
Summary
Significant progress in interventional cardiology made radial access a real alternative to a femoral approach in percutaneous coronary intervention (PCI). However, it carries some risk of local or long-term complications such as hematoma or radial artery occlusion. Recently, more distal radial access has been proposed. This distal transradial access in the anatomical snuffbox was suggested to have some advantages over the standard radial site in terms of better comfort of both patient and operator and potentially decreased the risk of local complications and radial artery related complications. Here, we report our initial experience of the very distal left and right transradial approach (VITRO) for acute stage coronary interventions. To our knowledge this is the first report of such experience in Poland.
Introduction
There is always constant progress in interventional cardiology. It includes not only new methods such as treatment of structural heart diseases but also more advanced techniques of percutaneous coronary interventions (PCI). Initially, the femoral approach was used for coronary interventions (CI). However, currently trans-radial access is strongly preferred [1]. It was proven to be superior to femoral access with significant mortality reduction especially in acute coronary syndromes (ACS) [2]. Moreover, radial access is associated with significantly lower rates of vascular complications including major bleeding [3]. What is important, the radial approach when compared to femoral access provides greater comfort for treated patients [4]. However, it is right radial access which is usually used, and after the intervention a transradial compression wristband is applied with compression time up to 120 min. Transradial access carries some risk of local complications. Furthermore, application of the wristband may cause significant patient discomfort and sometimes painful hand swelling. Recently, more distal radial access has been proposed [5, 6]. This distal transradial access in the anatomical snuffbox was suggested to have some advantages over the standard radial site in terms of better comfort of both patient and operator and potentially lower risk of local complications and radial artery occlusion.
Aim
The aim of the current study was to assess the feasibility of even more distal transradial access (very distal transradial approach – VITRO) in consecutive patients submitted to diagnostic or therapeutic CI. The success rate of very distal arterial access, the time from the first puncture to the guidewire insertion and the complication rate were assessed.
Material and methods
