
Purpose
Anal cancer is an unusual disease accounting for approximately 2% of all gastrointestinal cancers [1]. However, the incidence and mortality are increasing. The estimated incidence and mortality rates for the next ten years are expected to rise from 54,300 to 72,900 and from 22,000 to 30,400 in the world, respectively [2]. For early stages, external beam radiation therapy (EBRT) demonstrated excellent clinical outcomes [3-5], while for locally advanced stages, concomitant radiotherapy and chemotherapy (CRT), such as 5-fluorouracil (5-FU) and mitomycin C (MMC) is the current standard of care [6-9]. External beam radiation therapy for anal canal cancers (ACC) involves the pelvis and inguinal region treated at a dose of 45-50 Gy (without treatment gap), including the tumor, anal canal, regional pelvic nodes, and inguinal nodes. Subsequently, a second volume boost (sequential or simultaneously integrated boost) to the tumor or to pathologic lymph nodes, is mandatory to achieve local control [10-12]. CRT demonstrates excellent rates of loco-regional control of disease and overall survival. By contrast, this effective treatment can impair quality of life; up to 40% of ACC survivors experience digestive toxicities, which negatively impact their real life. Locally advanced tumors are frequently associated with more fecal incontinence than surviving patients with smaller tumors [13]. Nowadays, there is no consensus regarding the boost technique for treatment planning, while the choice of a technique used is based on hospital facilities, physicians’ formation, and medical experience [14]. Our hypothesis was to evaluate if sparing of surrounding normal tissues and the contralateral sphincter provided by brachytherapy could decrease gastrointestinal (GI) toxicity compared with a boost delivered by EBRT. The aim of this study was to evaluate survival outcomes and to compare the impact on toxicity in the choice of boost technique for ACC patients treated in our institution.
Material and methods
Study population
Clinical records of consecutive patients, who underwent interstitial brachytherapy (ISBT) or EBRT boost (EBRTb) after EBRT or CRT in our institution between December 2012 and December 2019, were retrospectively analyzed. The local institutional ethic committee authorized the study design and analysis (approval number: IPC 2024-013). Any size tumors invading adjacent organs, such as T4 tumors (stage, IIIB-IIIC), were not considered. One hundred and sixty-two patients with non-metastatic biopsy-proven anal canal invasive carcinoma (stage, I-IIIA) were enrolled in the study. Tumor staging included pelvic examination, digital rectal examination, rectal ultrasound, pelvic magnetic resonance (MRI), and 18-fluorodeoxyglucose (FDG) positron emission tomography (PET) scanning. Tumor staging was performed as per the American Joint Committee on Cancer (AJCC) TNM staging classification for anal carcinoma (9th edition). Clinical tumor stages were: stage I (15.4%), IIA (17.3%), IIB (8%), and IIIA (59.3%). Nodal positive disease was present in 13 stage IIB (100%) patients and 45 stage IIIA (47%) patients. The patients characteristics are summarized in Table 1.
Table 1
Patient and tumor characteristics
Treatment
External beam radiotherapy
All patients underwent first course of EBRT (19.1%) or CRT (80.9%). EBRT was delivered to pelvis and inguinal region (97.5%), and to anal canal and lower rectum (2.5%), considering tumor size and the risk of lymph node involvement. Patients underwent three-dimensional conformal radiotherapy (3D-CRT) (8.6%) and intensity modulated radiation therapy (IMRT) or volumetric modulated arc therapy (VMAT) (91.4%). Dose was prescribed to the point according to International Commission on Radiation Units & Measurements. EBRT was administered over a five-week period to a dose of 45 Gy in 1.8 Gy (PTV-1). Target goals specified that more than 95% of planning target volume (PTV) will receive the prescription dose, and ≤ 10% of PTV will receive more than 110% of the prescription dose. Daily kV/kV electronic portal images and weekly kV cone-beam CT (CBCT) were performed to assure set-up accuracy.
Clinical target volume 1 (CTV-1) included the entire anal canal and the pelvic, inguinal, pre-sacral nodes, and mesorectum, considering the risk of lymph node involvement and clinical stage. Planning target volume (PTV-1) used 0.7-1 cm expansion margin around CTV-1 [15]. In case of lymph node involvement, at the end of PTV-1, a sequential boost (PTV-2) was delivered, with a mean dose of 20 Gy in 10 fractions. Applying the linear-quadratic model, the total dose (PTV-1 + PTV-2) was 64.3 Gy in equivalent dose at 2 Gy per fraction (EQD2 α/β10).
