
Summary
Transcatheter aortic valve implantation (TAVI) in patients who have undergone mitral valve replacement (MVR) is associated with increased risk of mitral valve damage. Limited data exist on TAVI in patients with AS who underwent MVR in the past. The novelty of our study is that TAVI in patients after MVR is feasible and transthoracic echocardiography (instead of transesophageal echocardiography) along with fluoroscopy gives satisfactory intraprocedural guidance in most patients.
Introduction
Severe aortic stenosis (AS) is an ever-growing healthcare problem in ageing populations. These patients present a clinical challenge, being often burdened with multiple comorbidities. In patients with aortic stenosis and acceptable operative risk surgical aortic valve replacement (SAVR) remains the gold standard. In symptomatic AS patients who are not suitable for SAVR due to prohibitive or high perioperative risk (EuroSCORE II > 8), transcatheter aortic valve implantation (TAVI) is an alternative recommended by current European Society of Cardiology/European Association of Cardio-Thoracic Surgeons (ESC/EACTS) guidelines. A few of these patients have a history of previous mitral valve replacement (MVR) and their initially mild aortic valve disease eventually progressed to severe AS [1]. TAVI in post-MVR patients is a technical challenge due to the respective proximity of the aortic annulus and non-compliant prosthetic mitral valve ring.
Patients who have undergone mitral valve replacement are at increased risk during TAVI due to possible interference between the mechanical mitral valve and aortic bioprosthesis.
Other MVR-related risks include mitral leaflet damage by guidewires and increased risk of endocarditis at follow-up. Little is still known about the periprocedural course and outcomes on follow-up of patients undergoing such treatment. Trials of the most frequently used TAVI-prostheses have excluded patients with previous MVR.
Although TAVI patients with a history of any previous cardiac surgery constitute up to 30% of all TAVI patients, the large national registries [2–5] surprisingly do not specifically mention post-MVR patients. Probably the first report of TAVI (via the apical approach) in a patient with previous MVR was reported in 2008 [6], followed by one large Spanish registry of 91 patients [7], small series [8–13] and single cases [14–20] (for literature overview see Table I). Current European guidelines on acquired heart valve disease do not cover this valvular scenario.
Table I
Previous reports of transcatheter aortic valve implantation in patients with previous mitral valve replacement
| Author, year of publication | Number of patients | Type of mitral prosthesis | Intraprocedural TEE guidance | Vascular approach | Type of aortic prosthesis | Mitral-aortic distance [mm] |
|---|---|---|---|---|---|---|
| Amat-Santos IJ, 2017 | 91 | Biological (n = 24) Mechanical (n = 67) | No data | F (n = 72) Other (n = 19) | Balloon-expandable valves (n = 51) Other (n = 40) | *** |
| Scholtz S, 2019 | 16 | SJM (n = 9) MA (n = 4) Other (n = 3) | No data | F (n = 13) A (n = 3) | C (n = 7) S (n = 6) DFM (n = 3) | Mean 6.9 |
| Soon JL, 2011 | 10 | Björk-Shiley (n = 1) Sorin (n = 1) Biological (n = 3) SJM (n = 5) | Yes | A | S | – |
| Asil S, 2016 | 6 | Biological (n = 1) Mechanical (n = 5) | No** | F | C | 6–9 |
| Drews T, 2011 | 6* | Physio ring (n = 1); SJM (n = 1), Björk–Shiley (n = 1) Hancock (n = 3); | Yes | A | S | – |
| Beller CJ, 2011 | 5 | Unspecified | Yes for four A | A (n = 4) F (n = 1) | S | Mean 10 |
| Bruschi G, 2009 | 4 | Sorin Monodisc and Bicarbon | approaches | F | C | – |
| Wachter K, 2016 | 2 | Carbomedics and Perimount Plus | No | A | J | – |
| Zacharoulis A, 2015 | 2 | Bileaflet mechanical | Yes | F | S | – |
| Vavuranakis M, 2014 | 2 | Omniscience and SJM | Yes | F | C | 5.8; 9.3 |
| Maluenda G, 2016 | 1 | Starr-Edwards | No | F | C | – |
| Daly MJ, 2015 | 1 | SJM | Yes | Carotid | C | 6 |
| Moon SW, 2014 | 1 | SJM | No ** | F | C | 4.5 |
| Acar B, 2014 | 1 | Single disc | Yes | F | S | – |
| Attia R, 2013 | 1 | SJM | No | A | S | – |
| Testa L, 2013 | 1 | Omnicarbon | Yes | F | C | – |
| Gedikli O, 2013 | 1 | Starr-Edwards | Yes | F | C | 10 |
| Chao V, 2010 | 1 | SJM | Yes | A | S | 3 |
| Dumonteil N, 2009 | 1 | Lillehei-Kaster | Yes | F | S | 9.7 |
| Rodes-Cabau J, 2008 | 1 | SJM | Yes | A | S | – |
Aim
To retrospectively assess the clinical features, detailed echocardiographic and computed tomography parameters, procedural and in-hospital outcomes as well as any valve intervention or major adverse cardiac and cerebrovascular events (MACCE) according to VARC-2 criteria at the same institution at follow-up of patients with a history of MVR and mitral valve valvuloplasty (MVV), who underwent TAVI.