The study included consecutive patients aged over 18 years referred to our catheterization laboratory for diagnostic coronary angiography or for PCI as the primary procedure in ACS or for elective CI. We did not include patients with ST elevation myocardial infarction, subjects in cardiogenic shock or patients in whom brachial or ulnar access was preferred, for example patients with forearm dialysis fistulas. All patients signed written informed consent forms. The VITRO study was approved by the Local Ethics Committee (KB 145/2018).
Procedures were performed by four operators experienced in the traditional radial approach. For the current study we used very distal radial access in the area of the anatomic snuff box (VITRO) (Figure 1).

The selection of left or right arterial access was predominantly based on the presence of a well-palpable distal radial artery and also on the operator’s preference.
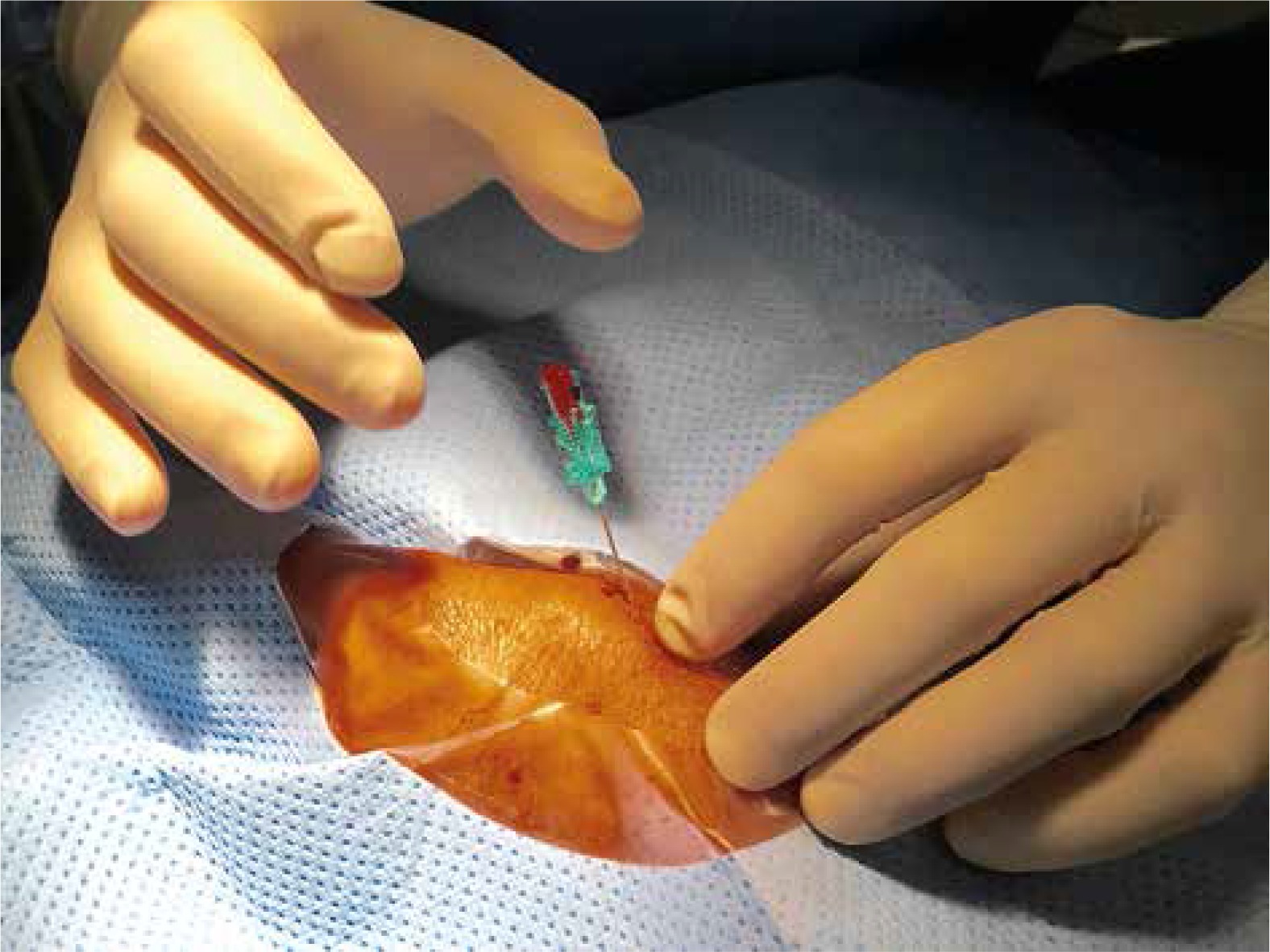
The left upper limb was placed comfortably on the lower abdomen of the patient while the right forearm was placed as in the traditional radial approach, but without palm supination. After manual localization of the radial pulse laterally to the extensor pollicis longus, de facto in the area of the functional snuff box, arterial puncture was performed. After the localization of a well-palpable radial artery, without ultrasonic guidance and after skin disinfection, local anesthesia (5–10 ml of 2% lignocaine) was injected subcutaneously in the area of the snuff box, with a small gauge needle. After 1–2 min the distal radial artery was punctured) with a 21 gauge open needle using a “dancing needle” technique (Figure 2).
Figure 2
“Dancing needle” – characteristic pulsing of the needle just before puncture of the artery wall
Caution was paid to puncture only the anterior atrial wall. Then a vascular 0.018” introducer or 0.014” coronary wire and 7–11 cm 6 Fr introducer sheath were inserted (Prelude, MeritMedical or Radifocus, Terumo). After the insertion of the sheath, the arterial pressure and heart rate were measured. If the patient’s systolic BP was above 100 mm Hg, 100–200 µg of nitroglycerine and 5000 U of unfractionated heparin were given through the sheath to prevent radial artery thrombosis. Subsequently the procedure was continued in the usual fashion according to its type. We assessed the success rate and the time from the patient’s preparation to the first record with a vascular sheath inserted into the radial artery.
After the procedure the sheath was retrieved partially, with a radial hemostatic band placed in a similar way to the traditional approach but more distally, with the pumped pillow adhering to the puncture site. The band covered the thenar area and metacarpus, but not the wrist (Figure 3).
Figure 3
Site of VITRO puncture covered with a hemostatic band (Io TM Radial Artery Compression Tourniquet, COMED B.V.)

The site of radial artery puncture was subsequently covered with a small aseptic gauze covered with hemostatic band. Prior to discharge from the laboratory, distal radial pulses in the wrist and at the puncture site were assessed.