Chemotherapy
Concomitant chemotherapy was delivered in 131 (80.9%) patients, and most of them (93.9%) received 5-FU (1,000 mg/m2 on days 1-4 and 29-32) and MMC (10 mg/m2 on days 1 and 29); cisplatin (CDDP) (2.3%) with 5-FU CDDP (75 mg/m2 on days 1, 29, and 1,000 mg/m2 on days 1-4 and 29-32); or capecitabine (3.8%) administered through the entire radiation treatment (excluding weekends), with 825 mg/m2/12 hours.
Brachytherapy boost implant
Brachytherapy indication and feasibility were validated by a dedicated consultation before starting EBRT or CRT. ISBT was performed if the tumor did not exceed a half of the circumference of anal canal. Maximal tumor thickness considered (from the wall to the deep) was ≤ 15 mm, and ISBT was delivered to anal canal macroscopic initial tumor site. Brachytherapy technique was described elsewhere [16, 17]. In brief, the implantation procedure was performed under general anesthesia, with a Foley catheter firstly introduced into the bladder. Post-CRT/EBRT, tumor regression was done during brachytherapy (BT) to evaluate the final BT dose. The number of needles was determined by digital exam, anoscopy, and initial extension of disease. According to the Paris system [18], needles were implanted equidistant and parallel using a Papillon’s template ring, perforated at 1 cm intervals. An anal cylinder (25 mm in external diameter) as dilatator was placed at the end of BT to keep the contralateral side of anal canal and normal rectal mucosa away from the needles (vectors). At the end of procedure, the needles and cylinder were attached to the applicator, which was sutured to the perineum (Figure 1).

ISBT treatment planning
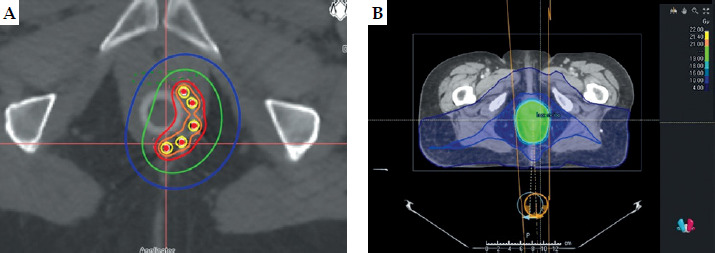
After recovery from general anesthesia, a planning CT scan in the supine position with slice thickness of 1.25 mm was obtained. Images were imported to the Oncentra Brachytherapy planning system (Nucletron), and CTV was delineated according to anal canal initial tumor description, with a safety margin up to 10 mm using a 10 mm diameter pearl. The needles were inserted with precise accordance and geometric principles defined by the Paris system. Dwell positions were subsequently activated at 2.5 mm intervals throughout CTV. Geometric optimization based on volumetric properties was then applied, and dose distribution was normalized to ensure that 100% of the prescribed dose encompassed 90% of CTV. High-dose region defined as 200% of the prescribed dose was systematically evaluated to confirm that its diameter did not exceed 1 cm along the axis perpendicular to the needles. To further limit the high-dose volume, manual or geometric optimization was carried out by the medical physicist. Total dose was calculated as equivalent dose at 2 Gy per fraction (EQD2) [19, 20]. Patients with complete clinical response received a total dose of 12 Gy in 3 fractions over 24 hours (EQD2 α/β10 = 14 Gy), with one fraction delivered on the day of implant and two fractions administered at least 6 hours apart on the following day. Patients with partial response received a total dose of 16 Gy in 4 fractions over 48 hours, with similar interval between fractions (EQD2 α/β10 = 18.7 Gy), and the total prescribed dose was delivered in one implant. Median brachytherapy dose was 12 Gy in 3 fractions (EQD2 α/β10 = 14 Gy). Adding the contribution of EBRT, the median total dose (EBRT + ISBT) was 58.3 Gy in equivalent dose at 2 Gy per fraction (EQD2 α/β10) (Figure 2A).
