
Purpose
Brachytherapy is a critical component of the treatment of cervical cancer. It is a technique for delivering radiation, in which the source of radiation is placed close to the tumor site [1]. Brachytherapy is used in conjunction with external beam radiotherapy (EBRT) to maximize the curative dose. Cisplatin is typically the drug of choice when used as a radiosensitizer at a dose of 30-40 mg weekly [1, 2]. Even though brachytherapy is used in a variety of cancer sites, it is the gold standard in the treatment of locally advanced cervical cancer.
Numerous obstacles exist in the provision of radiotherapy services in general, and particularly brachytherapy, in low- and middle-income countries. Technical challenges include a lack of reliable electricity, a dearth of local expertise for maintenance, and a lack of manpower with technical expertise necessary to operate the equipment [3]. However, non-technical obstacles, including a lack of political will, insufficient funding, and competing healthcare needs, such as human immunodeficiency virus, malaria, tuberculosis, and other neglected tropical diseases, exist [4].
Sub-Saharan Africa encompasses all of Africa’s territory South of the Sahara Desert. It spans across Southern, Central, Eastern, and Western Africa. Sub-Saharan Africa is home to 19 of 20 countries, with the highest cervical cancer prevalence, with sub-Saharan Africa having the highest global burden [5]. Additionally, this region lacks adequate coverage of the human papillomavirus vaccine, cervical cancer screening, and access to high-quality treatment. Currently, the majority of countries in sub-Saharan Africa lack radiotherapy facilities, resulting in treatment delays, while others must travel across borders to neighboring countries to access radiotherapy services [6-8]. The few countries that offer radiotherapy or brachytherapy face lengthy wait times for services. According to recent reports, Africa accounts for only 3% of global brachytherapy units. This is sadly insufficient to achieve the 2030 goal of eradication [9].
While World Health Organization (WHO)’s goal of eliminating cervical cancer by 2030 through a triple intervention strategy is welcome news for Africa, particularly sub-Saharan Africa, procedures of providing brachytherapy services to treat 90% of invasive cases are enormous [10].
The aim of the present study was to discover how many brachytherapy units are available and where they can be found in Africa.
Material and methods
Data sources and extraction
The GLOBOCAN 2018 database, which is presented by the International Agency for Cancer Research (IARC), was used to extract data on cervical cancer. It is an online database that provides a global estimate of cancer incidence and mortality for 36 different cancer types in 185 countries. Number of new cervical cancer cases, ranking of cervical cancer incidence and mortality, and country population estimates are among the variables collected. For the 54 African countries, data was gathered.
We chose cervical cancer as our focus because brachytherapy is a key part of the standard of care for its’ treatment, and it is the biggest cause of cancer-related deaths in Africa. Cervical cancer was just named the first cancer to be targeted for worldwide eradication.
Directory of Radiotherapy Centers (DIRAC) yielded information about radiotherapy centers, megavoltage devices, and brachytherapy units. Since 1959, the International Atomic Energy Agency (IAEA) has hosted DIRAC, the world’s most comprehensive database on radiation resources. It has records of radiation infrastructure from 141 nations, both present and historical. However, data is only available for 30 of 54 Africa’s countries (Figure 1).
Fig. 1
Brachytherapy availability in Africa. Varying shades of green show the availability and density of brachytherapy units in countries where they are available. Blue color shows where there are no brachytherapy units

For the analysis, the total number of brachytherapy units was included, regardless of type (high-dose-rate or low-dose-rate) or functional state.
Estimation of the number of brachytherapy units available
Cervical cancer incidence and total number of brachytherapy units vary significantly across the continent, with the former being significantly higher than the latter. Therefore, to ensure comparability across nations, we estimated the availability of brachytherapy units across the continent by calculating the number of brachytherapy units per 1,000 cases of cervical cancer using the formula below.