Material and methods
Patient population
All consecutive patients who underwent MVR or MVV before TAVI between July 2010 and September 2019 were identified. Patients’ charts were reviewed in all identified cases. Demographics, prior medical history and clinical characteristics were prospectively collected.
Echocardiographic assessment
All patients underwent complete pre-interventional and post-interventional transthoracic echocardiography (TTE) as well as cardiac and vascular computed tomography. In some transesophageal echocardiography (TEE) was also performed. A detailed description of standard echocardiographic views as well as the computed tomography acquisition protocol and measurements from both modalities is reported elsewhere [21].
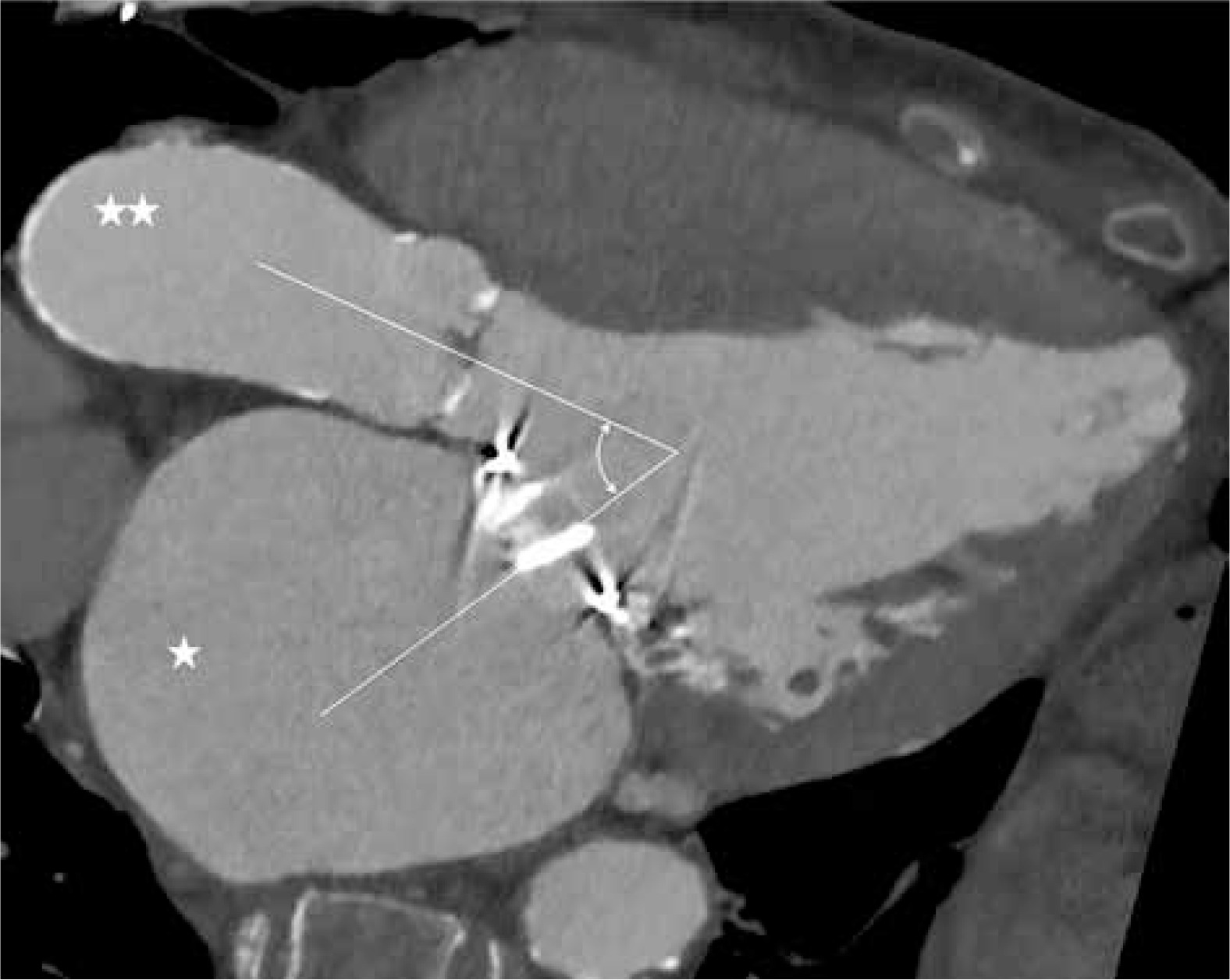
Computed tomography assessment included measurements of: 1) shortest distance between the mitral prosthesis and the aortic annulus (mitral-aortic distance) in the 3-chamber view (Figure 1), 2) angle between axes of mitral and aortic planes (mitral-aortic angle). 3) perimeter of aortic annulus, 4) vertical distance between aortic annulus and coronary ostia. Additionally, screening for vascular access was done routinely (as for any TAVI procedure).
TAVI procedure
The procedure was based on a heart team decision. The technical aspects of TAVI have been described by us in detail previously [22].
Statistical analysis
Continuous variables were expressed as mean with standard deviation (SD) or median with interquartile range (IQR) depending on symmetrical distribution or not, respectively. Categorical variables were expressed as frequency and percentage. Comparative analyses were done using the c2 test or Fisher’s exact test for categorical data, as appropriate.
Numerical variables were assessed with the ANOVA test or Kruskal-Wallis test for non-normally distributed variables. P-values < 0.05 were considered statistically significant. Univariate logistic regression analysis was performed to determine predictors of in-hospital mortality.
Statistical analysis was performed using MedCalc 9.3.8.0 (MedCalc, Marierkerke, Belgium).
