
INTRODUCTION
Sebaceous adenoma (SA) is a benign skin tumor of sebaceous origin most commonly occurring within the head and neck area in the middle-aged or elderly individuals [1, 2]. Dermoscopy of SA is underinvestigated, with about 30 cases reported in the literature (and almost all in association with Muir-Torre syndrome; MTS) [2–8]. While the most characteristic dermoscopic feature suggesting the diagnosis of tumor of sebaceous origin is the presence of yellow color, in the reported case, lesions presented with pink and brown-grayish coloration.
CASE REPORT
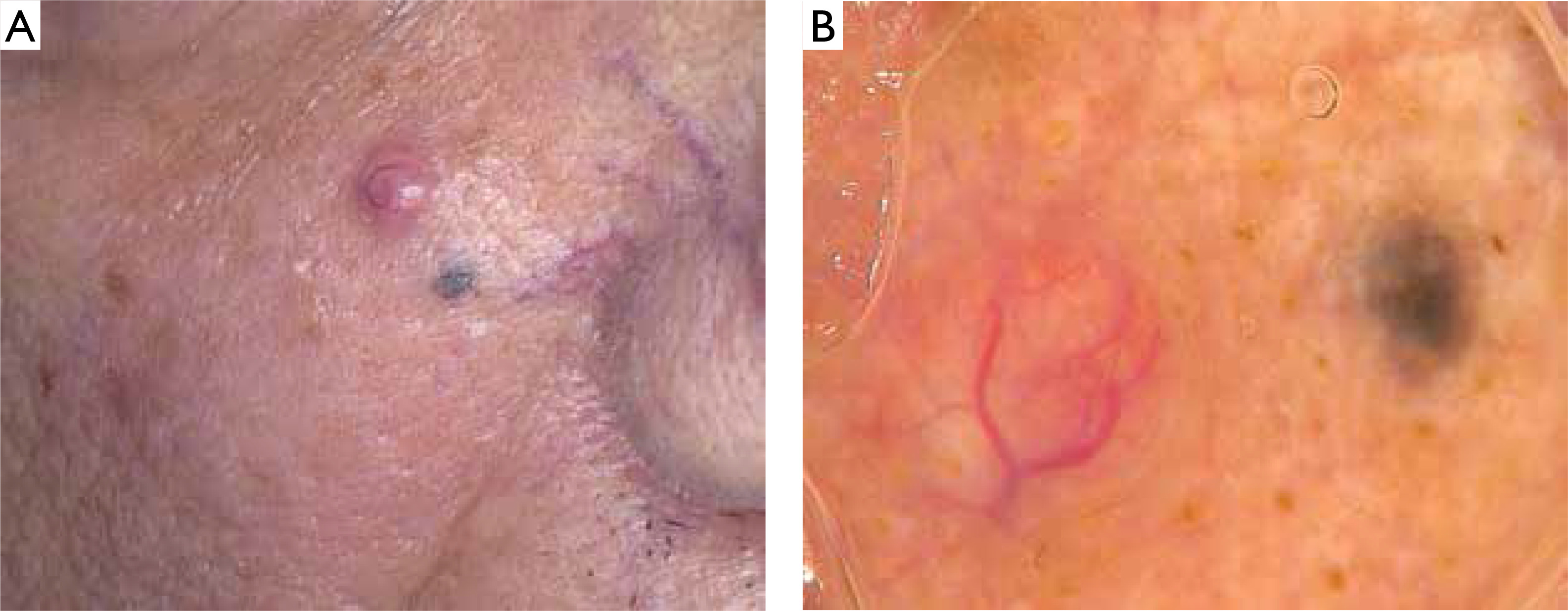
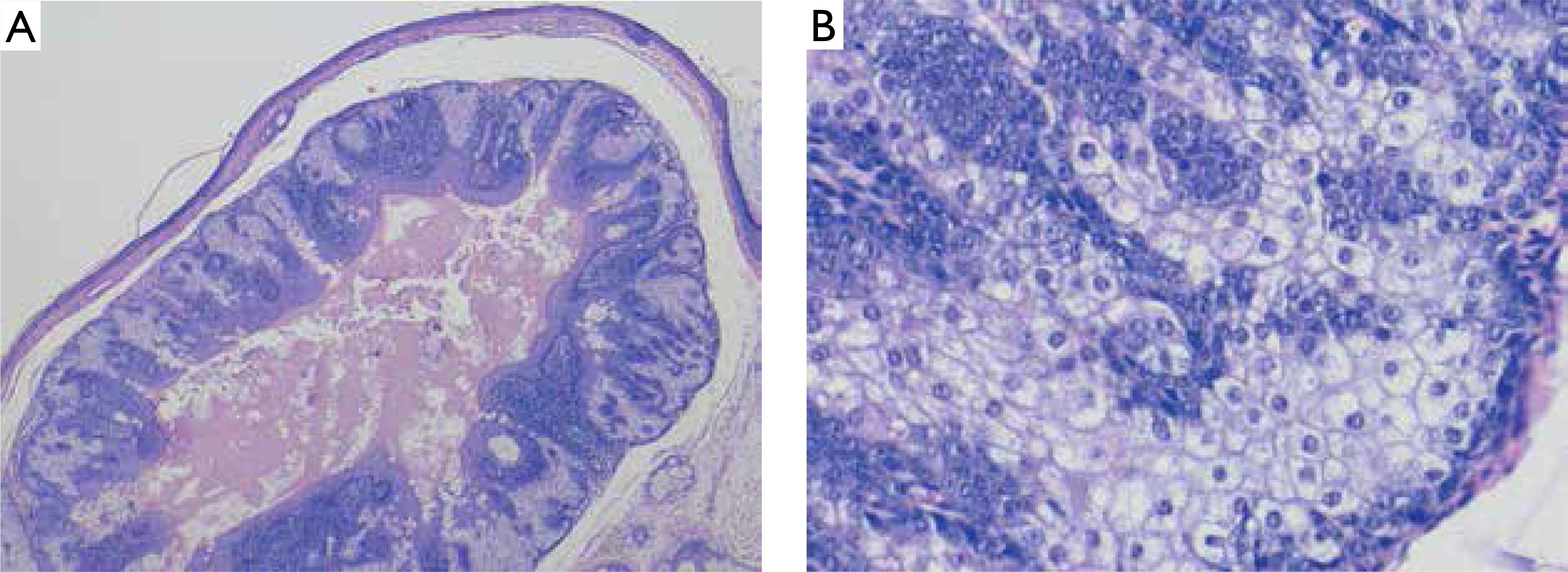
An 80-year-old man (phototype II), presented with amelanotic, non-ulcerated tumor on the right cheek and adjacent dark macule (Figure 1 A). Personal and family history of skin cancer was negative. On dermoscopy, the nodular lesion showed pink branched vessels within the tumor and brown-grayish structureless pattern in the macule (Figure 1 B). Both lesions were excised, and histopathological evaluation showed the architecture of SA in both of them with preserved expression of MLH1, MSH2, MSH6 and PMS2 (Figure 2). Neither signs of recurrence, nor other signs of MTS, have been observed on 12-month follow-up.
Figure 1
A – Clinical presentation – amelanotic, non-ulcerated tumor on the right cheek and adjacent dark macule; B – Dermoscopy shows pink branched vessels within the tumor and brown-grayish structureless pattern in the macule (FotoFinder, camera Medicam 800 HD, 20× magnification, non-polarized mode with ultrasound gel as an immersion fluid)
DISCUSSION
SA is a benign skin tumor that usually presents as a flesh-colored, asymptomatic nodule. These lesions most commonly occur within the head and neck area, although they may be present in any anatomical region [1]. As multiple sebaceous adenomas most commonly occur in the spectrum of MTS, it is recommended to perform evaluation of mismatched repair proteins (MSH2, MLH1, MSH6, and PMS2) as an initial screening test. MTS is a rare autosomal dominant genodermatosis characterized by the presence of sebaceous