








Introduction
Percutaneous cerebral angiography is a standard approach used when diagnosing cerebrovascular diseases [1–3]. While the trans-femoral approach (TFA) is commonly used in a wide array of vascular interventional procedures [4–7], the trans-radial approach (TRA) has been adopted in place of the TFA in the cardiology field given that it results in lower rates of vascular complications and reduced bleeding, thereby improving patient safety outcomes and overall satisfaction [8–10]. The benefits associated with this approach have attracted interest in the use of the TRA when conducting cerebrovascular interventions [11].
Despite growing recognition of the advantages of the TRA, its adoption by neurointerventional specialists has been relatively limited to date, and the TFA dominates current training for these specialists such that there may be some reluctance to transition to the TRA even though it can be adopted without any change in the learning curve [11]. Several recent meta-analyses have been performed comparing the clinical efficacy of the TRA and TFA approaches in the context of cardiological interventions [10, 12], highlighting the need for a similar meta-analysis exploring the clinical efficacy of TRA cerebral angiography based on published randomized controlled trial (RCT) results [13–18].
Aim
This meta-analysis was thus designed to conduct a detailed comparison of the relative safety and efficacy of the TRA and TFA in the context of cerebral angiography.
Material and methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) statement [19] was used to guide the design of this meta-analysis, which was registered at INPLASY.COM (INPLASY202290021).
Study selection
Relevant studies published as of August 2022 in the PubMed, Embase, and Wanfang databases were identified using the following search strategy: (((transradial) AND (transfemoral)) AND (cerebral)) AND (angiography).
Eligible studies were those meeting the following criteria:
(a) Types of studies: RCTs;
(b) Patients: individuals requiring cerebral angiography;
(c) Types of interventions: TRA vs. TFA cerebral angiography;
(d) Languages: no limitations.
Study types that were excluded from this analysis were:
Data extraction
