
Pre-procedural planning to guide structural heart interventions is often demanding and requires experience in cardiac imaging. Left atrial appendage (LAA) morphology is often complex [1] and variable. Transesophageal echocardiography (TEE) alone may not always be optimal to size the device adequately. Even experienced echocardiographers in certain conditions may sometimes have difficulty with proper sizing of the devices. Compared to TEE, computed tomography (CT) results in larger LAA orifice measurements, improves odds of predicting correct device size, and reduces fluoroscopy time in patients undergoing LAA occlusion [2]. Application of 3D printing, computational modeling, and ultimately incorporation of artificial intelligence are changing the landscape of today’s cardiac interventions [3].
Here we present 5 cases of LAA occlusion with additional use of artificial intelligence (AI) enabled technology FEops performed in the First Department of Cardiology in Katowice.
Case reports
Case 1
An 84-year-old man with persistent atrial fibrillation (CHA2DS2-VASc 6 points, HAS-BLED 4 points) was admitted for implantation of a left atrial occluder because of recurrent intestinal bleeding. Transthoracic echocardiography (TTE) revealed an enlarged left atrium with moderate valvular dysfunctions. In CT thrombus was excluded. Planning with FEops revealed a 2-lobed appendage with a very short but adequate landing zone (Figure 1). The AI simulated devices were the Amulet 22 mm, 25 mm, 28 mm, and 31 mm. According to our opinion and review of delivered simulations, taking into consideration frame deformation and the gap between the device and the wall of the appendage we chose a 25 mm device with high confidence for implantation. The stability was confirmed with a tug test. Proper placement of the device was confirmed in TTE on the next day, and in 2 months follow-up TEE. No complications were observed.