Fig. 2
A) Brachytherapy implant (sparing not involved sphincter). Red line = 4 Gy isodose (total EBRT + ISBT = 58.3 Gy (EQD2 α/β10)); green line = 2 Gy isodose (total dose EBRT + ISBT = 50.3 Gy (EQD2 α/β10)); blue line = 1.1 Gy isodose (total dose EBRT + ISBT = 47.2 Gy (EQD2 α/β10)). B) External beam radiation therapy boost (EBRTb): homolateral and contralateral sphincter receives the total dose (total EBRT + ISBT = 61.2 Gy (EQD2 α/β10))
Dose prescription
Dose prescription was decided in terms of clinical response and contribution of EBRT dose. Standard dosimetric parameters to target volume were calculated, including CTV, D90, V100, V150, and V200. The most irradiated tissue volumes adjacent to clinical target volume, i.e., reference volumes to 0.1 cm3, 2 cm3 for the bladder, urethra, and vagina/prostate, were estimated. The aim was to limit the total physical dose of EBRT + BT (equivalent dose in 2 Gy fractions) for the bladder and urethra D2cm3 (Gy α/β3) < 50 Gy, for vagina D2cm3 (Gy α/β3) 55 Gy, and prostate D2cm3 (Gy α/β3) < 50 Gy.
EBRT boost
Gross tumor volume (GTV) comprised the macroscopic disease at diagnosis (clinical and suspected lesion on MRI and/or PET-CT, and rectal ultrasound). CTV EBRTb included GTV with an isotropic expansion up to 5-10 mm, and an isotropic 10 mm expansion was applied to obtain PTV EBRTb. The ICRU 83 recommendations were applied for planning, with the aim to deliver 15-20 Gy (1.8-2 Gy/fraction) without interrupting the treatment (Figure 2B).
Response evaluation and follow-up
Tumor response was evaluated at three months post-treatment using digital rectal examination (DRE), inguinal node palpation, pelvic MRI, and chest, abdominal, and pelvic CT. PET-CT scan was performed in patients initially staged as II-III disease. Patients were followed 2-4 weeks after BT, then every 4 months for 2 years, every 6 months for 3 years, and then annually. Acute (< 3 months) and chronic (≥ 3 months) toxicities were assessed using the National Cancer Institute common terminology criteria for adverse events, version 5.0.
Data and statistical analyses
All statistical analyses were performed at a significance level α = 0.05 using SAS® 9.4 software. Data were described by using counts (frequencies) for categorical endpoints, medians (min-max), and means (standard deviations) for quantitative endpoints. Local relapse-free survival was defined as the time from the date of diagnosis to the date of local recurrence or death. Colostomy-free survival was specified as the time from the date of diagnosis to the date of local relapse requiring colostomy or amputation or death. Disease-free survival was defined as the time from the date of diagnosis to the date of local or loco-regional or distant relapse or death. Overall survival was specified as the time from the date of diagnosis to the date of death. Patients without considered events were right-censored. These time-to-event endpoints were estimated by using the classic Kaplan-Meier method, while follow-up was assessed with the reverse Kaplan-Meier method. Univariate and multivariate analyses controlling for other prognostic and confounding factors were measured using Cox regression models. Associated hazard ratios (HR) were estimated with their Wald 95% level bilateral confidence interval. Associations with toxicity endpoints were assessed using Fisher and Wilcoxon tests in terms of the nature of variable, and with univariate and multivariate logistic models, with associated odds ratios (ORs) estimated using their bilateral Wald confidence intervals. As a sensitivity analysis, statistical analyses were repeated in a restricted sub-group of patients with circumferential involvement ≤ 50%, to assess the robustness of findings. The purpose of this analysis was to determine whether the main results remained consistent within this more homogeneous subset of patients.
Results
The median follow-up was 66 months (95% CI: 61.9-69.9), and the median EBRT dose was 45 Gy (range, 36-45 Gy), with 1.8 to 2 Gy per fraction. The median overall treatment time (OTT) from the first day of EBRT or CRT to the completion of boost was 58 days (range, 35-90 days), with 55 days (range, 35-90 days) and 60 days (range, 36-79 days) for ISBT and EBRTb, respectively. Lymph node involvement was present in fifty-five patients, mainly in the EBRTb group (92.7%). The median boost dose was 12 Gy (range, 12-20.4 Gy) and 20 Gy (range, 13.4-24 Gy) for ISBT and EBRTb, respectively.
Local relapse-free survival
Five patients (3.1%) had locally persistent disease at 3 months, and all of them were treated by EBRTb. Thirteen (8.0%) local recurrences were reported, six in the ISBT and seven in the EBRTb groups. Salvage treatment was delivered by abdomino-perineal resection (APR) in sixteen patients, while two patients underwent chemotherapy, followed by APR. The overall local relapse-free survival rate at 5-year was 87% (range, 80-92%), with 88% (range, 79-94%) for ISBT and 86% (range, 74-93%) for EBRTb. Several factors for local recurrence were evaluated in univariate analysis, including overall treatment time, tumor stage, EBRT technique, concomitant chemotherapy, and boost modality. None of these factors increasing the risk of local recurrence were found to be significant in univariate and multivariate analyses (results not shown).