Relevant data were independently extracted from included studies by two researchers (WJZ and XJ), with inconsistencies being resolved through discussion with a third researcher (PHL). Extracted baseline data included first author, year of publication, country, patient numbers, age, gender ratio, history of smoking, body mass index (BMI), diabetes, hypertension, coronary heart disease, and hyperlipidemia. Extracted operative data included successful puncture rates, puncture time, successful cerebral angiography rates, operative duration, fluoroscopic duration, complication rates, and duration of postoperative recovery.
Quality assessment
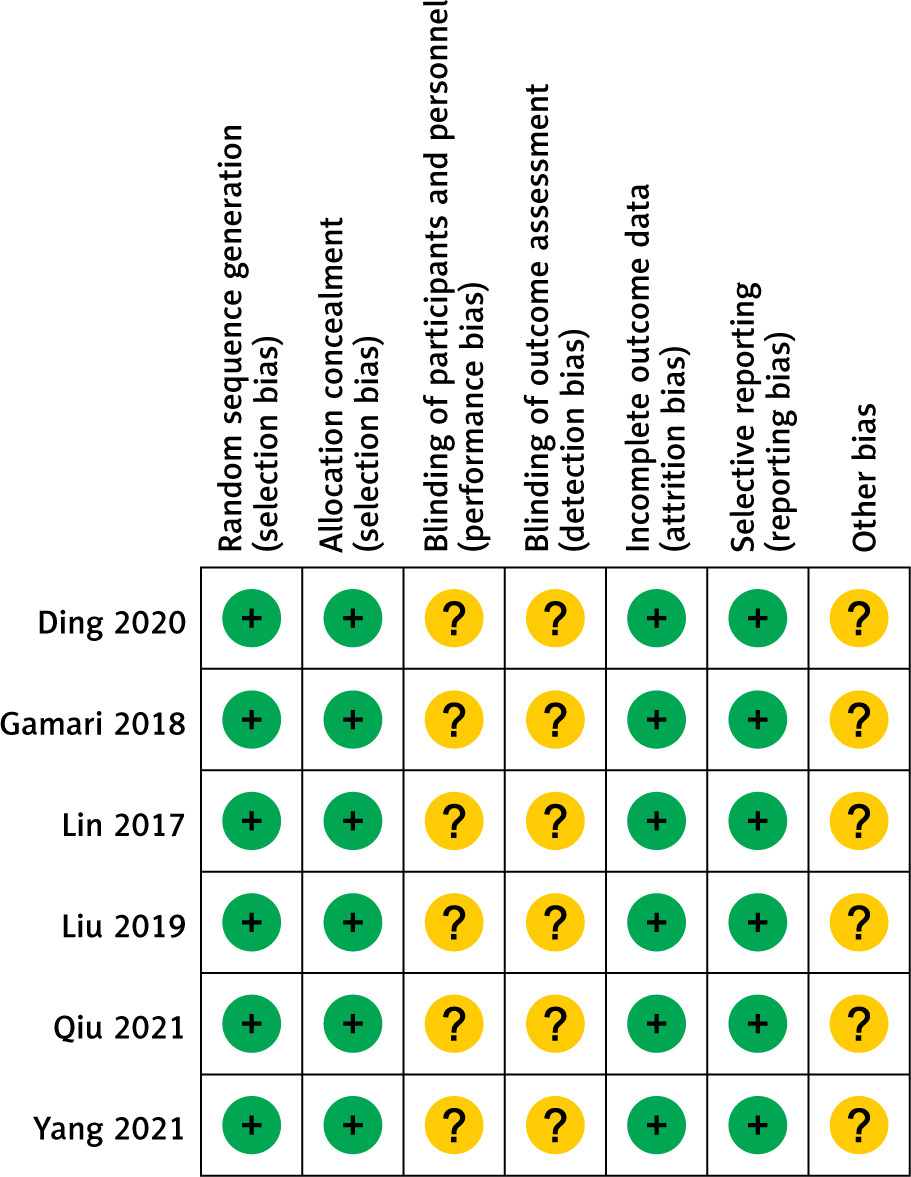
The risk of bias for included RCTs was examined using the Cochrane Collaboration tool, which was used to assign a high, low, or unclear risk of bias to each of the following forms of bias: selection, performance, detection, attrition, reporting, and other [20].
Study endpoints
Successful cerebral angiography rates were the primary endpoint for this meta-analysis. Secondary endpoints included successful puncture rates, puncture duration, operative duration, fluoroscopic duration, complication rates, and duration of postoperative recovery.
Successful cerebral angiography was defined by a single operator having successfully completed bilateral common carotid and vertebral angiography scans without the need to cross over to an additional access site [16]. Puncture time was the interval between initial puncture and successful introducer sheath placement [21]. Operative duration was the interval from arterial puncture to final closure [21]. Fluoroscopic duration was measured as a surrogate readout for radiation exposure during angiographic analysis [21].
Statistical analysis
RevMan v5.3 was used to pool all data. Dichotomous variables were analyzed using pooled odds ratios (ORs) and 95% confidence intervals (CIs), whereas mean difference (MD) values and 95% CIs were employed for analyses of continuous data. χ2 and I2 analyses were used to test for heterogeneity, and significant heterogeneity was defined by an I2 > 50%, random-effects and fixed-effects models being used in the presence and absence, respectively, of significant heterogeneity. A “leave-one-out” approach was utilized to perform sensitivity analyses exploring sources of heterogeneity. Egger’s test was performed using Stata v12.0 to detect publication bias, with p < 0.05 as the threshold for significant bias.
Results
Study inclusion
The study selection process is outlined in Figure 1. Ultimately, this meta-analysis incorporated 6 RCTs (Table I). These studies, all of which were conducted in China, included 542 and 539 patients who underwent TRA and TFA cerebral angiography, respectively (Table II).