Statistical analysis
On November 4, 2020, DIRAC data was accessed, entered into Microsoft Excel version 2016, cleaned, and exported to IBM SPSS version 25 for analysis. Number of new cases of cervical cancer, ranking of new cases, rating of mortality, country, and population of the country were the variables. Descriptive statistics were used to analyze the data. These were presented as frequencies and proportions. Color-coded maps were used to depict continental distribution of brachytherapy units.
Results
There are 243 radiotherapy centers in 30 of 54 Africa’s countries, with 83% (202/243) of these centers located in the North and South of Africa. However, not all of these radiotherapy centers have brachytherapy equipment accompany the existing external beam units that they already have.
In 20 of the 54 African countries, there are 101 brachytherapy units. This equates to 3% (101/3,375) of the total worldwide units. Of these, 68% (69/101) are high-dose-rate (HDR) units, 21% (21/101) low-dose-rate (LDR) units, and 11% (11/101) units that are not specified (N.S.) (Table 1).
Table 1
Availability of radiotherapy centers and radiotherapy facilities in Africa according to IAEA’s Directory of Radiotherapy Centers (DIRAC), November, 20, 2020
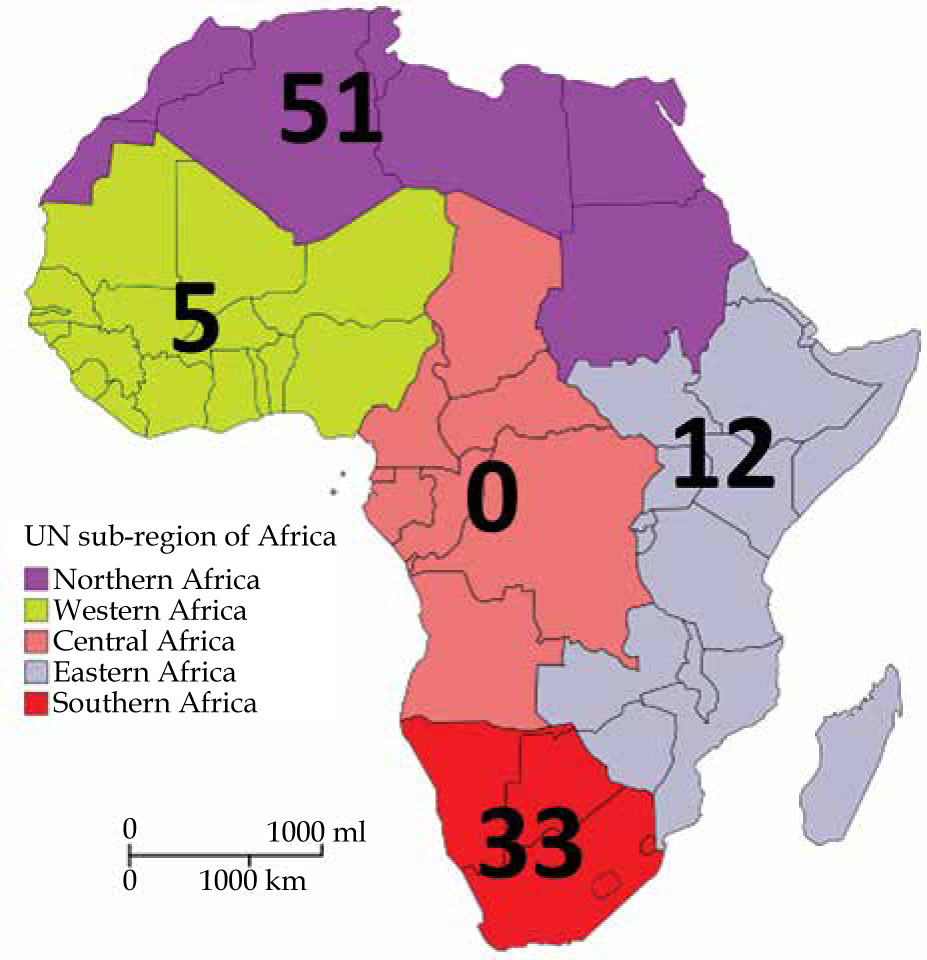
The DIRAC statistics did not include information regarding radioisotopes utilized; however, a review of the literature revealed that all three of the most regularly used radioisotopes for brachytherapy are available on the continent (Table 2). North Africa is home to half of all brachytherapy units (51/101), while the Central African region lacks such a facility (Figure 2). South Africa has the highest absolute number of brachytherapy units on the continent, accounting for 24% (24/101) of all units (Table 1). Egypt has the most brachytherapy units available (23.7 per 1,000 new cases), whereas Nigeria has the largest deficit of brachytherapy units (0.13 per 1,000 new cases).