gland tumors and/or keratoacanthomas associated with gastrointestinal and genitourinary neoplasia. The lack of expression of the mentioned proteins in a sebaceous tumor should warrant microsatellite instability (MSI) analyses. Detection of MSI is an indication for cancer surveillance and examination of the patient’s family.
Dermoscopy of SA is still poorly investigated, with about 30 reported cases. Moscarella et al. [3], who included 18 sebaceous adenomas from 6 patients with MTS, defined two main dermoscopic patterns (which could be observed in different tumors from one patient). Lesions with a central crater dermoscopically showed elongated radial telangiectasias (crown vessels) enfolding structureless ovoid white-yellow center (sometimes covered with hemorrhagic crust). Lesions without a central crater revealed branched, blurred vessels over a white to yellow background and several yellow comedo-like globules. Further observation of 5 cases by Lallas et al. [4] generally confirmed this observation, and it was concluded that the combination of yellowish structures with unfocused arborizing vessels is suggestive of a sebaceous tumor, however, precise differential diagnosis is problematic. Observations from other reported cases are generally in line with this knowledge [5–8]. Our case is unique due to the lack of yellow structures on dermoscopy and a completely different picture of two tumors with similar histopathological architecture located in one anatomical area. As expression of MLH1, MSH2, MSH6 and PMS2 was preserved in both lesions and no MTS signs were observed, we assume that they could be classified as MTS-unrelated SA. It is possible that different genetic background could influence the clinical and dermoscopic presentation in the described case.
CONCLUSIONS
SA is a relatively rare adnexal tumor that should be considered in differential diagnosis when a combination of yellowish structures and unfocused arborizing vessels is observed on dermoscopy. Possible other dermoscopic presentations (with no yellow color) are branched vessels and brown-grayish structureless pattern.