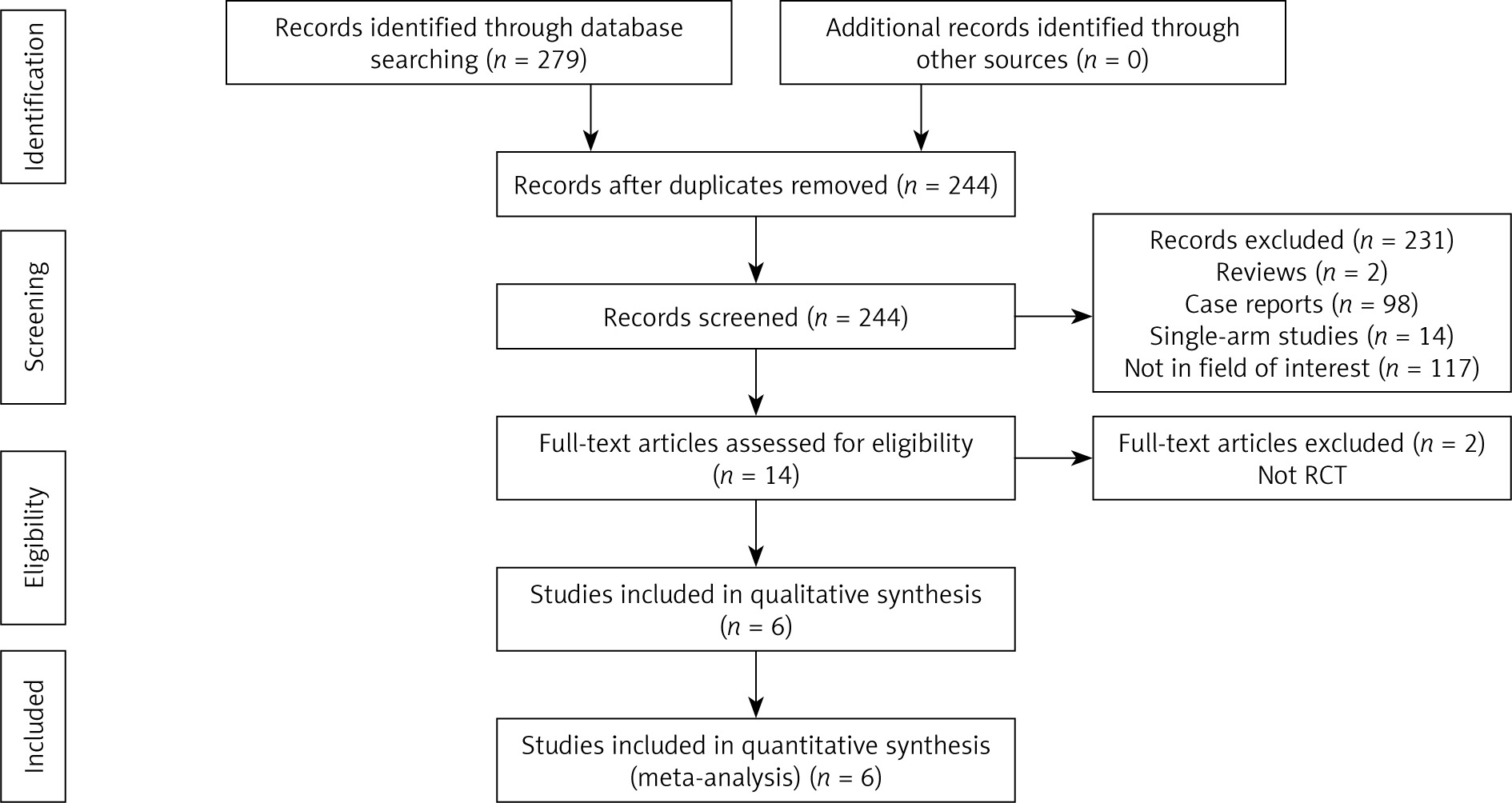
Table I
Baseline data of included studies
| No. | First author | Year | Countries | Study design |
|---|---|---|---|---|
| 1 | Ding [13] | 2020 | China | Randomized controlled trial |
| 2 | Gamari [14] | 2018 | China | Randomized controlled trial |
| 3 | Lin [15] | 2017 | China | Randomized controlled trial |
| 4 | Liu [16] | 2019 | China | Randomized controlled trial |
| 5 | Qiu [17] | 2021 | China | Randomized controlled trial |
| 6 | Yang [18] | 2021 | China | Randomized controlled trial |
Table II
Baseline data of patients
| Authors [ref.] | Groups | Number of patients | Male/female | Age [years] | BMI | Smoking | Hypertension | Diabetes | Hyperlipidemia | CHD |
|---|---|---|---|---|---|---|---|---|---|---|
| Ding [13] | TRA | 175 | 93/82 | 55.4 | Not given | Not given | Not given | Not given | Not given | Not given |
| TFA | 175 | 92/83 | 55.3 | Not given | Not given | Not given | Not given | Not given | Not given | |
| Gamari [14] | TRA | 100 | 52/48 | 55.2 | Not given | Not given | Not given | Not given | Not given | Not given |
| TFA | 100 | 54/46 | 55.4 | Not given | Not given | Not given | Not given | Not given | Not given | |
| Lin [15] | TRA | 152 | 86/66 | 62.5 | Not given | Not given | 105 | 37 | Not given | Not given |
| TFA | 148 | 79/69 | 59.7 | Not given | Not given | 107 | 32 | Not given | Not given | |
| Liu [16] | TRA | 50 | 41/9 | 68 | 24.2 | 28 | 36 | 12 | 23 | 11 |
