reconstruction of left pulmonary artery, AP-view; ring-like stenosis (arrow)
In summary, three-dimensional rotational angiography reconstruction can be a reasonable tool in the diagnostic work-up of CTEPH and for planning interventional or surgical treatment. Detailed reconstruction of the pulmonary arteries allows for the selection of appropriate balloon catheters that are even appropriate for distally located lesions. It can also provide additional information for PEA. Nevertheless, this strategy needs further assessment in a larger group of CTEPH patients.







