
Purpose
Prostate cancer penile metastases are rare, with less than 500 cases described in the literature [1]. They represent less than 0.5% of metastatic localizations of prostatic adenocarcinoma with more frequent clinical manifestations described as painless nodules of the glans or corpus cavernosum or malignant priapism [1-4]. Given the often poor prognosis of these tumors, the therapeutic strategy is essentially oriented towards organ preservation and improved quality of life [5].
Since the last decade, the concept of ablative treatment of an oligometastatic prostate cancer has gained popularity based on encouraging clinical results [6].
We present a case report of a penile oligometastasis of a prostatic adenocarcinoma treated with ablative high-dose rate brachytherapy.
Patient and disease history
In October 2013, a 54-year-old patient underwent radical prostatectomy for high-risk prostate cancer – pT3b, pN0, R1, Gleason score 8 (4 + 4). While post-operative prostate-specific antigen (PSA) was 0.71 ng/ml, an adjuvant radiation therapy delivering a total dose of 66 Gy in 33 fractions to the anastomosis, combined with short androgen deprivation therapy (ADT) using Degarelix 120 mg (6 months), was proposed.
In September 2017, a rise in PSA (PSA = 0.31 ng/ml) without evidence of local relapse or distant metastasis led to consideration of intermittent ADT.
In January 2019 (PSA = 0.04 ng/ml), a palpable nodule (30 mm × 12 mm) located on the left dorsolateral side of the penis was observed on MRI, potentially evocative of Lapeyronie disease.