Table 2
Types of brachytherapy sources available in 11 out of 20 African countries from published articles
| Country | Brachytherapy source | Reference | |
|---|---|---|---|
| 1 | Uganda | 137Cs | Kavuma et al., 2021 [17] |
| 2 | Nigeria | 60Co | Ntekim et al., 2010 [21] |
| 3 | Sudan | 60Co | Christ et al., 2021 [18] |
| 4 | Tanzania | 60Co | Suleiman et al., 2019 [19] |
| 5 | Zambia | 192Ir | Lombess et al., 2020 [22] |
| 6 | Botswana | 192Ir | Clayman, 2015 [23] |
| 7 | Ghana | 60Co, 137Cs | Scott et al., 2021 [24] |
| 8 | Zimbabwe | 60Co | Chibonda et al., 2021 [15] |
| 9 | Kenya | 192Ir | Ndonye, 2018 [20] |
| 10 | Egypt | 60Co | Hegazy et al., 2020 [16] |
| 11 | South Africa | 192Ir | Minnaar et al., 2021 [25] |
We looked at nations with at least one brachytherapy unit per 1,000 new cases of cervical cancer to obtain an estimate of the extent of availability. Only 11 of the 20 nations have more than one brachytherapy unit per 1,000 new cervical cancer cases (Table 1).
Cervical cancer is the first or second most common cancer diagnosed in 87% of countries (47 out of 54), and the first or second leading cause of cancer mortality in 89% of countries (48 out of 54). Nigeria, the continent’s most populated country and has the highest absolute number of cervical cancer cases, accounting for 12.5% (14,943/119,284) of all cases. Some countries with only a single-unit of brachytherapy have a higher number of units per 1,000 new cases, because the country has a low number of cervical cases. For example, Mauritius has only one brachytherapy unit and only 120 occurrences of cervical cancer, whereas South Africa has 24 units per 1,000 cases (Table 1).
Discussion
Current availability of brachytherapy infrastructure and capacity for cervical cancer treatment
The WHO’s current recommendations for worldwide cervical cancer eradication are based on a triple intervention, with targets of 90% vaccination of girls before the age of 15, 70% screening of eligible women, and 90% treatment of all pre-malignant lesions and malignancy [10]. These techniques would have the greatest impact if all interventions ware applied concurrently [10]. Our study confirms the findings of previous evaluations that Africa’s current capacity for brachytherapy is regrettably inadequate, and demand for brachytherapy services will continue to grow unless urgent measures are implemented to bridge brachytherapy infrastructure [7, 11]. While significant improvements have been made in the last decade, they have been insufficient to keep pace with the continent’s rising cancer rates [9, 12, 13]. The majority of low- and middle-income nations lack the necessary infrastructure for radiotherapy. Only 20 of the 30 countries with external beam radiotherapy facilities have complementing brachytherapy facilities, and the Central African region lacks even a single-unit, implying that women with cervical cancer lack access to effective treatment. According to a recent study, two-thirds of women diagnosed with cervical cancer do not receive early and adequate treatment, and only around 22% receive treatment with the purpose of curing the disease [14].