Results
Between March 2018 and September 2018, 320 patients entered the Vitro program. In 112 (32%) patients the radial pulse in the snuffbox area was not palpable or was too weak and they were referred for the traditional radial approach. Thus, eventually we included 218 consecutive patients (142 male, 76 female, mean age: 69 ±11 years) referred for coronary angiography, elective angioplasty or primary PCI in ACS. In 165 (75.7%) patients elective procedures where performed while in 53 (24.3%) subjects indications for urgent CI were present. Detailed patients’ characteristics are presented in Table I.
Table I
Clinical characteristics of all patients and patients with puncture failure
The success rate of the very distal approach was 89.4% in patients with a palpable radial pulse in the snuffbox area, and 60.1% of 320 patients who entered the Vitro program. In 9 patients arterial puncture failed, while in 14 others despite successful arterial puncture the wire could not be advanced towards the forearm part of the radial artery. In 32 cases, it was necessary to insert the 0.014” coronary guidewire due to the resistance when inserting the 0.018” (0.47 mm) standard guide despite good backflow from the needle. In 28/32 times the use of the coronary guide allowed for the effective assumption of distal access. In 21 failed cases crossover to the traditional radial approach was successfully performed. In two we performed coronary angiography with brachial access and in one case we switched from left distal to right distal access. In all 218 patients 6 Fr sheaths were used. Median procedural time was 6 min, ranging from 2 to 36 min. Detailed information on coronary procedures is listed in Table II.
Table II
Procedural characteristics of patients with successful VITRO puncture (145 LdTRA and 51 RdTRA)
Not only elective diagnostic angiographies were performed with VITRO but also urgent ad hoc PCI in subjects with unstable angina or non-ST elevation myocardial infarction (NSTEMI). Moreover, this very distal approach allowed us to perform 11 rotablations and fractional flow reserve/instantaneous flow reserve (FFR/iFR) examinations in 11 patients.
Hemostasis and complications. Hemostasis was obtained within two hours in almost all patients. No major bleeding, requiring prolonged hospital stay, surgery or transfusion, occurred. One patient on oral anticoagulation with dual antiplatelet therapy (DAPT) had conservatively managed minor forearm bleeding.
Discussion
Our experience demonstrates the feasibility of the very distal radial approach located at the functional snuffbox. The vascular approach of this access site was successful in 195 of 218 patients with a well-palpable radial pulse in the snuffbox area with a success rate of 90% and was similar to the previously reported success rate of the approach in the anatomical snuffbox [7]. However, in an additional 102 of our patients the distal pulse was not palpable or was too weak, and they underwent the traditional radial approach or other (brachial, ulnar). It suggests that in approximately two thirds of consecutive patients referred for coronary angiography the distal radial approach could be performed with a high success rate. It should be underlined that all operators participating in the current study are highly experienced in traditional radial access, and in our laboratory this access is routinely used in more than 98% of treated patients. We observed no significant learning curve of the very distal radial approach. Median time needed to obtain VITRO was 6 min (time was measured from the patient’s preparation to the first (record) loop with a recorded vascular sheath inserted into radial artery). Both left and right distal radial accesses have been reported in the literature [5, 7, 8]. In the current study the choice of site of access was made by the operator according to his and the patient’s preferences or possibility (12 of 18 dialysis patients were managed from right access due to fistula on the left forearm). Importantly, in our study the VITRO procedure was not supported by ultrasonographic assessment of the radial artery. Despite this the success rate was similar to the one reported when ultrasonography was incorporated in the protocol [5]. However, it is likely that ultrasound support could be of value in patients with a weak pulse. We used VITRO in both elective and urgent coronary artery angiography and CI. Interestingly, using this access, it was possible to perform a wide range of interventions, including not only angiography or stent implantations but also FFR and coronary rotablations. We observed no significant complications. Potential advantages of snuffbox access have been reported in previous studies [5, 7–9], and were confirmed in this study. The arm position during the intervention, especially for the left access, was comfortable for the patient and caused no significant palm motor limitations, which is of special value for right-handed patients. A potential important advantage of distal radial access is only 2 h hemostasis time, because of the superficial position of this small vessel.