Results
Patient population
Overall 628 patients underwent TAVI at our institution in the studied period. Among them were 17 patients after previous MVR (n = 15) or MVV with ring insertion (n = 2). Only patients with previous MVR were included in further analysis. Mean time from mitral valve surgery to TAVI was 15.4 ±5.9 years (range from 4 to 25 years).
In 1 patient the mitral valve was operated on twice. First, a Bjork-Shirley prosthesis was implanted and 15 years later a redo MVR was done with SJM (St Jude Medical, Inc., St. Paul, MN, USA) prosthesis placement.
Types of mitral prostheses: in all patients mechanical prostheses were previously placed and the most frequently used prostheses were the SJM, n = 9, followed by Medtronic Hall, (Medtronic, Inc, Minneapolis, Minn, USA), n = 3, Sorin Bicarbon (Sorin Biomedica, Saluggia, Italy), n = 1, Carbomedics (CarboMedics Inc, Austin, TX, USA), n = 1 and unspecified, n = 1.
Indication for TAVI and preoperative assessment
All patients presented with AS in the native aortic valve. Demographics and baseline clinical data are presented in Table II. Echocardiographic and computed tomography data are shown in Table III. Mean aortic valve area (AVA) was 0.65 ±0.21 cm2 and mean transaortic gradients were 73.9 ±21.1 mm Hg and 45.9 ±13.7 mm Hg, max and mean, respectively. The distance between the mitral prosthesis and the aortic annulus ranged from 4 to 14 mm, mean 8.6 ±2.5 mm. The angle between the mitral prosthesis and aortic valve planes ranged from 37 to 78°, mean 53 ±11°. EuroSCORE II was 8.7 ±3.7.
Table II
Baseline characteristics of patients after mitral valve replacement (n = 15)
[i] AMI – acute myocardial infarction, BAV – balloon aortic valvuloplasty, CABG – coronary artery bypass grafting, HF – heart failure, NYHA – New York Heart Association, PCI – percutaneous coronary intervention, SD – standard deviation, TVR – tricuspid valve replacement, TVV – tricuspid valve valvuloplasty, WBC – white blood cells, Hgb – haemoglobin, eGFR – estimated glomerular filtration rate, hsCRP – high sensitivity C-reactive protein.