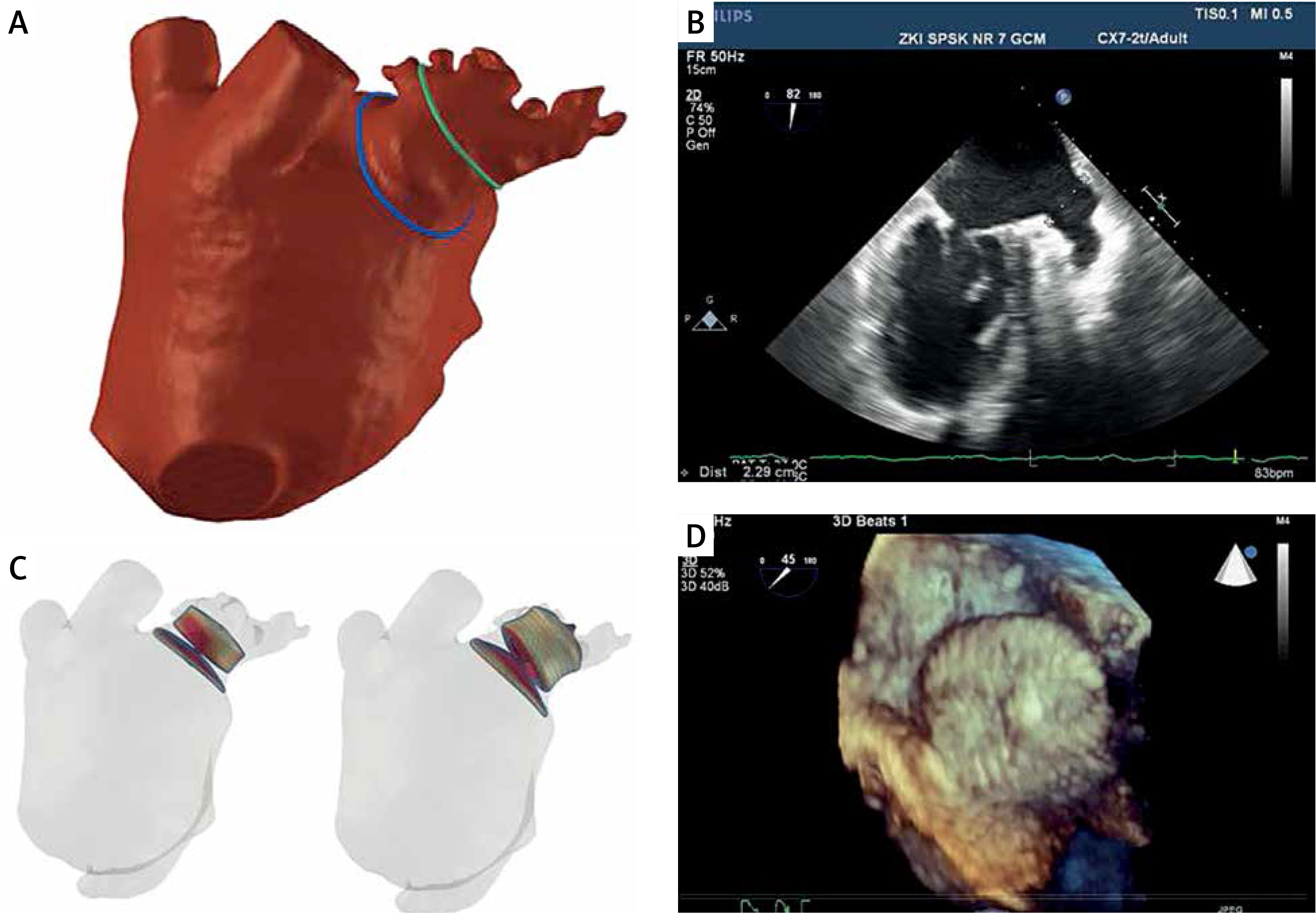
Figure 1
Combined visualization of the appendage using FEops and intraprocedural echocardiography. FEops clearly demonstrates 2-lobed structure (A) with short landing zone. Traditional intraprocedural echocardiography measured landing zone 2.29 cm (B) at the borderline of device sizes 25 and 28 mm. We chose the 25 mm device size based on our preassessment and FEops. The figure shows sample simulation for the 22 mm device with a clear gap in the red color and 25 mm with no gap and proper device deformation (C). We implanted the device with very good sealing (D) and positive follow-up
Case 2
A 74-year-old woman with persistent atrial fibrillation (CHA2DS2-VASc 5 points, HAS-BLED 4 points) was admitted for implantation of a left atrial occluder because of recurrent persistent anemia without apparent cause despite diagnostic tests, and intolerance of NOACS. Transthoracic echocardiography (TTE) revealed an enlarged left and right atrium without other apparent abnormalities. In CT thrombus was excluded, and LAA type 2C was observed with a very high degree of trabeculations. The simulated devices were Amulet 20, 22, 25, and 28 mm. According to our opinion and prior assessment of delivered simulations we chose the 22 mm device for implantation. The stability was confirmed with a tug test. Proper placement of the device was confirmed in TTE on the next day and in 3 months’ follow-up. No periprocedural complications were observed.