Throughout the continent, in recent years, there has been a continuous movement from LDR to HDR brachytherapy delivery. Currently, in numerous nations, including Nigeria, Ghana, Zimbabwe, and Botswana [15-17], HDR afterloaders are used (Table 2). Although there is no evidence to suggest that LDL and HDL techniques have any impact on clinical outcomes [18], HDR has the advantage of reducing staff’s and patient’s radiation exposure and can treat more patients each week than LDR [19]. One advantage of LDR is that the radioisotope generally utilized is cesium-137, which has a 30-year half-life. This decreases the frequency, cost, and logistical complexity associated with source replacement. On the other hand, the HDR sources (iridium-192 has a half-life of 74 days, and cobalt-60 has a half-life of 5.3 years) have a shorter half-life, and hence require regular replacement. This presents significant logistical and regulatory issues for countries, which use these radioisotopes [15-25].
Challenges to the quest for the elimination of cervical cancer in Africa
To eliminate cervical cancer in Africa, a comprehensive and integrated cancer care infrastructure across the cancer care continuum is required. Cancer prevention includes health education, promotion, and vaccination as well as cancer screening, diagnosis, and treatment (including surgery, radiotherapy, and systemic therapy) [4]. In Africa, the provision of radiotherapy facilities in general, and brachytherapy facilities in particular, faces plenty of challenges, ranging from professional training to equipment procurement, and maintenance to a lack of electricity, respectively. Overcoming these obstacles would necessitate strong political will on the part of African governments as well as strong technical support from the world’s cancer community [10].
Capital and human resources
While research indicate that providing radiation is cost-effective and generates economic and societal returns on investment, the logistics and cost of providing these facilities exceed the capabilities of some African countries [4]. For example, a time-driven activity-based cost analysis of radiotherapy facilities determined that the cost of purchasing a high-dose-rate brachytherapy afterloader, a three-dimensional brachytherapy treatment planning system (3D-TPS), and the cost of building a brachytherapy suite is $545,000 USD and $272,160 USD, respectively, in a low- and middle-income setting. Similarly, estimates indicate that the expense of training radiation oncologists in low- and middle-income countries is enormous. A radiation oncologist’s training costs $100,000 USD, a medical physicist’s training costs $50,000 USD, a radiation therapist’s training costs $28,000 USD, a dosimetrist’s training costs $39,000 USD, a nurse’s training costs $28,000 USD, and an engineer’s training costs $33,333 USD. These figures are for professional training only, and does not include foundational education, including a medical degree (MBBS), a bachelor’s degree, or continuing professional education [26, 27].
This is prohibitively expensive for nations with underdeveloped health systems that are already trying to address other critical health issues, including malaria, HIV, tuberculosis, maternity and child health, and nutrition. Additionally, they face socio-economic difficulties, such as poverty, insecurity, and political instability [28].
Political instability and conflicts
Africa has experienced varying degrees of conflict and political instability in recent years, ranging from terrorism to war and conflict. In 2021, four successful military coups occurred in Mali, Guinea, Sudan, and Chad, largely as a result of perceived poor governance, insecurity, and foreign interference by former colonial masters [29]. Empirical evidence indicates that during such times, health facilities are destroyed, health professionals are targeted and killed, basic medical supply logistics are devastated, and financial resources intended for infrastructure provision are diverted to insecurity operations rather than public health infrastructure provision. In the long-run, this causes a lot of problems for oncology services, which lead to more cancers and deaths [29-31].