Table III
Pre-procedural computed tomography measurements, pre- and post-interventional echocardiography and procedural data
[i] AR – aortic regurgitation, AVA – aortic valve area, AVR – aortic valve replacement, IQR – interquartile range, LMCA – left main coronary artery, LVEDD – left ventricle end diastolic diameter, LVEF – left ventricle ejection fraction, LVOT – left ventricle outflow tract, MR – mitral regurgitation, PASP – pulmonary artery systolic pressure, SD – standard deviation, PCI – percutaneous coronary intervention, RCA – right coronary artery, TTE – transthoracic echocardiography, TAVI – transcatheter aortic valve implantation, TEE – transesophageal echocardiography.
TAVI procedures
In all but 1 patient vascular access was via the femoral artery. In 1 case the subclavian artery was used.
Only in 1 patient was the TAVI procedure performed with TEE guidance. In other patients we assessed mitral valve function during TAVI by observing the mobility of mitral valve discs and blood pressure. The most frequently used prosthesis during TAVI was EVOLUT R (n = 7), followed by CoreValve (n = 4), SAPIEN XT (n = 3) and ACCURATE (n = 1). Mean aortic prosthesis diameter was 28.5 ±2.7 mm. In all patients the prosthesis was successfully deployed. Predilatation was used in 11 (73.3%) cases and postdilatation was done in 6 (40%) cases. One patient developed cardiac tamponade during prosthesis deployment. This was successfully treated with pericardiocentesis. In 1 patient the EVOLUT-R prosthesis was implanted above the coronary ostia.
A significant drop of mean and maximal transaortic pressure was noted, 38.3 ±14 and 58.6 ±27.6 mm Hg, respectively. No significant change of mitral gradient or dysfunction of the mitral prosthesis was observed.
All patients were discharged home. Pharmacological treatment included oral vitamin K antagonist in all patients, acetylsalicylic acid in 6 patients and a double antiplatelet regimen in 1 patient.
Follow-up
Infection
One female patient developed infective endocarditis with infiltrations on the leaflets of the aortic bioprosthesis 6 years after TAVI. This was successfully treated with vancomycin and subsequently with teicoplanin.
Re-intervention
A patient in whom the prosthesis was implanted above the coronary ostia developed progressive stenocardia. Thus, percutaneous coronary intervention with “chimney” stenting of the left main coronary artery was performed 5 months after TAVI.
Death
Two patients died shortly after hospital discharge. One male patient treated with oral vitamin K antagonist and acetylsalicylic acid (75 mg) died suddenly 11 days after the TAVI procedure due to possible internal bleeding. One female patient developed sepsis with blood cultures positive for Staphylococcus aureus. Despite antibiotic therapy she died 48 days after TAVI.
There were no other MACCE.
Discussion
The main findings of our study are that TAVI in patients after mechanical MVR is feasible and TTE (instead of TEE) along with fluoroscopy gives satisfactory intraprocedural guidance in most patients. Not a single case of acute intraprocedural or postprocedural dysfunction of the mitral prosthesis was observed. Thus, despite potentially increased risk of the procedure (compared to TAVI in patients with a native mitral valve) it can be performed without complications in the majority of cases. Vigilance for possible complications at follow-up is essential.
Role of echocardiographic and computed tomography evaluation
The role of pre-interventional work-up with computed tomography and echocardiography has been discussed in detail before [23, 24]. In regard to the intraprocedural TEE guidance, available evidence from previous trials does not support its routine use. In our series of patients, intraprocedural TEE guidance was used in only 1 patient for SAPIEN prosthesis implantation. In the rest of patients fluoroscopy guidance with TTE done only immediately after the procedure was satisfactory. In general, TEE guidance may be reserved for patients with an extremely poor TTE window. Similarly, in a single-center retrospective analysis no differences in regard to periprocedural complications and 30-day readmissions were seen between subgroups with TEE guidance (n = 104) versus without (n = 74) [25]. TEE guidance was not associated with a lower incidence of moderate and severe paravalvular leak in another observation, either [26]. Data from a large France TAVI registry (more than 12,000 patients) indicate that TEE guidance decreased from 60% to 32% of cases over a period ranging from 2013 to 2015 [6]. However, patients after MVR pose a greater challenge during TAVI and some authors underscore the essential role of TEE guidance. Thus, in most of the reported cases, intraprocedural TEE guidance was used (Table I). No such data from the above-mentioned Spanish registry are available. Next, what also matters is the type of mitral prosthesis. A radio-opaque mechanical valve seems suitable for X-ray guidance, whilst a radio-lucent bioprosthesis may require TEE guidance.
