
Purpose
Intracavitary brachytherapy (ICBT) plays an important role in the treatment of cervical cancer [1]. Interstitial brachytherapy (ISBT) combined with ICBT presents a high local control rate with lower toxicity, particularly for locally advanced cervical cancer involving the parametrium or uterine body [2]. Novel hybrid applicator Venezia (Elekta, Sweden) enables IC/IS BT for locally advanced cervical cancer. In previous reports on magnetic resonance imaging (MRI)-based image-guided adaptive brachytherapy (IGABT) using Venezia applicator, the number, position, and depth of interstitial needle were determined from interim MRI preceding first BT without the applicator [3, 4]. However, MRI-based IGABT was better for delineating a large target that involves the parametrium, when compared with computed tomography (CT)-based IGABT [5, 6]. MRI-based pre-plans without applicators are insufficient because of the lack of accuracy in image fusion. Positions of the uterine body and cervix are greatly displaced depending on the presence or absence of an applicator. Moreover, interstitial needle must be set to ovoid before the applicator insertion, secondary to characteristics of Venezia applicator. Although there is a three-dimensional applicator model supplied by the vendor in the applicator libraries of the Oncentra Brachy (Elekta, Sweden) treatment planning system (TPS), the interstitial needle was not reconstructed in this model. In practice, essential interstitial needle is different for each patient due to the tumor location and volume. Unfortunately, the method to determine the optimal interstitial needle number, position, and depth while using Venezia applicator is unknown. In our experience, transrectal ultrasound-guided real-time interstitial needle insertion was challenging due to the large size of Venezia applicator. Therefore, to solve this problem, we aimed to produce a template model of Venezia applicator with whole needles, to acquire CT images, and to reconstruct the structure on TPS. Using template CT as a map helps clinicians understand the interstitial needle’s insertion route in advance. This study introduces a novel intra pre-plan method of interstitial needle optimization using template CT fusion for BT treatment of cervical cancer using Venezia applicator.
Material and methods
Applicator overview
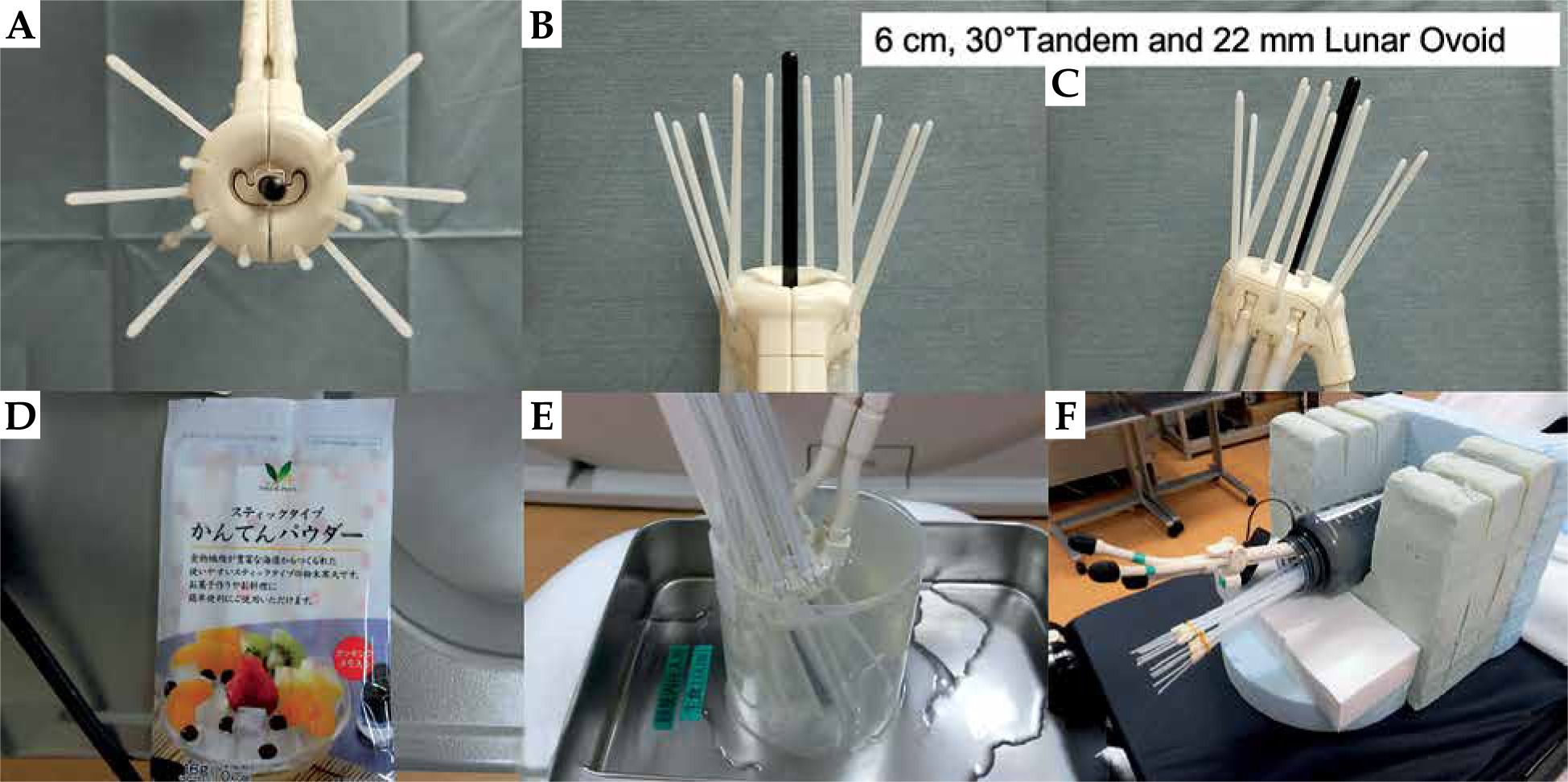