Case 3
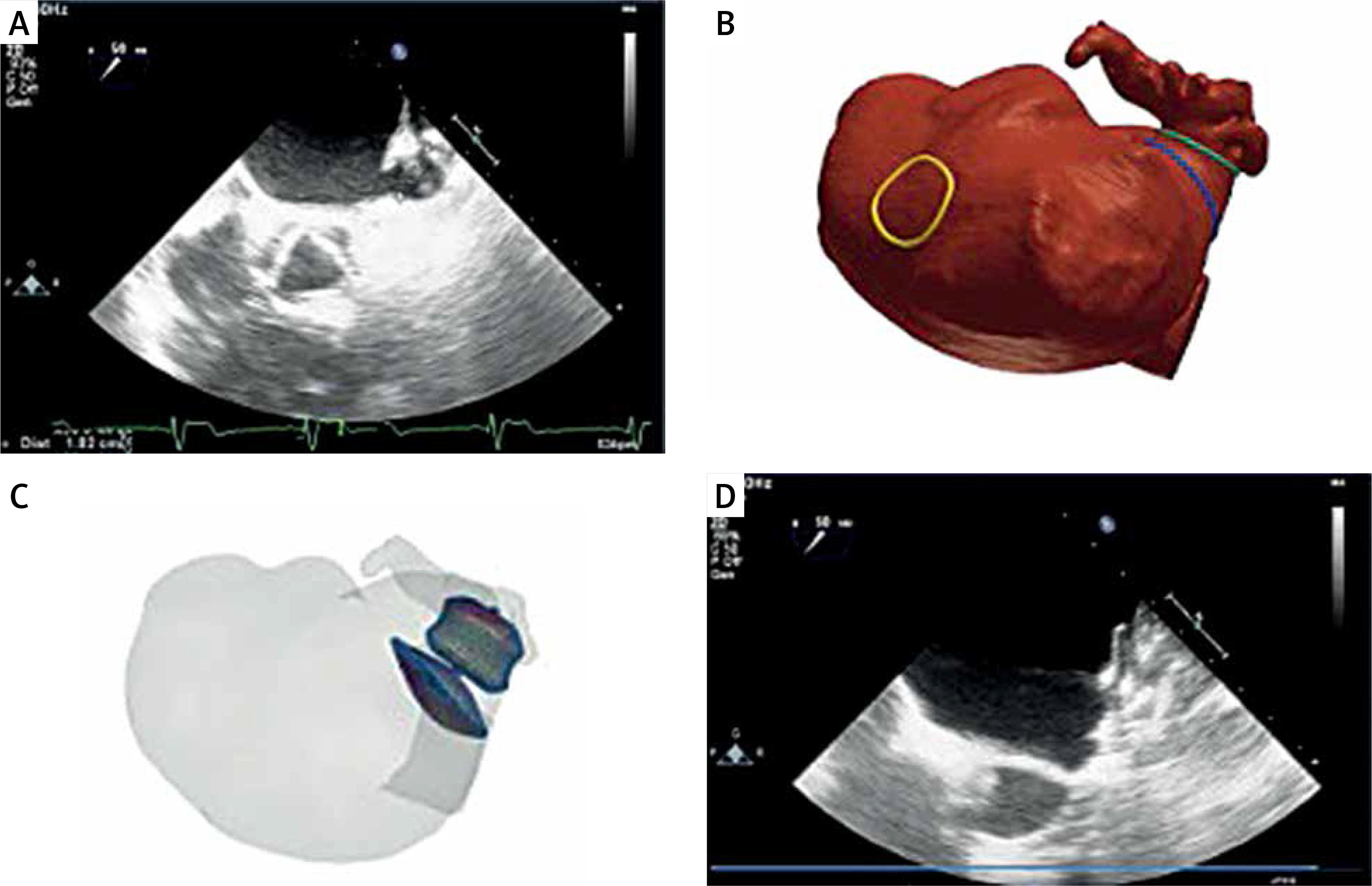
A 79-year-old woman with paroxysmal atrial fibrillation (CHA2DS2-VASc 4, HAS-BLED 3 points) was admitted to our hospital for LAA closure due to recurrent bleeding from the gastrointestinal tract of unknown cause. Preprocedural echocardiography was very demanding because of the anatomy of the appendage. Measurements of the right device size by TEE were not possible to perform adequately due to very difficult visualization. CT was performed and revealed chicken wing anatomy of the LAA and excluded presence of thrombus (Figure 2). The case was assessed with FEops and an Amulet 22 mm was finally used after personal analysis. No complications occurred and the device was stable with good sealing in the follow-up. In this patient measurements by FEops were crucial for our team.
Case 4
A 76-year-old woman with paroxysmal atrial fibrillation (CHADS-VASC-5, HAS-BLED 3 points) and 1st degree atrioventricular block was admitted for LAA occlusion because of multiple central nervous system aneurysms and contraindications for anticoagulant therapy according to the neurologist’s consultation. TTE revealed thickening of the interventricular septum and enlarged left atrium with mild mitral incompetence. In CT thrombus was excluded. The FEops simulated devices were Amulet 22, 25 and 28 mm. According to our opinion and review of delivered simulations and intraprocedural echocardiography we chose the Amulet 25 mm for implantation. The stability was confirmed with a tug test. The next day after the procedure, elevated creatinine values above 2 mg/dl were found, which returned to normal the next day after adequate pharmacological treatment. Proper placement of the appendage device was confirmed in TTE on the next day after the procedure and in TEE 3 months post-operatively.