| TFA | 51 | 40/11 | 67 | 24.4 | 28 | 40 | 14 | 14 | 8 | |
| Qiu [17] | TRA | 25 | 15/10 | 54.3 | 23.3 | Not given | Not given | Not given | Not given | Not given |
| TFA | 25 | 14/11 | 54.6 | 24.6 | Not given | Not given | Not given | Not given | Not given | |
| Yang [18] | TRA | 40 | Not given | 55.6 | 24.2 | Not given | Not given | Not given | Not given | Not given |
| TFA | 40 | Not given | 56.1 | 24.3 | Not given | Not given | Not given | Not given | Not given |
Risk of bias analyses revealed that none of these studies provided details regarding participant, personnel, or outcome assessment blinding, and all studies exhibited an unclear risk of other forms of bias (Figure 2).
Successful puncture rates
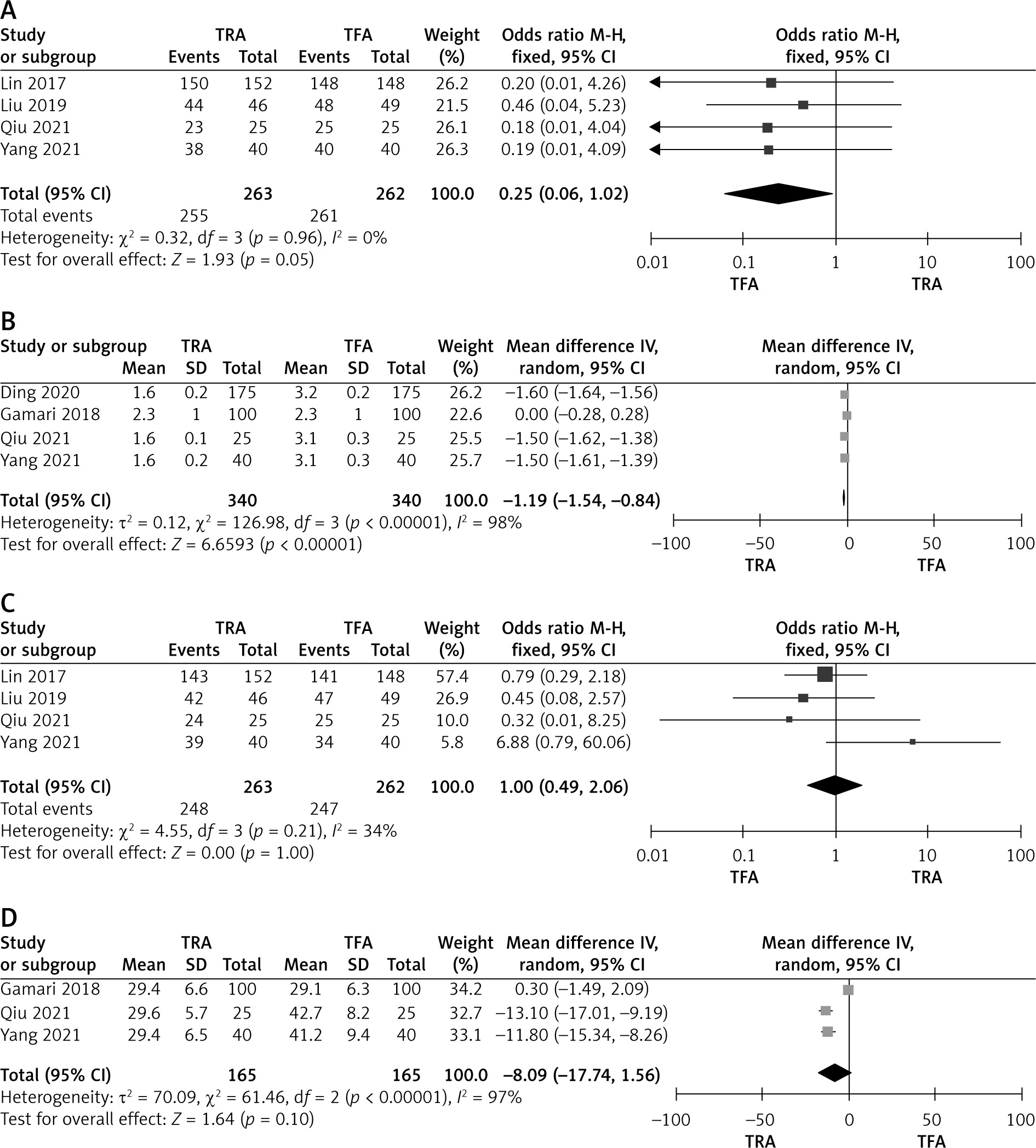
In total, successful puncture rates were extracted from 4 studies enrolling 263 and 262 patients who underwent TRA and TFA cerebral angiography, respectively [15–18]. Similar pooled successful puncture rates were observed in both the TRA and TFA groups (97.0% vs. 99.6%; OR = 0.25, p = 0.05, Figure 3 A). While no significant heterogeneity was observed for this endpoint (I2 = 0%), Egger’s test revealed a significant risk of publication bias (p = 0.0001).
Puncture time