A novel Venezia applicator was designed for IC/IS BT. Venezia applicator consisted of an intra-uterine tube (tandem) and interstitial lunar ovoid tube (ovoid). Diameters of the tandem were 4 and 6 mm, but 4 mm size was easier to insert and less uncomfortable for the patient. Tandem length was from 0-3 cm to 7 cm at 1 cm intervals. For each 3-7 cm long tandem, two types of angles (15° and 30°) were available. There were three types of ovoids involved: 22, 26, and 30 mm. When two lunar ovoids were combined together and fit, they formed a ring shape. The lunar ovoid had multiple holes for the insertion of interstitial needle (22 mm ovoid had six parallel and oblique holes, while 26 and 28 mm ovoids had eight parallel and oblique holes). Additionally, a firm disposable guiding tube was required to set interstitial needle for the lunar ovoid. Clinicians could easily treat IC/IS BT by inserting an interstitial needle through the optimal hole. Owing to the structure of such an ovoid, the interstitial needle of Venezia applicator consisted of two types of needles, i.e., parallel and oblique. The oblique needles had a 20° angle with respect to the axis of applicator. Venezia applicator (6 cm, 30° tandem + 22 mm lunar ovoid) with whole needles (6F × 294 mm, ProGuide Round Needle, Elekta, Sweden) is presented in Figure 1A-C. Although parallel needle was parallel to tandem with 30° tandem, it was not parallel to tandem with 15° tandem; therefore, caution was necessary. Moreover, attention was paid to using an oblique needle secondary to its’ pathway. As presented in Figure 1A-C, the oblique needles spread far outward with respect to the tandem. Therefore, clinicians need to be careful not to damage the bladder or small intestine during deep insertion of the oblique needle. Therefore, a map demonstrating the needle insertion route was considered necessary.
Production and image acquisition of template
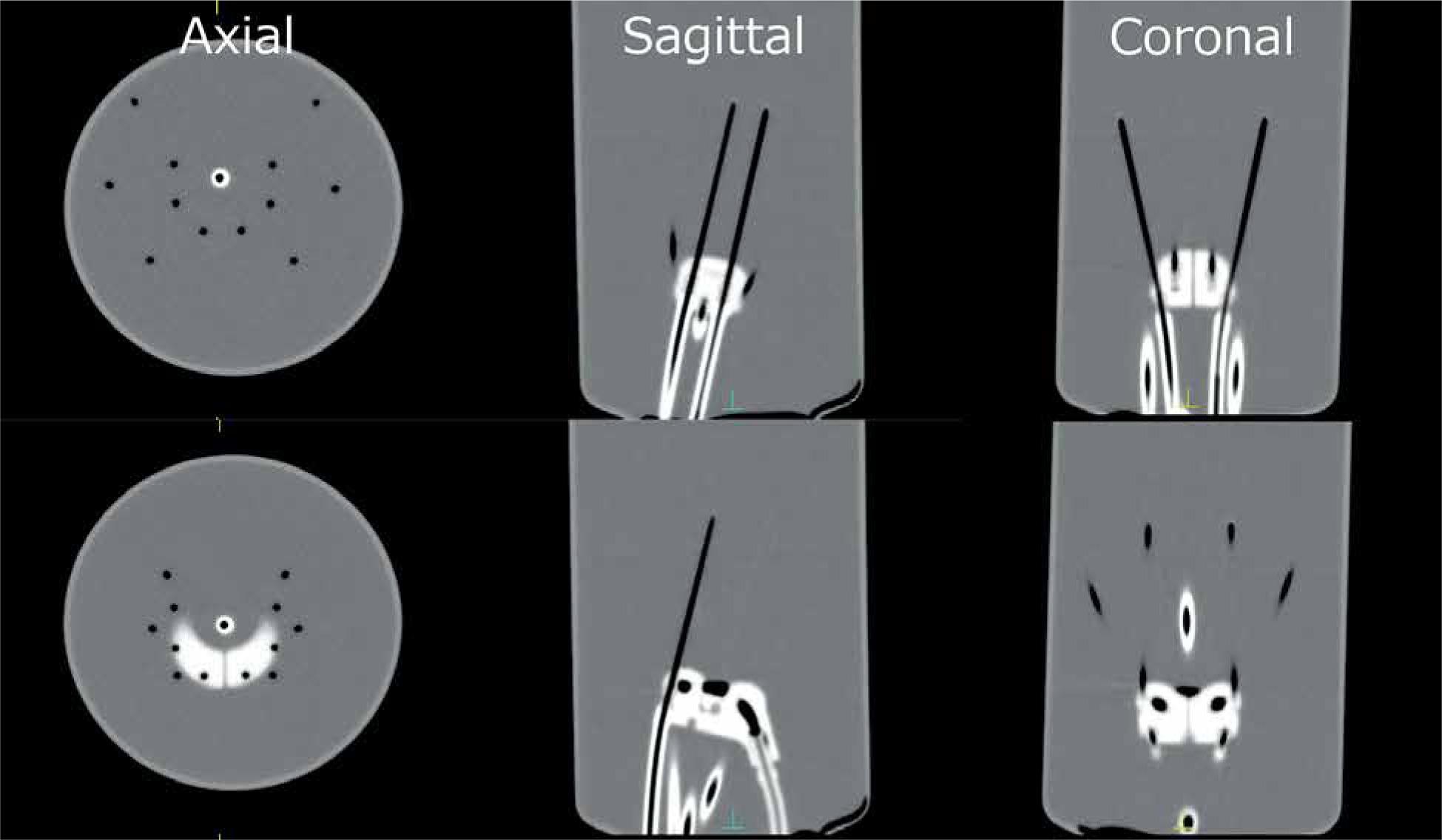
To optimize interstitial needles with Venezia applicator, initially, we conceptualized the template model with whole needles using the applicator. Whole needles (6F × 294 mm, ProGuide Round Needle) were inserted 5 cm from the tip of the ovoid in advance (Figure 1A-C). An agar was used to fill the air gaps between the applicator and needles (Figure 1D, E). We created four patterns of the template model (15° and 30° tandem each and 22 and 26 mm lunar ovoid each). The applicator was fixed horizontally to CT bed (Figure 1F). A CT scan (Aquilion, Canon Medical Systems Corporation, Japan) and three-dimensional (3D) reconstruction were obtained. Using CT imaging, the conditions included X-ray tube voltage of 120 kV, X-ray tube current of 300 mA, rotation time of 1 second, slice thickness of 1 mm, and field of view of 200 mm. Template CT images are presented in Figure 2.