Colostomy-free survival
The five-year colostomy-free survival (CFS) rate was 92% (range, 86-95%), with 95% for ISBT and 88% for EBRTb, and no significant differences were observed between both boost modalities (p = 0.16). At the final analysis, six patients (3.7%) had a colostomy due to toxicity (one patient in the ISBT, and five patients in the EBRTb groups), out of whom four experienced concomitant local relapse.
Disease-free and overall survival
The 5-year disease-free survival (DFS) rate was 84% (range, 78-89%), with 87% (range, 77-93%) for ISBT and 82% (range, 72-89%) for EBRTb (p = 0.15). The five-year overall survival (OS) rate for the entire cohort was 93% (range, 88-96%), with 96% (range, 89-99%) and 91% (range, 82-96%) for ISBT and EBRTb, respectively (p = 0.29).
Toxicity
No grade 4 or 5 toxicities (adverse events) were observed.
Early toxicity
One hundred and fifty-six grade ≥ 2 acute toxicities were reported, with 51.9% and 48.1% of total 130 patients in the ISBT and EBRTb groups, respectively. The most frequent acute toxic event (frequently at the end of EBRT or chemoradiotherapy) was skin toxicity (76.4%) with radiation dermatitis (n = 53 grade 2, and n = 66 grade 3). Thirty-five (22.4%) GI toxicities were observed (n = 27 grade 2, and n = 8 grade 3), including one (0.6%) vascular grade 2 and one (0.6%) hematologic toxicity grade 3.
Late toxicity
A total of 181 chronic toxicities were documented in 100 patients, with 29.8% and 70.2% in the ISBT and EBRTb groups, respectively. Of those, GI toxicity was the most frequent adverse event reported, with 119 (65.7%) events (n = 96 grade 2, and n = 23 grade 3), 39 (21.5%; n = 33 grade 2 and n = 5 grade 3) vaginal/sexual toxicity, and genitourinary (GU) toxicity grade 2 (6.1%), lymphatic toxicity grade 2 (2.8%), five bone toxicity (2.8%), and two vascular toxicity grade 3 (1.1%) (Table 2).
Table 2
Adverse events
GU late toxicity analysis
Late GU grade ≥ 2 toxicity was more frequent among patients who underwent EBRTb (81.8%) vs. 18% in the ISBT boost group. A non-significant tendency was found in the multivariate analysis according to the type of boost (EBRTb vs. ISBT) and late GU toxicity, with OR = 3.48 (0.68-17.69) and p = 0.1333.
GI late toxicity analysis
Chronic GI toxicity grade ≥ 2 was correlated with boost modality, with 44.9% and 67.9% in the ISBT and EBRTb groups (p = 0.0035), respectively. GI toxicities included 30 cases of fecal incontinence (n = 28 grade 2, and n = 2 grade 3), 22 diarrhea grade 2, 15 rectal pain (n = 14 grade 2, and n = 1 grade 3), 23 radiation rectitis (n = 8 grade 2, and n = 15 grade 3), 19 rectal hemorrhage (n = 17 grade 2, and n = 2 grade 3), 2 rectal fistula grade 3, 2 anal stenosis grade 2, 2 flatulence grade 2, 1 rectal perforation grade 3, and 1 anorectal infection grade 2.
In general, rectal pain, radiation rectitis, and rectal hemorrhage grade 3 required hyperbaric oxygen and/or endoscopic intervention (argon plasma coagulation), and six patients (3.7%) underwent colostomy due to toxicity, with four of them showing concomitant local relapse. Univariate analysis for late GI morbidity showed a difference in favor of ISBT boost vs. EBRTb: OR = 2.59 (1.37-4.92), p = 0.0035 (Table 3). After adjustment for other prognostic and confounding factors, this effect was not statistically significant, with OR = 1.82 (0.88-3.78) and p = 0.1060.
Table 3
Univariate and multivariate genitourinary (GI) toxicity grade ≥ 2
Fecal incontinence analysis
To evaluate the sphincter impairment, fecal incontinence was compared and analyzed in both groups, with boost modality, concomitant chemotherapy, surgical resection at diagnosis, histopathology, age, sex, and clinical stage assessed. In univariate analysis, there was a significant difference between boost modality: ISBT vs. EBRTb, 6 (7.7%) vs. 26 (31%), p = 0.0005; and clinical stage: I-II vs. III, 8 (12.1%) vs. 24 (25.0%), p = 0.0473. In the multivariate analysis, ISBT boost modality was the only factor leading to preservation of anal continence, with OR = 7.14 (2.17-23.46) and p = 0.0012.