Data pertaining to puncture time were successfully extracted from four studies enrolling 340 and 340 patients who underwent TRA and TFA cerebral angiography, respectively [13, 14, 17, 18]. The puncture time in the TRA group was significantly shorter than that in the TFA group (MD = –1.19; p < 0.00001, Figure 3 B). While significant heterogeneity was detected for this endpoint (I2 = 98%), sensitivity analyses failed to reveal the source of such heterogeneity, and no significant publication bias was detected (p = 0.487).
Successful cerebral angiography
In total, four studies enrolling 263 and 262 total patients who underwent TRA and TFA cerebral angiography, respectively, provided data regarding successful cerebral angiography rates [15–18]. Pooled successful cerebral angiography rates were similar in the TRA and TFA groups (94.3% vs. 94.3%; OR = 1.00, p = 1.00, Figure 3 C). This endpoint was not subject to significant heterogeneity (I2 = 34%), nor was any publication bias detected (p = 0.815).
Operative duration
Data pertaining to operative duration were successfully extracted from three studies enrolling 165 and 165 patients who underwent TRA and TFA cerebral angiography, respectively [14, 17, 18]. Pooled operative duration was similar in both the TRA and TFA groups (MD = –8.09; p = 0.10, Figure 3 D), although significant heterogeneity was detected for this endpoint (I2 = 97%). Sensitivity analysis identified the study conducted by Gamari et al. [14] as the source of this heterogeneity. There was no evidence of publication bias for this endpoint (p = 0.184).