Applicator and interstitial needle reconstruction on treatment planning system
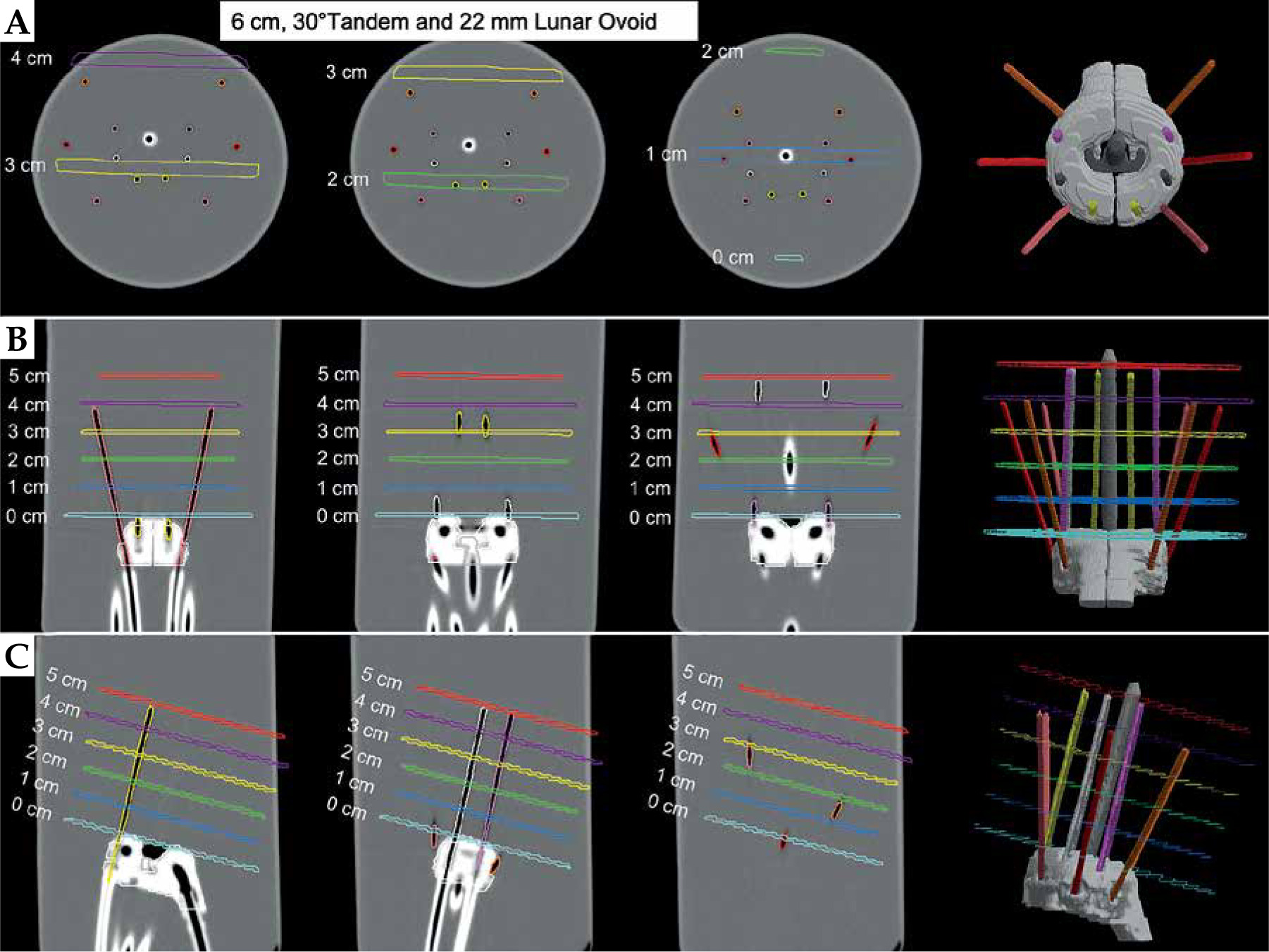
After CT image acquisition, digital imaging and communications in medicine (DICOM) CT of the template was exported to TPS (Monaco version 5.11.02, Elekta, Sweden). A radiotherapy technologist (RTT) delineated the applicator (tandem and ovoid), and whole interstitial needles on TPS. To optimize the interstitial needle depth, we created virtual depth lines as a structure (Figure 3). The tip of ovoid was the baseline of virtual lines. Virtual depth lines were set from 0 to 5 cm at 1 cm intervals. The tilt of a virtual line was set perpendicularly to the tandem. Interstitial needles and virtual lines were color-coded for easy recognition. Therefore, clinicians could establish an insertion route of the entire interstitial needle in advance using this template CT as a map.