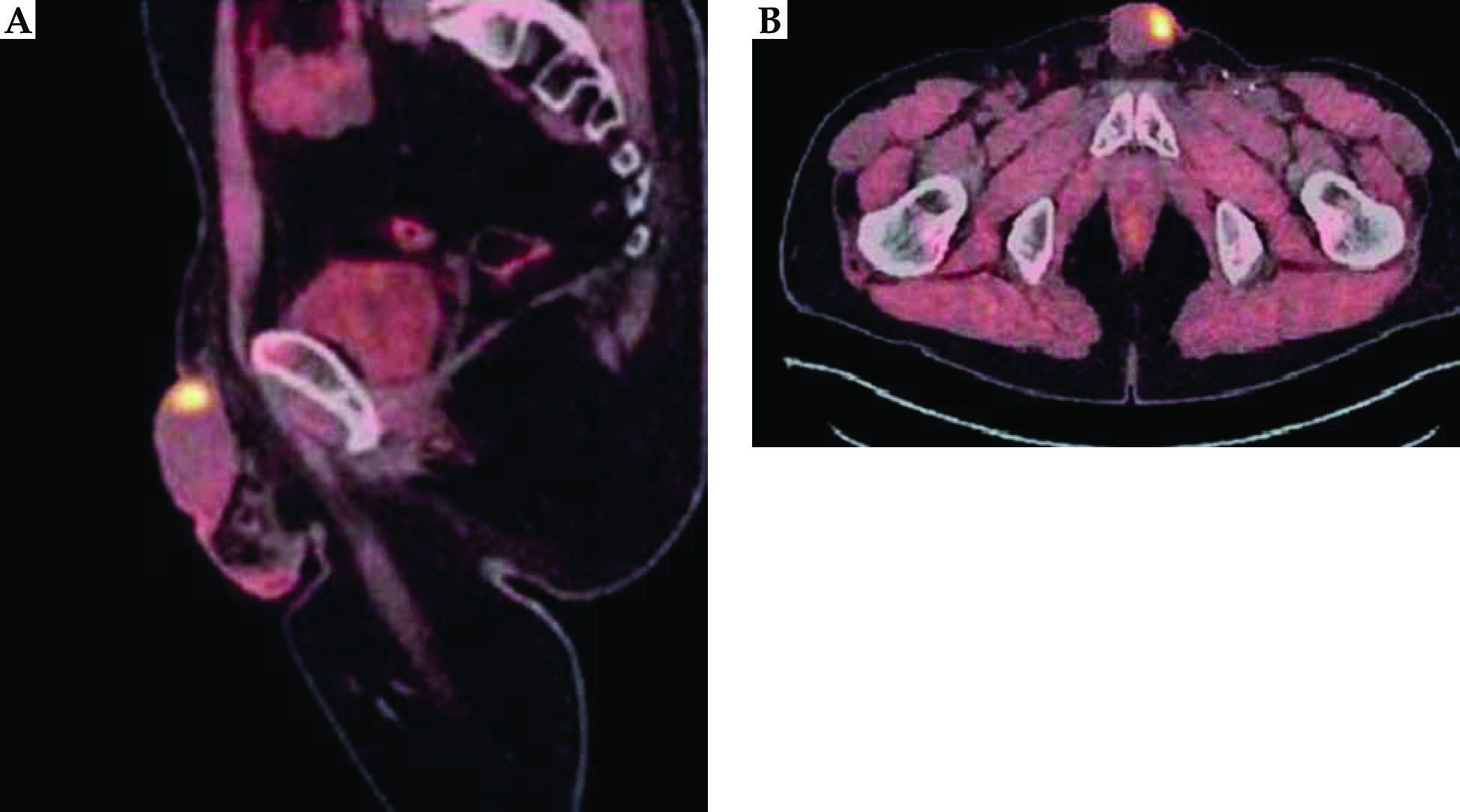
In May 2020, the PSA reached 1.57 ng/ml. Positron emission tomography (PET) using 18F-fluoro-choline showed a hypermetabolic focus on the left dorsolateral side of the penis and biopsies established the diagnosis of prostate cancer penile metastasis (Figure 1). The 68Ga-PSMA-11-PET confirmed not only this hypothesis but also the absence of other distant disease.
In October 2020, the by then 61-year-old patient was referred to the Radiation Therapy Department of Antoine Lacassagne Cancer Center.
In this context of a single prostatic adenocarcinoma penile metastasis, we discussed, with the patient, either palliative continuous ADT or metastasis-directed therapy (MDT) based on total penectomy or brachytherapy, as part of a conservative treatment. The patient opted for the organ preservation ablative procedure.
Brachytherapy procedure
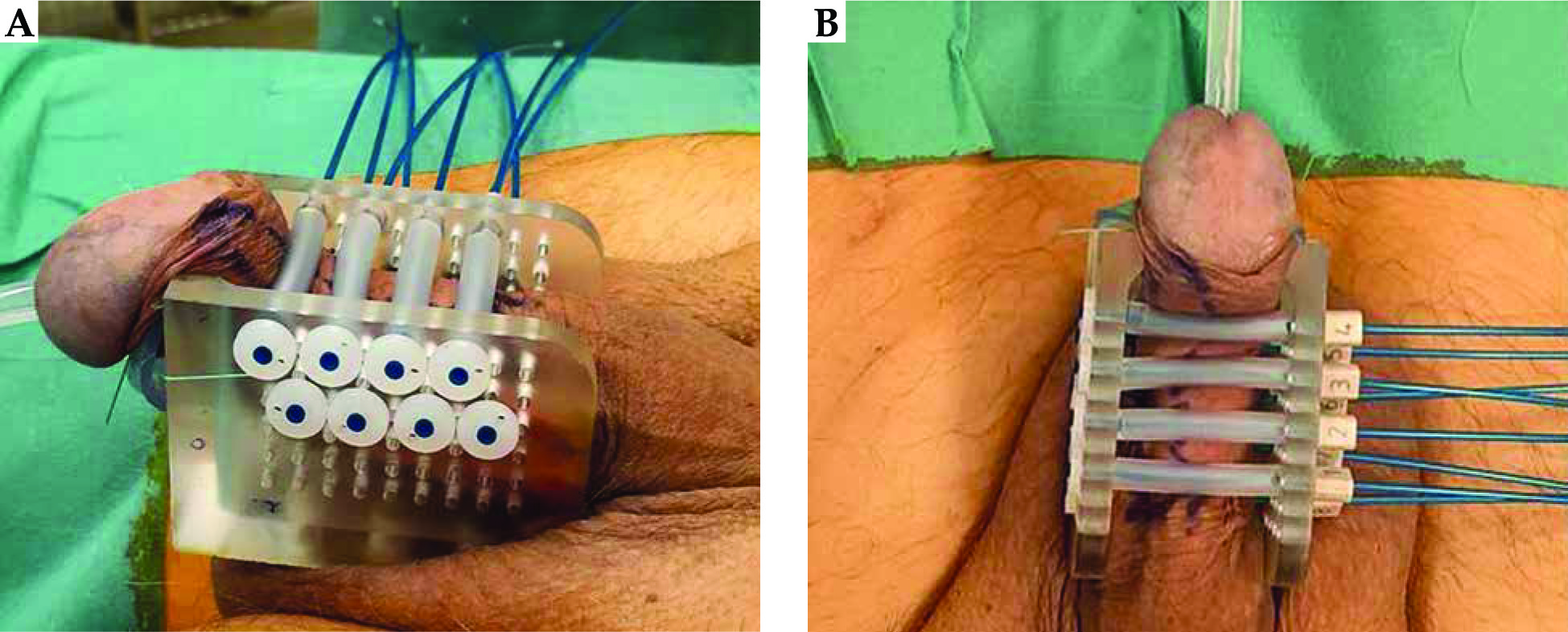
The patient was treated with multicatheter interstitial high-dose rate brachytherapy (MHB). After urethral catheterization, the penis was placed in an applicator with two parallel templates comprising 10 mm spaced holes in all directions. Eight needles were implanted in 2 planes through the templates, providing for the insertion of plastic catheters through the entire volume of the tumor (Flexible Catheter Leade Eckert and Ziegler BEBIG company, Berlin, Germany) (Figure 2).