Fluoroscopic duration
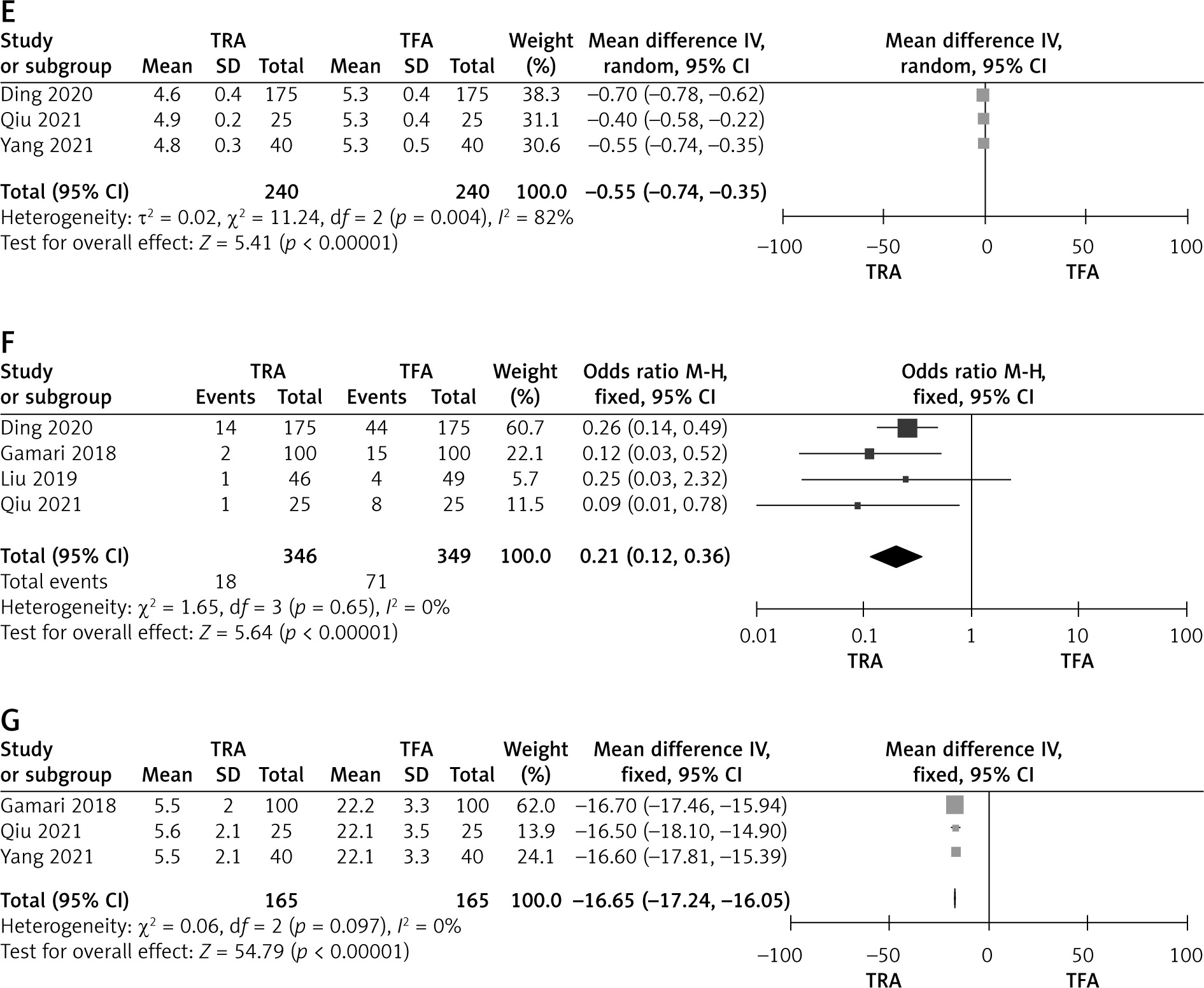
Data pertaining to fluoroscopic duration were successfully extracted from three studies enrolling 240 and 240 patients who underwent TRA and TFA cerebral angiography, respectively [13, 17, 18]. Relative to individuals who underwent TFA procedures, those who underwent TRA procedures exhibited a significantly reduced fluoroscopic duration (MD = –0.55; p < 0.00001, Figure 3 E). However, this endpoint was subject to significant heterogeneity (I2 = 82%), and sensitivity analyses identified the study conducted by Ding [13] as the source of this heterogeneity. There was no evidence of publication bias for this endpoint (p = 0.06).
Complication rates
Overall complication rates were extracted from four of the included RCTs enrolling 346 and 349 patients who underwent TRA and TFA cerebral angiography, respectively [13, 14, 16, 17]. Complication rates were significantly lower for individuals who underwent TRA procedures relative to those who underwent TFA procedures (5.2% vs. 20.3%; OR = 0.21, p < 0.00001, Figure 3 F). No significant heterogeneity was detected (I2 = 0%). There was no evidence of publication bias for this endpoint (p = 0.089).
Complication rates are provided in further detail in Table III. Significantly lower pooled hematoma (2.0% vs. 7.8%; OR = 0.27, p < 0.0001) and pseudoaneurysm rates (0.0% vs. 4.2%; OR = 0.17, p = 0.04) were observed in the TRA group relative to the TFA group, whereas similar pooled artery spasm rates were evident in both groups (0.6% vs. 3.6%; OR = 0.28, p = 0.11). No significant heterogeneity was observed for any of these endpoints (Table III).