Fig. 3
The applicator (tandem and ovoids) and whole interstitial needles are contoured on treatment planning system (TPS). A) Axial image, B) coronal image, and C) sagittal image. Virtual depth lines are created as follows: light blue – 0 cm, blue – 1 cm, light green – 2 cm, yellow – 3 cm; purple – 4 cm, and red – 5 cm from top of the ovoid
Results
Interstitial needle optimization (intra pre-plan)
After making the template CT on TPS, the actual treatment could start. We used a CT scanner, which was placed in our BT room. The patient was placed in lithotomy position, and local or systemic anesthesia was administered as usual. During this procedure, intravenous injection of pentazocine, hydroxyzine hydrochloride, and midazolam were administered for anesthesia. First, we inserted Venezia applicator (only tandem and ovoids) without any needle into the patient’s uterus and vagina. The applicator was inserted in the optimal position, and a CT scan was performed (tandem + ovoid CT). The tandem and ovoids were removed from the patient when tandem + ovoid CT was optimal.
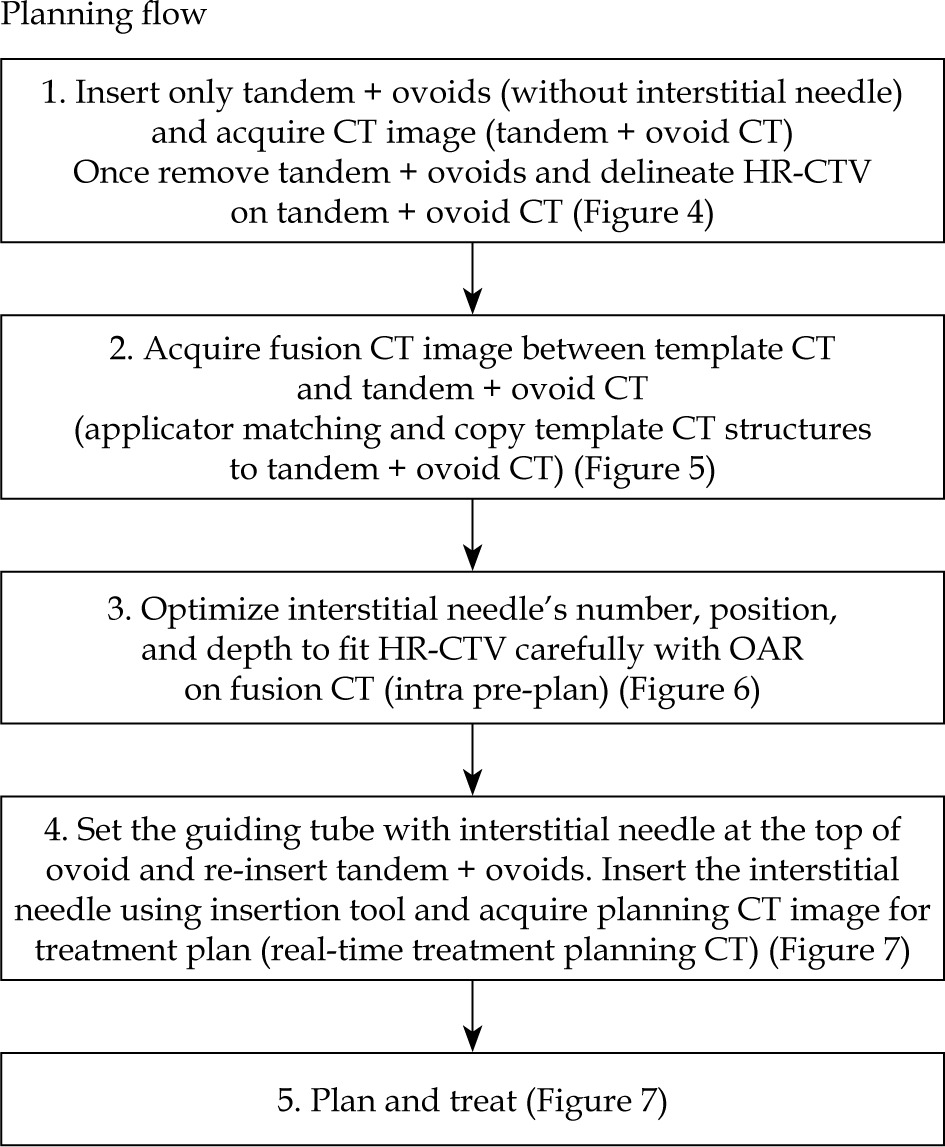
Second, we delineated high-risk-clinical target volume (HR-CTV) on tandem + ovoid CT (Figure 4). We performed image fusion between the template CT and tandem + ovoid CT (Figure 5). In particular, applicator matching between two CT images was performed, and template CT structures to tandem + ovoid CT was copied. Third, we optimized the interstitial needle’s number, position, and depth to fit HR-CTV on fusion CT, while being cautious with organs at risk (OARs) (Figure 6). Considering the fusion CT in the axial, sagittal, and coronal views, we could decide the necessary needle type and insertion depth of the needle that was optimal to cover HR-CTV. Additionally, we could understand the type of needle that was inappropriate or dangerous, secondary to the risk of damage to surrounding normal tissues (e.g., bladder and small intestine). Owing to the applicator matching, the accuracy of fusion CT was excellent. The location deviation was < 1 mm. This series of procedures was named as intra pre-plan. When the optimal needle number, position, and depth were determined, the optimized needle was set to the lunar ovoid with a guiding tube. The top of the needle was set at the top of the ovoid. Further, we re-inserted tandem and ovoids into the patient’s uterus and vagina with an interstitial needle. We inserted the optimized interstitial needle using an insertion tool of optimal depth immediately following the applicator insertion. Lastly, real-time treatment planning CT was performed, followed by planning (Figure 7). Planning flow procedures are summarized in Figure 8.