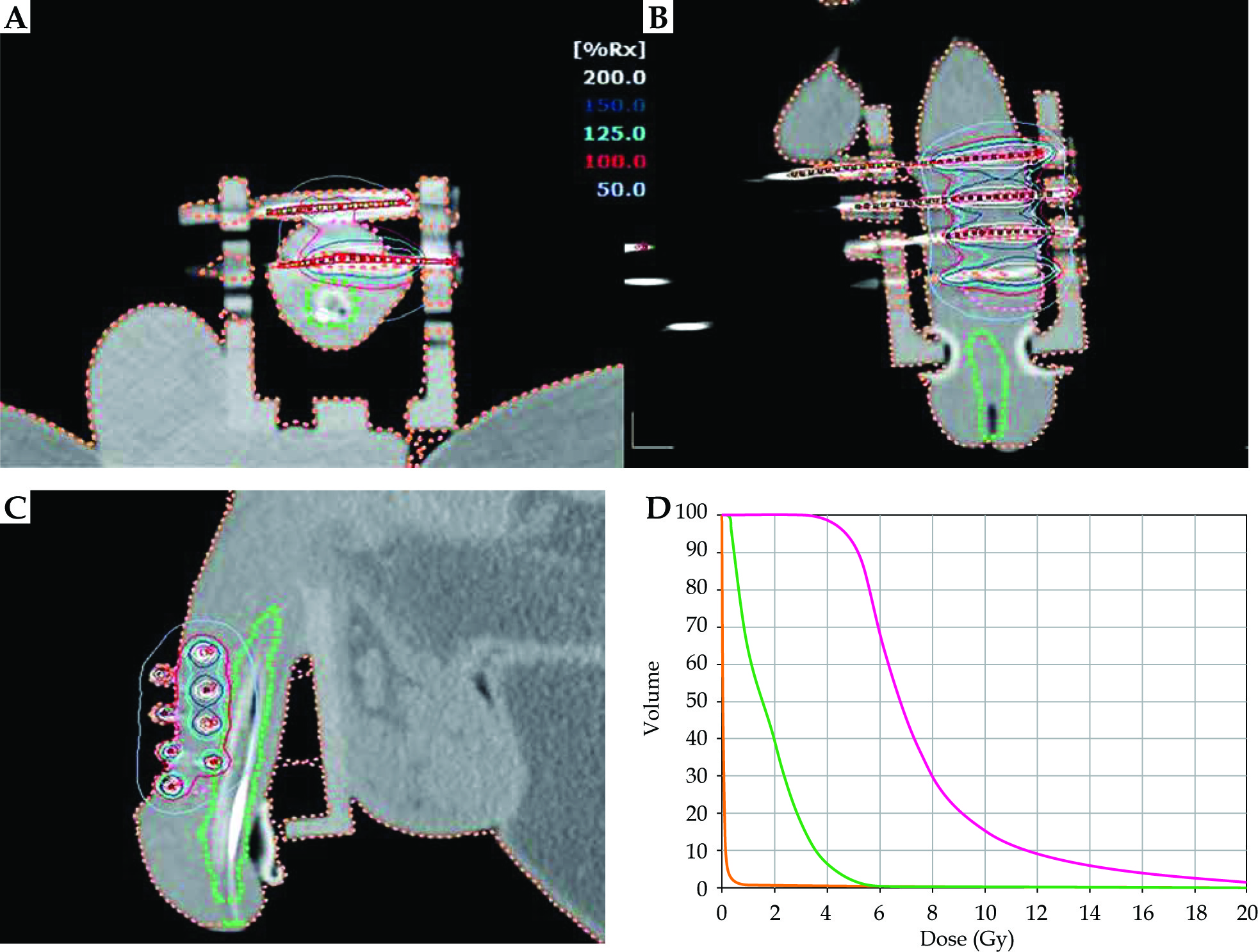
After the patient recovered from the anesthesia, a planning computed tomography (CT) scan without iodine injection was performed for dose distribution analysis and optimization purposes. The prescribed dose was 36.4 Gy in 7 fractions of 5.2 Gy each, over 4 consecutive days. The equivalent doses at 2 Gy for αβ = 1.5 (EQD2αβ1.5 for tumor tissue), for αβ = 3 (EQD2αβ3 for urethra), and for αβ = 10 (EQD2αβ10 for skin) were calculated. The optimization of the dose distribution on clinical target volume (CTV) and urethra was manually achieved with graphical optimization (SagiPlan 2.0, Eckert and Ziegler BEBIG Company, Berlin, Germany). The dose constraints used have already been reported [7]. For CTV, the treatment objectives, namely V100% (volume receiving 100% of the prescribed dose) > 90% of the prescribed dose, V150% (volume receiving 150% of the prescribed dose) < 35% of the prescribed dose, were respected. Confluence of two V200% isodoses (volume receiving 200% of the prescribed dose) and V200% diameter > 10 mm were avoided. Dose constraints for the urethra were V115% < 1% (urethra volume receiving 115% of the prescribed dose should be less than 1% of the urethra volume). D10u (dose delivered to 10% of the urethral volume), D30u (dose delivered to 30% of the urethral volume) and DNR (dose non-homogeneity ratio) were also reported. Treatment characteristics are reported in Table 1 and MHB treatment planning is presented in Figure 3.