Case 5
An 84-year-old woman with persistent atrial fibrillation (EHRA 1, CHA2DS2-VASc 7, HAS-BLED 5 points) and multivessel coronary artery disease was admitted for implantation of an LAA occlusion device because of gastrointestinal bleeding on different anticoagulant drugs. TTE revealed atrial dilatation, ventricular septal hypertrophy, mild mitral regurgitation and severe tricuspid regurgitation. In TEE thrombus was excluded – the landing zone measured 22 mm. CT showed 1st type of LAA with LAA width of 25 mm. The simulated devices were Amulet 25, 28 and 31 mm. Despite large differences in measurements between TEE and CT we chose the 28 mm device for implantation as suggested by FEops simulation. At first impression the device seemed too large based only on echocardiographic measurements, but we achieved a very good position of the device without problems. The stability was confirmed with a tug test. Proper placement of the device was confirmed in TTE on the next day. No complications and no pericardial effusion were observed in follow-up.
Discussion
Despite the emerging role of intracardiac echocardiography, TEE still remains the gold standard for intraprocedural guiding in structural heart interventions. Nowadays pre-procedural planning may be performed using less invasive diagnostic methods. Our procedures were performed traditionally with the standard protocol and CT preassessment, with additional use of FEops. LAA occlusion is a procedure in which complications such as device leak, myocardial injury, and device embolization can be decreased substantially with incorporation of proper imaging and digital tools [4]. Studies show that CT-based selection of LAA occlusion device size may be a more precise method than conventional TEE [5]. Moreover, computational modelling like FEops accurately predicts device deformation and apposition and may potentiate more complete LAA occlusion [6]. Use of computational modelling may have many benefits, but high CT quality requires adequate equipment and a specific study protocol. Use of the dedicated website is very intuitive and easy to navigate. Different device sizes and position simulations (usually 4–5) are delivered by FEops, and it is up to operators to choose the best one based on personal analysis (Table I). In our view a great advantage of the system is that it also delivers optimal X-ray angulations for operators, thus limiting unnecessary non-optimal angiographical views during intervention, especially in specific anatomies. Moreover, the suggested depth of implantation is sometimes controversial and FEops facilitates an intraoperative decision as in our third case. In our opinion, preplanning with FEops shortens the time of the procedure and of periprocedural TEE. In the majority of cases the whole procedure may be performed under local anesthesia. In the authors’ view FEops’ main advantage is for low to medium volume operators as the level of confidence of the right device size selection, especially in challenging anatomies, is very high. One must always remember that intra-procedural assessment still remains core for this procedure.
Table I
Left atrial appendage width in TEE final occluder used as assessed by FEops analysis
| Case | CHA2DS2-VASc | HAS-BLED | TEE [mm]/landing zone | FEops [mm] | Occluder used [mm] |
|---|---|---|---|---|---|
| 1 | 6 | 4 | 23 | 25, 28, 31 | 25 |
| 2 | 5 | 4 | 19 | 20, 22, 25, 28, | 22 |
| 3 | 4 | 3 | 19 | 18, 20, 22, 25 | 22 |
| 4 | 5 | 3 | 20 | 22, 25, 28 | 25 |
| 5 | 7 | 5 | 20 | 25, 28, 31 | 28 |
Results of randomised predict LAA-LAA [7] study testing weather preprocedural planning for LAA closure with Amplatzer- Amulet device based on patient specific computational simulations results in more efficient procedure and outcomes were released in 2022 TCT meeting. It demonstrated added value of AI-enabled, CT-based computational modelling when planning for percutaneous LAA closure with improved procedural efficiency, safety and efficacy.