Fig. 4
Computed tomography (CT) image after insertion of Venezia applicator (only tandem + ovoid) without any interstitial needle (tandem + ovoid CT). Light blue line – HR-CTV
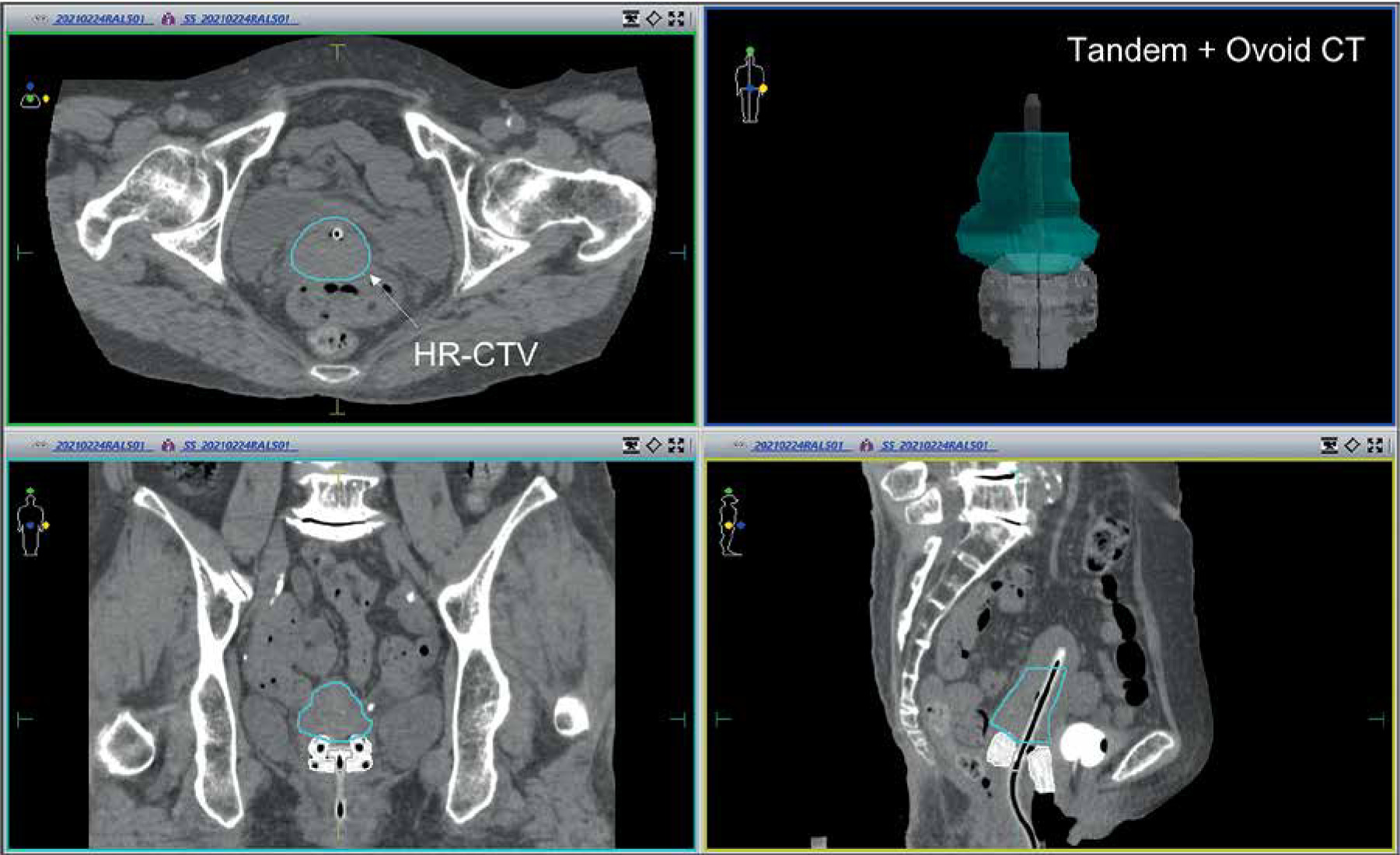
Fig. 5
Image of the production of fusion computed tomography (CT). Upper figure: template CT and lower figure: tandem + ovoid CT. Applicator matching between the two CT images is performed.