Table 1
Treatment characteristics
| Dosimetric data | # | |
|---|---|---|
| CTV (cc) | 6.9 | |
| D90 (%) | 99.5 | |
| V100 (%) | 89.6 | |
| V150 (%) | 32.8 | |
| V200 (%) | 13.7 | |
| DNR | 0.365 | |
| EQD2 | ||
| αβ1.5 (Gy) | 68.7 | |
| αβ3 (Gy) | 59.7 | |
| αβ10 (Gy) | 46.1 | |
| Urethra | ||
| D0.1cc (%) | 101.6 | |
| D1cc (%) | 62.9 | |
| D10u (%) | 69.0 | |
| D30u (%) | 45.7 | |
[i] CTV – clinical target volume, D90 – dose delivered to 90% of CTV expressed in percentage of the prescribed dose, V100 – CTV receiving 100% of the prescribed dose expressed in percentage, V150 – CTV receiving 150% of the prescribed dose expressed in percentage, V200 – CTV receiving 200% of the prescribed dose expressed in percentage, DNR – dose non-homogeneity ratio = 1 – [V100 – V150]/V100, EQD2αβ1.5 – equivalent dose in 2 Gy fractions for tumor tissue, EQD2αβ3 – equivalent dose in 2 Gy fractions for urethra, EQD2αβ10 – equivalent dose in 2 Gy fractions for skin, D0.1cc – dose delivered to 0.1 cc of the urethral volume, D1cc – dose delivered to 1 cc of the urethral volume, D10u – dose delivered to 10% of the urethral volume, D30u – dose delivered to 30% of the urethral volume
The first fraction was delivered on the day of the implant and the remaining dose was delivered twice daily, 6 hours apart (Saginova, Eckert and Ziegler BEBIG company, Berlin, Germany) [8]. The overall treatment was well tolerated with painless removal of the catheters and rapid normalization of urinary function.