Duration of postoperative recovery
The duration of postoperative recovery was reported in three studies enrolling 165 and 165 patients who underwent TRA or TFA cerebral angiography procedures, respectively [13, 17, 18]. Relative to individuals in the TFA group, those in the TRA group exhibited a significantly reduced duration of postoperative recovery (MD = –16.65; p < 0.00001, Figure 3 G). While no significant heterogeneity was observed for this endpoint (I2 = 0%), Egger’s test identified a significant risk of publication bias (p = 0.018).
Discussion
This meta-analysis was conducted to examine the relative safety of cerebral angiography procedures conducted via trans-radial and trans-femoral approaches. An initial comparison of puncture-related outcomes revealed similar rates of successful puncture (≥ 97%) in both groups, although the TRA entailed a significantly shorter puncture time relative to the TFA. Relative to femoral arteries, radial arteries can be more readily localized owing to the superficial access area for these venous structures [17].
Successful cerebral angiography rates were similar in both groups in this meta-analysis, consistent with the non-inferiority of the TRA relative to the TFA when conducting cerebral angiography procedures. In individuals with complex aortic arch anatomy such as individuals with bovine or type III arches, angiographic procedures are often longer and entail a higher risk of embolic events with the potential to cause neurological damage [22]. One retrospective analysis of 535 individuals with bovine or type III arches found the TRA to be associated with significantly higher successful catheterization rates in the right common carotid artery, right subclavian artery, and left vertebral artery relative to the TFA [21]. The TRA has also been reported to offer advantages with respect to carotid stent placement in patients with bovine arch [23], with a reported 100% procedural success rate in 16 individuals with bovine or type III aortic arches undergoing TRA-based carotid stenting having been reported by Dahm et al. [24].
Pooled operative duration values were comparable in the TRA and TFA groups in this study, whereas the TRA group exhibited a significantly shorter pooled fluoroscopic duration. This inconsistency is primarily attributable to the fact that these two endpoints were extracted from different RCTs. TRA procedures were shorter in individuals with unfavorable arch anatomy, enabling the use of less contrast and necessitating fewer procedures as compared to TFA procedures [21]. However, operative duration may be impacted by both operator experience and patient comorbidities including hypertension, heart disease, diabetes, and hyperlipidemia. Both of these endpoints were also subject to significant heterogeneity, indicating that these results were not stable and that additional high-quality RCTs will be essential to fully resolve the relative advantages of TRA and TFA cerebral angiography.
The results of this meta-analysis highlight the fact that the TRA is associated with lower complication rates than the TFA. As the radial artery access point is not adjacent to major blood vessels of nerves, this contributes to low rates of access site complications [21]. In the TRA group in this meta-analysis, pooled pseudoaneurysm and artery spasm rates were very low (< 1%) in the TRA group. When analyzing complications associated with 46 TRA cerebral angiography procedures performed by trainees, Liu et al. [16] observed an overall complication rate of just 1% and a hematoma rate of 0%.
Limb immobilization is an important factor that contributes to the prolonged postoperative recovery of individuals who undergo TFA relative to those who undergo TRA, highlighting the benefits of shifting the selected operative approach [21]. This prior finding was consistent with the results of the present meta-analysis, and this endpoint exhibited low levels of heterogeneity, suggesting that these results were stable.
There are certain limitations to this meta-analysis. For one, while only RCTs were eligible for inclusion in these analyses, the included RCTs all failed to offer any details regarding participant, personnel, or outcome assessment blinding, potentially contributing to bias affecting these results. In addition, only pooled successful cerebral angiography rates were compared for the TRA and TFA groups, whereas successful catheterization rates for the supra-aortic and branch vessels were not successfully extracted from the included studies, thus limiting the level of detail provided by these meta-analysis results. Third, subgroup analyses were not conducted for individuals with bovine or type III aortic arches, as only one of the included RCTs offered data for these patient subgroups [16]. Lastly, all included RCTs were conducted in China, highlighting a need for additional research focused on studies conducted throughout the world in order to ensure that these results can be generalized to other populations.