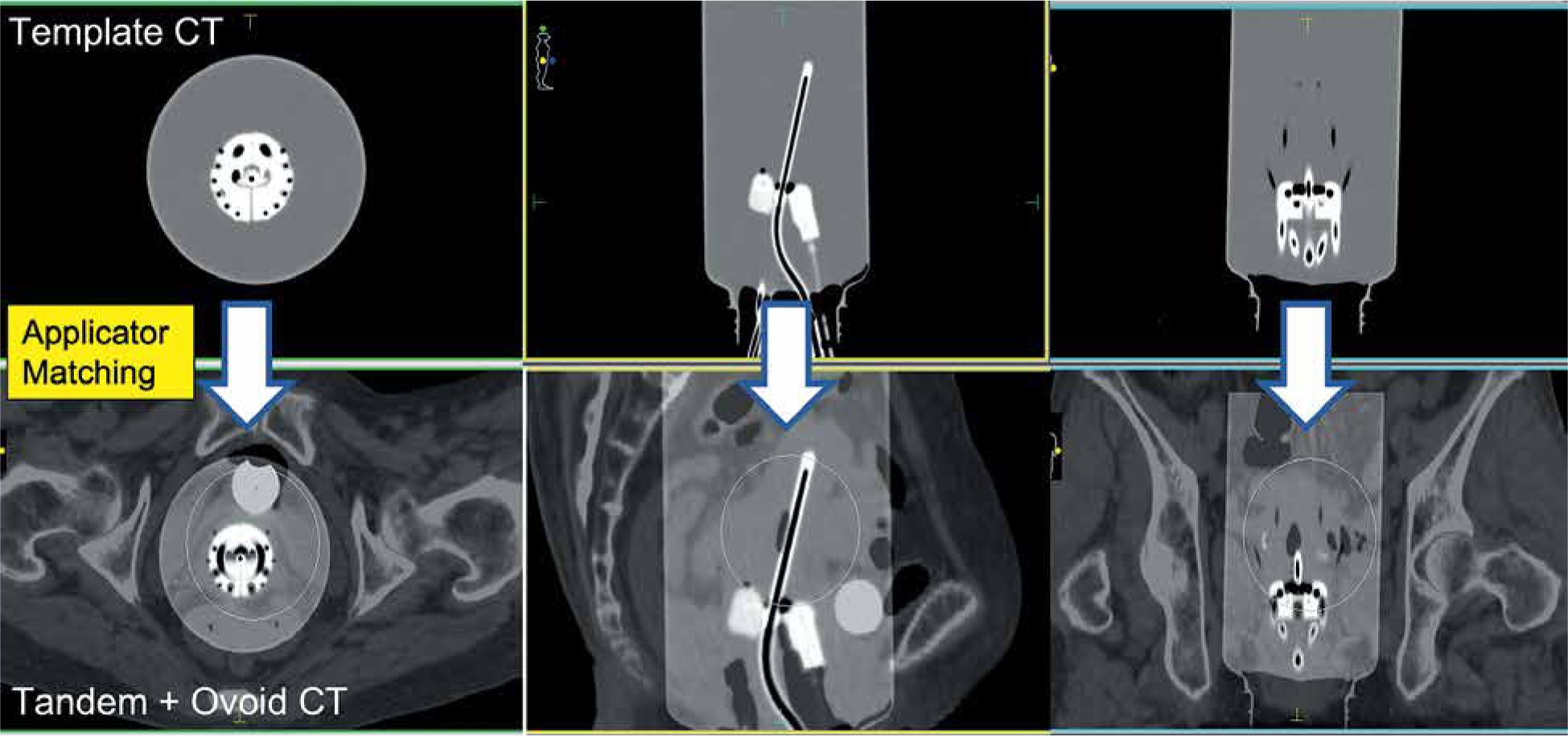
Fig. 6
Fusion computed tomography (CT) image between template CT and tandem + ovoid CT. By considering the fusion CT a map, optimization of the interstitial needle number, position, and depth can be done. For example, there are optimal interstitial needles (white arrow) and unsuitable/dangerous interstitial needles (yellow arrowhead)
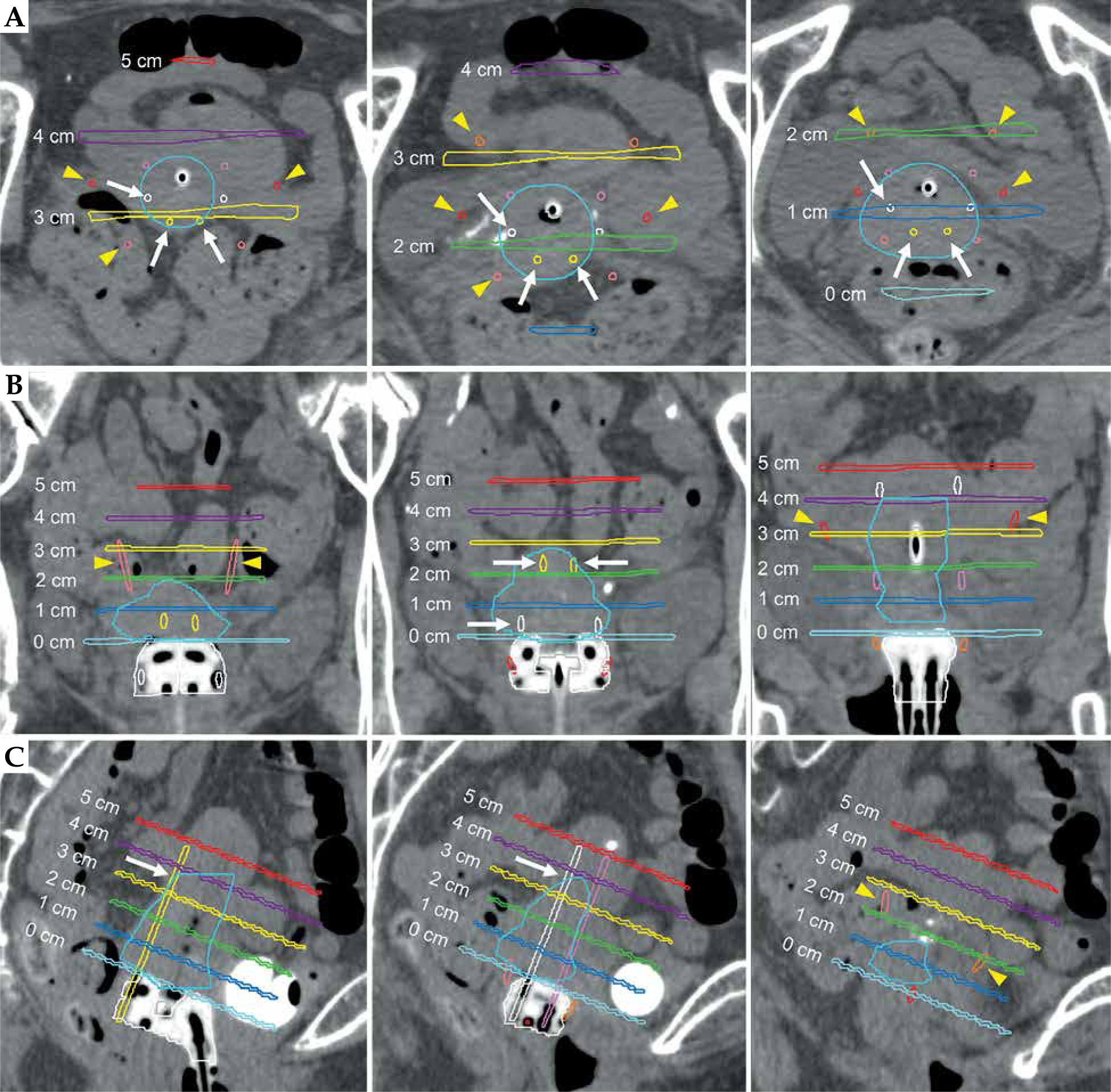
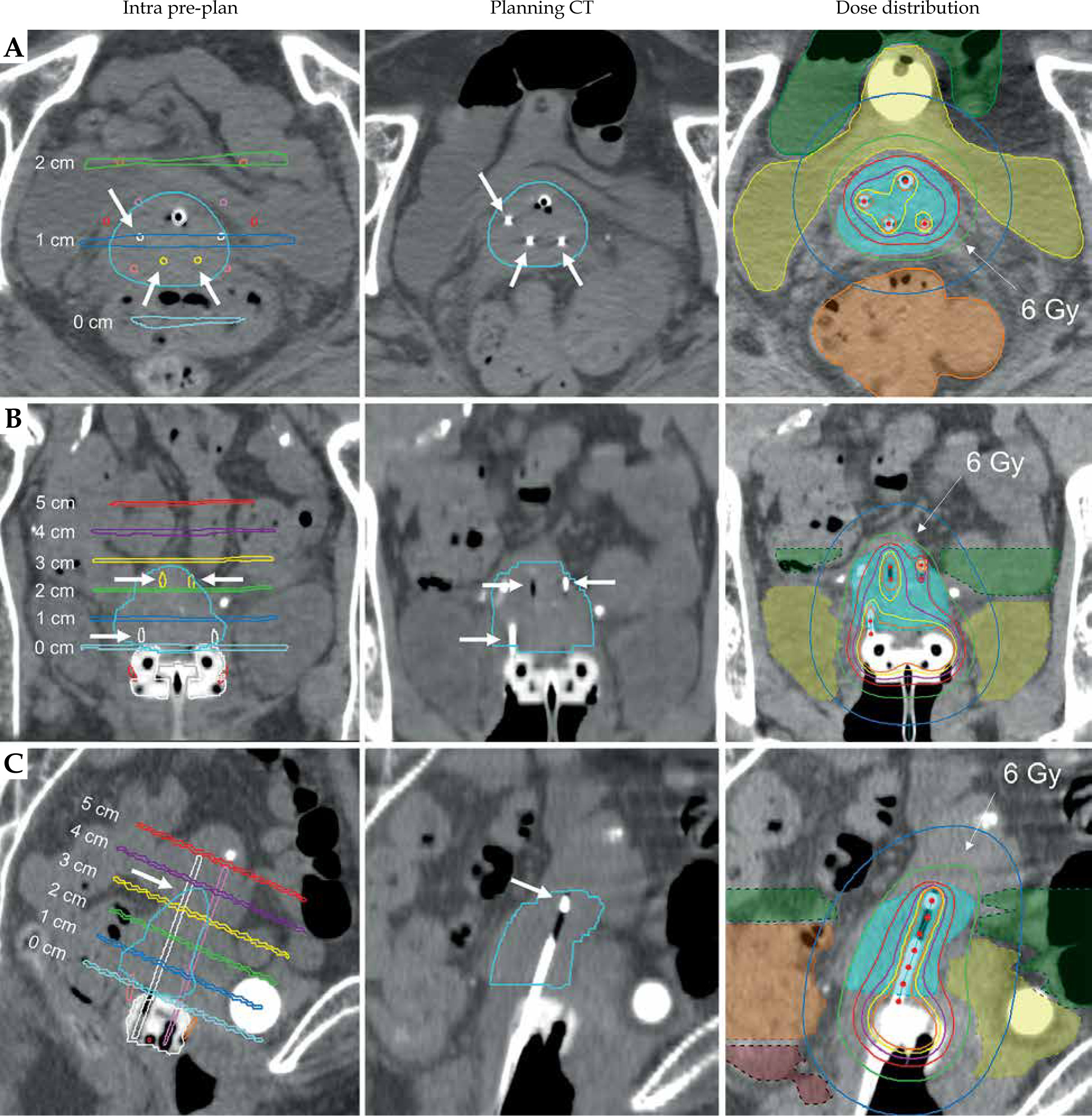
Fig. 7
Intra pre-plan, real-time treatment planning computed tomography (CT) image, and dose distribution after insertion of Venezia applicator with three optimized interstitial needles. A) Axial view, B) coronal view, and C) sagittal view. Light green line of dose distribution represents 100% isodose line (6 Gy)
Planning and treatment
After real-time treatment planning, CT was performed, and the acquired CT images were transferred to another TPS (Oncentra Brachy version 4.5.3, Elekta, Sweden). Dosimetric calculation was based on the American Association of Physicists in Medicine Task Group 43 (TG-43) report. RTT delineated the applicator, and clinicians contoured HR-CTV and OARs on real-time treatment planning CT (Figure 7). The optimized interstitial needles were also delineated. As presented in Figures 6 and 7, the inserted interstitial needles on the treatment planning CT were optimized in the number, position, and depth, all of which were optimized on fusion CT in advance. Further, clinicians could optimize dwell time with tandem, ovoids, and needles to prescribe the optimal dose for HR-CTV and OARs. Final dose distribution of the treatment planning CT is presented in Figure 7.