At the six-month follow-up, clinical examination confirmed a complete response of the penile tumor without any inguinal lymph node involvement. In terms of side effects, urinary function was normal (IPSS 2) while a G1 dyschromia was observed in regard to the treated area (Figure 4). The new 68Ga-PSMA-11-PET confirmed the absence of hypermetabolism in the initial penile tumor area as well as at a distance. Assuming that the single Degarelix injection was done in September 2020, blood tests were in line with clinical and imaging results with PSA = 0.19 ng/ml and testosterone = 435 ng/dl (N > 175).

Discussion
Interstitial brachytherapy is a technique of choice, and is a strong recommendation for treatment of penile carcinoma at stage T1a, T1b and T2 [9].
In the largest series of high-dose brachytherapy (HDB) for penile carcinoma, Kellas-Ślęczka et al. analyzed 76 patients treated with HDB (42.8 Gy or 48.2 Gy for adjuvant or definitive treatments, respectively). They observed a five-year local-relapse-free survival rate (LRFS) of 66%, with a penis preservation rate of 67% [10]. Recently, in our study [11] on 29 patients treated with multicatheter interstitial high-dose-rate brachytherapy (MHB), we found that the five-year LRFS rate was 82%. In our series, 93% of patients had radiodermatitis (grade 2: 83%). Regarding late toxicities, the most serious complication is necrosis, which varies from 0 to 26% in the literature.
Prostate cancer penile metastasis is generally associated with a poor prognosis; half of the patients die during the year after diagnosis [12]. De Luca et al. [13] reported that the most common primary tumors are prostate (33%) and bladder cancers (30%).
Different mechanisms for prostate cancer metastasis to the penis include direct invasion, implantation from prior instrumentation, retrograde venous flow, and arterial or lymphatic dissemination [14]. In the case of symptomatic penile metastasis, treatment options vary, depending on disease burden. Therapeutic options can be based on radiation therapy, chemotherapy, or ADT, while partial or total penectomy is indicated for patients with priapism or uncontrollable pain [15].
In the past decade, the concept of “oligometastasis” for patients diagnosed with a limited number of prostate cancer metastases, generally defined as less than five lesions, has shown a better prognosis compared to patients with extensive metastatic disease [5]. The distinction between recurrent or de novo metastatic disease may also be important because of their different biological and clinical characteristics [16, 17]. The main goal of the oligometastasis recurrence concept is to postpone palliative ADT prescription, with its negative impact on quality of life and risk of metabolic syndrome. This objective can be achieved with different ablative treatments such as metastasectomy, stereotactic body radiation therapy (SBRT) and brachytherapy. The Ost et al. STOMP trial was the first randomized study to assess the possibility of deferring palliative ADT with MDT (metastasectomy or SBRT) in an oligometastatic prostate cancer recurrence population [18]. In the MDT group, a total dose of 30 Gy (80% of the maximal dose) was delivered in three fractions. Patients showed a longer ADT-free survival and a decrease of PSA in the MDT group v. surveillance. No significant toxicity grade ≥ 2 in the MDT group was observed [19]. The first randomized trial demonstrating the impact of ablative therapy on a primary end point of overall survival (OS), in patients with oligometastases, is the SABR-COMET trial [20]. In this study including multiple histologies, Palma et al. noted an absolute benefit of 24.6% at 5 years in favor of ablative therapy.
In radiotherapy settings, brachytherapy offers a more favorable dose distribution compared to external beam radiotherapy, due to rapid dose fall-off and the ability to spare fragile normal tissues. Furthermore, brachytherapy provides for repeat repositioning, compared to SBRT, in the case of prostate cancer penile metastases.
We reported the first prostate cancer penile metastasis managed by interstitial high-dose rate brachytherapy.