Low screening and vaccination
Cervical cancer screening on a national scale has been implemented in a number of high-income countries since the 1940s [32]. This has resulted in a decline in cervical cancer incidence and mortality rates in these countries. Due to insufficient funding, inadequate infrastructure, and unsatisfactory human resource capacity, screening has largely been opportunistic in the majority of low- and middle-income countries (LMICs). Recent data indicate that screening uptake in Africa varies significantly by region, ranging from 7.65% in Southern Africa to 14.13% in Eastern Africa. This is abysmally low in comparison to the developed world’s average of more than 60%. High-risk human papilloma virus (HPV) has been shown to be responsible for over 90% of cervical cancer cases [33]. This resulted in the discovery and subsequent approval by the United States Food and Drug Administration (FDA) of the HPV vaccine in 2006. The WHO recommended the vaccine as a highly effective intervention for cervical cancer prevention. However, despite of more than 15 years after the vaccine was FDA-approved, only 55% (107 out of 194) of WHO member states have implemented a comprehensive or partial national HPV vaccination program, and only 15% of 15-year-old girls worldwide are vaccinated. Numerous countries, particularly those of LMICs, lack a national HPV vaccination program. Only 31% of eligible girls in 16 sub-Saharan African countries, and about 1% in five Northern African and Western Asian countries, are fully vaccinated [34, 35]. Regrettably, these figures exclude Nigeria, Africa’s most populous country with the highest rate of cervical cancer. Nigeria accounts for 12.5% (14,834/119,284) of cervical cancer cases on the continent, but the country has yet to implement a national HPV vaccination program [36]. Rwanda and South Africa have the highest vaccination rates in Africa, at more than 80%. This success rate is attributed to the government’s political will, international support, and a strategy for implementing school-based screening [37].
Increased screening and treatment of cervical cancer have been shown to have a greater short-term impact on cervical cancer death reduction than vaccination [38]. This is because the impact of the current vaccination campaign as a preventive measure would take several years to manifest. As a result, for women who already have the disease, increasing access to external beam radiotherapy and brachytherapy is the only way to reduce cervical cancer mortality [38].
The current study discovered that the entire region of Central Africa lacks a single brachytherapy unit, as do the majority of countries in sub-Saharan Africa [1, 6]. Women with cervical cancer in these areas or countries must be sent to other countries for treatment, or they could die from the disease [3, 8, 39].
While brachytherapy is indicated for other types of cancer, most notably breast and prostate cancer, it is an integral part of the standard of care for cervical cancer [3, 4]. As a proxy for availability, we used the number of units of brachytherapy per 1,000 new cases of cervical cancer. The next question is: How many brachytherapy units will be needed in Africa by 2030 to treat 90% of cervical cancers?
There is no internationally accepted standard for a number of brachytherapy units per unit population or confirmed cervical cancer, assuming that the output of a machine capable of treating 500 patients per year should be applied to brachytherapy [12, 40]. The number of 119,284 new cases that were found in 2018 would need 235 units, which is more than double Africa’s current capacity. Although North Africa has one of the lowest cervical cancer incidence rates in Africa, it accounts for more than half of all current units. As a result, sub-Saharan Africa has the greatest need to improve access to brachytherapy. To establish an adequate infrastructure for the provision of high-quality brachytherapy in Africa, strategic political action and incremental and sustained investment are required. This goal of treating 90% of cervical cancers in Africa is a high one, but it can be done with a lot of help from African government and non-government organizations as well as from African’s development and financial institutions and African’s private sector.
Limitations of the study
This study has several limitations. First, it can be hard to assure that these facilities are working properly because machine failures are common in Africa, and maintenance times are often long because of lack of local expertise. Second, because the DIRAC database is a self-reporting system, it is occasionally difficult to ascertain the completeness of data. There are also a lot of countries that are always trying to improve their brachytherapy services, but new installations are often not reported in a timely manner. Finally, because many African countries lack high-quality population-based cancer registries, the GLOBOCAN data are estimates. As a result, some cervical cancer incidence and mortality figures may be underestimated.
Conclusions
Africa requires an Afro-centric strategy for cervical cancer elimination that is contextualized and addresses unique challenges in its’ settings. Political campaigns across the continent, funding strategies, and collaboration with professional cancer groups in Africa as well as government and non-government organizations could also be done.