Discussion
Since 2005, the Groupe Européen de Curiethérapie and European Society for Radiotherapy and Oncology (GEC-ESTRO) have published a series of recommendations to promote the development of 3D-BT for cervical cancer [7-10]. The GEC-ESTRO guidelines recommend the use of MRI-based IGABT for cervical cancer. Recently, the EMBRACE-I multicenter prospective cohort study on MRI-based IGABT for cervical cancer BT was published by Pötter et al. [11]. They demonstrated an excellent 5-year local control rate (92%), and a lower late toxicity rate at a median follow-up of 51 months. In the EMBRACE-I study protocol, MRI-based treatment planning with an applicator in place was mandatory for at least first application, and subsequent applications could be CT-planned with consideration of previous MRI-based information. Therefore, although MRI-based IGABT is the standard method of 3D-BT for cervical cancer BT, CT-based IGABT still plays an important and complementary role.
A novel Venezia applicator was designed for IC/IS BT for cervical cancer. However, interstitial needle had to be set to ovoid before applicator insertion, secondary to characteristics of applicator. Additionally, the use of interim MRI preceding first BT for pre-planning of interstitial needle optimization without an applicator was insufficient due to lack of accuracy in image fusion. Therefore, we produced a template CT of Venezia applicator with whole needles and used it as a map. As presented in this study, the intra pre-plan method demonstrated an excellent reproducibility of the interstitial needle optimization treated with Venezia applicator of IC/IS brachytherapy for cervical cancer. The most important step in this procedure was tandem + ovoid CT. Since the Venezia applicator’s tandem and ovoids had a fixed form that could be combined by performing applicator matching, fusion CT presented a high accuracy of consistency between template CT and tandem + ovoid CT (Figures 5-7).
This novel intra pre-plan method demonstrated several advantages. First, clinicians need not to worry about interstitial needle optimization on interim MRI preceding first BT without an applicator. Furthermore, they can establish an optimal interstitial needle position and depth in advance, to which an accurate and safe secondary insertion is achievable. Therefore, clinicians can achieve the best performance of Venezia applicator using intra pre-plan, and even those with limited experience in IC/IS BT can perform simple, safe, and accurate IC/IS BT. Second, once the template CT is produced, it can be adopted for other patients who need the Venezia applicator BT. Therefore, the intra pre-plan method using a template CT has great versatility. Moreover, we believe that our intra pre-plan method can be applied to Venezia applicator and Geneva’s latest applicator (Elekta, Sweden). Third, optimizing interstitial needle placement in advance reduces the insertion of unnecessary needles, making it less invasive for the patient and more cost-effective.
This study has some limitations. First, we could not compare the intra pre-plan method with a standard method for needle optimization and dose distribution. Ideally, a randomized trial would be required for the evaluation of clinical outcomes; however, this might be impossible. Even if clinicians do not use our intra pre-plan method, they might administer IC/IS BT using Venezia applicator with optimized interstitial needle. However, the standard method, especially for clinicians with limited experience in the field of IC/IS BT would take more time for interstitial needle optimization than our method. Next, this technique is CT-based IGABT. As stated before, the GEC-ESTRO recommends the usage of MRI-based IGABT for gynecological brachytherapy. Although the same template model using MRI is available, in practice, it is often difficult to perform multiple MRI scans by inserting and removing the applicator in the same fashion. Therefore, the present technique is more suitable for CT-based IGABT than MRI-based IGABT. Grover et al. reported a survey of the American Brachytherapy Society for image-guided cervical BT in 2014 [12], and Toita et al. reported a national survey of ICBT for cervical cancer in Japan [13]. In their study, CT was used for 95% and 60% of the treatment planning in the U.S. and Japan, respectively. Additionally, in the consensus guidelines for delineation of clinical target volume for IGABT in cervical cancer, although MRI is superior for delineation of parametrial extension, CT is sufficient for delineation of the target [6]. Therefore, although MRI is the standard modality of IGABT for cervical cancer BT, our intra pre-plan method would be helpful for CT-based IGABT treatment of cervical cancer using Venezia applicator. However, if there is no CT scanner in BT room, the administration of our method could be slightly difficult. Third, at least two CT scans are performed with this technique because of the necessity of tandem + ovoid CT and real-time treatment planning CT. Although ideally, at least these two CT scans would be needed in every BT session, at least only one-time procedure of this technique could give clinicians sufficient information on the needle optimization. Then, there is a potential to omit the second or later procedure of this technique. However, our technique may have a higher radiation exposure than MRI-based and standard CT-based IGABTs. Finally, using our procedure, overall treatment time during brachytherapy is slightly longer than during the standard procedure. However, with optimal anesthesia, the patient’s uncomfortable symptoms during this procedure are well-tolerated.
Conclusions
We introduced a novel intra pre-plan method of interstitial needle optimization using template CT fusion for BT treatment of cervical cancer using Venezia applicator.
To use this CT-based intra pre-plan method, we believe that the interstitial needle optimization of Venezia applicator would be safer, more effective, and cost-effective.








