
A 50-year-old man, with one-month effort angina and a history of hypertension and dyslipidemia, was subjected to coronary angiography (CA), via the left radial approach, which revealed single-vessel chronic total occlusion (CTO) of the mid-right coronary artery (RCA) (Figures 1: Ia, b). The left ventricle ejection fraction (LVEF) was 50% with hypokinesia at the infero-lateral wall. Since the patient was recently symptomatic with a positive stress test and a relatively low J-CTO Score ≈ 2, an ad-hoc percutaneous coronary intervention (PCI) was decided, with the patient’s informed consent. In our cath lab, for the last three years, there has been a newly engaged CTO program including two operators with ≥ 20 CTO procedures per year and a total volume of 50 CTOs/year and both of them were involved in the present procedure.
Figure 1
Ostial RCA dissection extending retrogradely into the RSOV (“contrast staining” in the RSOV, yellow asterisk) and antegradely in the RCA (IIIb). Stent dislodgement, swinging in the aorta (Va, black arrow). Final angiographic result: TIMI III flow in the RCA (VIb, c)
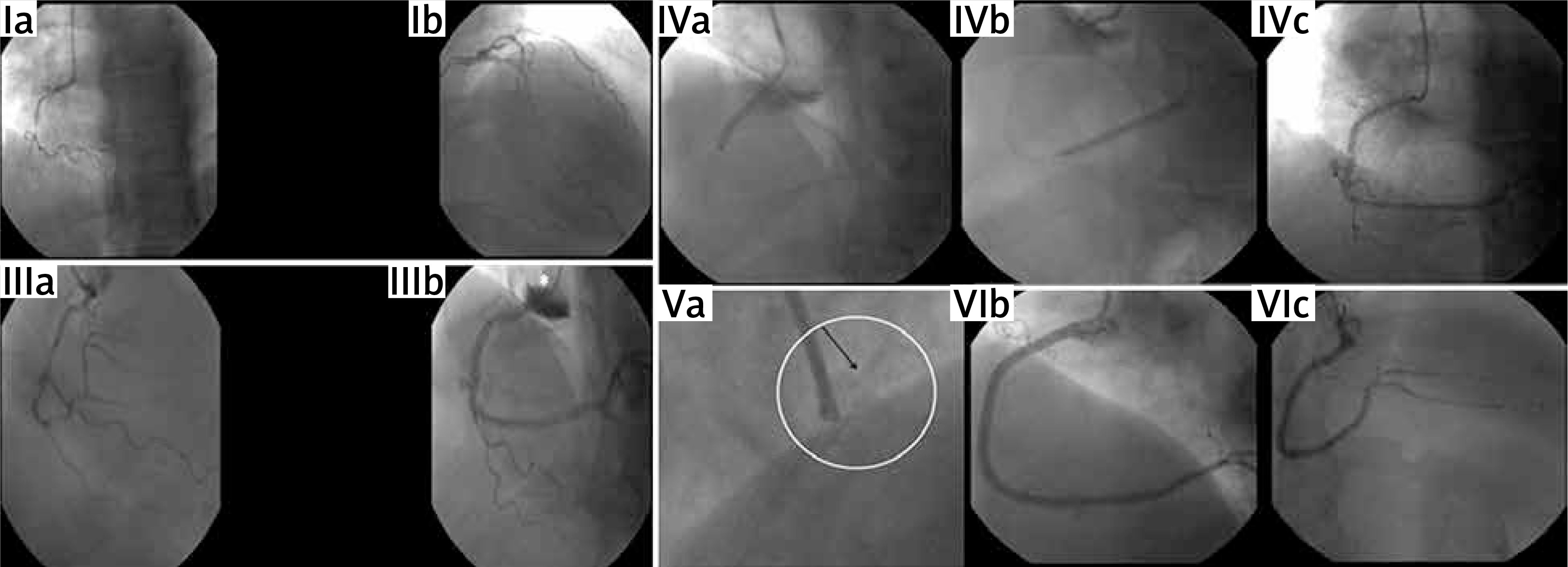
After RCA engagement with a 6F, Amplatz-Left (AL) 1 guiding-catheter, the CTO lesion was crossed with ProVia-6-guidewire. After several predilatations and a failed attempt to deliver a 2.75 × 28 mm drug-eluting stent (DES) (Xience PRO-A) – due to the occurrence of a dissection distally Figure 1, IIIa) – the patient complained about severe chest pain and a drop in his blood pressure was noticed. The subsequent contrast injection revealed contrast staining in the right Valsalva sinus (RSOV) and ostial RCA dissection (Figure 1. IIIb). A 3 × 32 mm DES (Supraflex Cruz) was deployed immediately proximally to seal the entry point at the RCA ostium (Figure 1, IVa). Transthoracic echocardiogram performed intra-invasively showed no intimal flap, aortic valve regurgitation (AVR) or hemopericardium. Another 2.75 × 32 mm DES (Xience PRO-A) was distally implanted to cover the initial dissection (Figure 1, IVb, c).
After forceful attempts to deliver a 3.0 × 28 mm DES (Supraflex) in the mid-RCA, the stent was dislodged and trapped by the struts of the ostially implanted stent. Crushing of the dislodged stent with a 3.5 × 23 mm DES (Xience PRO-A) was performed and a 3.0 × 28 mm DES (Xience PRO-A) was successfully implanted in the mid-RCA. Final angiogram showed both elimination of contrast staining at the RSOV and TIMI III flow in the RCA (Figure 1, V-VI).
The emergency computed tomography angiography (CTA) showed a subtle intramural hematoma at the RSOV, without active dissection. Anticoagulation therapy was not sustained and dual antiplatelet therapy was continued.
The higher incidence of coronary perforations during CTO management has been established in previous studies [1]. Iatrogenic aortic dissection (IAD) is a rare, yet potentially catastrophic complication of CA or PCI with an overall incidence of < 0.06%, which is higher in the setting of acute myocardial infarction (AMI) and CTO procedures [2–7]. RCA is the most frequently involved vessel. Guiding catheter, followed by guide-wire induced traumas are the most common causes, while AL and Judkins-Right guiding catheters for RCA engagement are usually involved [2, 4, 5, 7].
The optimal IAD management after its occurrence is unclear. If the patient is hemodynamically stable and there are no complications (AMI, hemopericardium, AVR, cerebral malperfusion) sealing the coronary entry-point of the dissection with a stent to prevent its extension seems reasonable, as it may prevent the need for high-risk urgent surgery [2–4, 6]. We propose that once IAD occurs, every effort should be undertaken to seal the entry-point by immediate coronary ostial stenting.
The best approach for IAD management, however, remains its prevention. Consequently, the use of aggressive catheters should always be balanced against the need for support, while coaxial alignment of the catheter needs to be ensured. In addition, if IAD occurs, contrast injection should be restricted to avoid rapid and extensive expansion. IVUS guided management has been reported as a helpful approach in this setting. In our case, after managing the IAD, the use of an undersized DES for ostial sealing in combination with the following forceful efforts for stent advancement – which should be generally avoided – in the mid-RCA further complicated the procedure with stent dislodgment. Crushing of the dislodged stent, if feasible, is a life-saving approach.