Technical steps
Most tips and tricks have been presented elsewhere [27]. Let us just draw attention to several key points.
Prophylactic intravenous antibiotic therapy (cefuroxime 1.5 γ or cefazoline 1 g) was administered 30 to 60 min before TAVI. If the procedure lasted > 4 h, an additional dose of antibiotic was given.
Aortic valve pre-dilatation was done in 11 of 15 our patients (in three of them before balloon-expandable SAPIEN). Some authors suggest that such pre-dilatation with a balloon of a similar size to the valve stent under TEE guidance may be an indicator of the compression effect of the aortic annulus on the mitral prosthesis [28].
Prosthesis type: Procedural success can be achieved with any of the commercially available valves. We have obtained no data pointing to possible advantages of choosing one type of valve over another in this small group of patients. The limited number of patients in our study gives no statistical power to such analysis. However, previous papers suggested possible advantages of self-expanding prostheses (although they do have a longer stent frame compared to the balloon expandable SAPIEN prosthesis), which are partially recapturable during adjustment [18]. Thus, should the discs of the mitral prosthesis show any signs of acute dysfunction during deployment of the aortic prosthesis, the position of the latter may be corrected.
Possible specific complications
Interference between mitral and aortic prostheses
Too small a distance between both prostheses (depending also on the mitral-aortic angle) may cause acute/delayed dysfunction of both prostheses.
Previous papers reported at least two cases of acute mitral prosthesis malfunction with a fatal outcome after TAVI in patients after previous MVR [13]. In the Spanish registry aortic prosthesis embolization occurred in 6.7% [7]. Still, as these two factors (mitral-aortic distance and angle) interplay in creating possible interference between aortic and mitral prostheses, they should be jointly assessed during pre-interventional planning.
Different minimal mitral-aortic distances have been proposed as a measure (Table 1) to avoid any interference of prostheses:
In all patients from the Spanish registry in whom the device embolized, mitral-aortic distance was < 7 mm.
Surprisingly, previous papers paid no attention to the mitral-aortic angle. Furthermore, no impact of this angle on the occurrence of aortic prosthesis embolization was found in the Spanish cohort.
Obstruction of the coronary arteries
The obstruction of coronary flow in one of our patients was clearly caused by the prosthesis having been implanted above the coronary ostia, and thus subsequent tunneling via “chimney” stenting of the left main coronary artery seemed a reasonable option. The risk of coronary obstruction (CO) was broadly investigated before, among others by Arai et al. [29] and Ribeiro et al. [30]. Anatomical parameters indicative of higher CO risk were mainly lower-lying coronary ostium (< 10 mm) and shallow sinus of Valsalva, and in the case of SAPIEN XT valve height/coronary height.
Bleeding
One of our patients died within 1 h after hospital re-admission with strong suspicion of internal bleeding. Indeed, results from the Spanish registry indicated that among patients undergoing TAVI, those with previous MVR had significantly higher risk of bleeding compared to the non-MVR group [7].
Optimal intraprocedural anticoagulation with unfractionated heparin (UFH) dosage was according to the patients’ weight (initial bolus of at least 5000 IU). Activated clotting time was maintained > 250 s. As opposite to standard TAVI, no subsequent reversal using protamine sulfate was done in patients after previous MVR. Low molecular weight heparin (enoxaparin) was administered 4 h after completion of the procedure. Vitamin K antagonists were re-initiated the next day (with overlapping UFH if needed).
Limitations
The retrospective nature of our study with a limited number of patients precluded more detailed statistical assessment.
Follow-up observations were limited to same-hospital readmissions and any re-interventions or same hospital outpatient clinic visits. Hospitalizations in other hospitals could not be ruled out.
Conclusions
TAVI may be safely performed in patients after previous MVR. Meticulous preoperative procedure planning with a multidisciplinary team is mandatory for optimal results. Bleeding may have potentially fatal consequences in some patients due to intensive anticoagulation and (in some cases) concomitant antiplatelet treatment.