Sensitivity analyses for GI toxicity and fecal incontinence
To avoid potential bias in the investigation, a sensitivity analysis was performed adjusting more strictly brachytherapy boost indications, to evaluate the impact of boost modality. Patients, who underwent EBRTb, were not eligible for brachytherapy or had theoretical contraindications to ISBT, with tumor topography between 4-6 cm from the anal verge (frequently overflowing to low rectum), tumor extension of more than 50% of the anal canal circumference, and tumor thickness of more than 15 mm, were excluded from the analysis. In total, twenty-two patients were excluded from the EBRTb group, with 62 patients remaining (n = 78 in ISBT vs. n = 62 in EBRTb). Regarding GI toxicity, the effect of boost type did not reach statistical significance, although a trend in favor of ISBT was observed: OR = 1.78 (0.83-3.83), p = 0.1415 (Table 3). Fecal incontinence was reported in 6 (7.7%) and 15 (24.2%) patients, who underwent ISBT and EBRTb, respectively. Univariate and multivariate analyses found ISBT as an independent prognosis factor for better sphincter function: OR = 5.44 (1.57-18.91), p = 0.0077 (Table 4).
Table 4
Fecal incontinence analysis
Discussion
Survivor patients in this population experience digestive toxicities, which negatively impact their real life, and are probably related to the topography and nature of ACC [13]. Since four decades, five randomized clinical trials demonstrated and validated EBRT and/or CRT as the best option to treat ACC [6-12]. Survival rates and toxicities were accepted by the medical community without evaluation of the impact of treatments on patients’ quality of life (QoL) [21]. Fortunately, due to treatment efficacy, ACC patients have nowadays a long survival prognosis, whereas must experience adverse effects and morbidity due to delivered treatments [22]. Chronic digestive toxicity with its impact on QoL remains the most frequent problem to resolve in this population. Among GI toxicities, fecal incontinence is regularly reported symptomatology after pelvic radiotherapy, representing an alteration in patient’s lifestyle due to complex management [23, 24]. There are several studies assessing fecal incontinence in these cases, showing contradictory results. Oehler-Jänne et al. [25] compared brachytherapy boost after treatment break vs. external beam boost without break in the treatment of anal carcinoma. Long-term morbidity and QoL were similar, and brachytherapy boost did not result in improved local control, overall survival, and cancer-specific survival. In contrast, Bentzen et al. [13] reported the prevalence and severity of fecal incontinence in anal cancer survivors by comparing 259 volunteers vs. 107 anal cancer survivors. Both groups were evaluated and compared according to the St. Mark’s score [26]. Stool incontinence was reported by 43% of the survivors and urgency was present in 64% of them, with the survivors having significantly lower global quality of life scores compared with the volunteers. Patients with locally advanced tumors had a higher incontinence score (p < 0.01) [13], while in our series, chronic fecal incontinence grade ≥ 2 was present in 19.8% of the patients. Comparing boost modalities, ISBT demonstrates to be a robust protective effect against fecal incontinence (p = 0.0012), whereas the association with GI toxicity is less pronounced and no longer statistically significant (p = 0.1060). This discrepancy likely reflects the heterogeneity of the composite endpoint: digestive toxicity contains various symptoms with differing susceptibility to the treatment. Furthermore, adjustment for potential confounders may reduce the apparent effect on the overall endpoint, while highlighting the strong, specific effect on fecal incontinence. Nevertheless, given the relatively small number of events, these findings should be interpreted cautiously and warrant confirmation in larger cohorts.
When pelvic-inguinal and boost volume are both delivered by EBRT, the entire anal canal and sphincter are irradiated at high doses. Histopathological damage to tumor and normal tissues induced by EBRT, including perivascular and interstitial fibrosis, lymph node fibrosis, vasculitis, and sclero-hyalinosis, can explain the impairment of sphincter [27]. On the contrary, if the boost is delivered by brachytherapy, the dose to the normal sphincter is negligible due to rapid reduction in the dose. This contributes to the maintenance of continence function, avoiding mechanisms of the development of fecal incontinence after irradiation [28]. There are also other hypotheses regarding the development of fecal incontinence in ACC, such as the relationship between tumor stages, tumor obstruction, and requirement of high radiation doses with large treatment fields. However, there are other pathologies, such as prostate and gynecological cancers, where without anal tumor obstruction, fecal incontinence is a frequent GI toxicity [29-33]. Increased age is also a risk factor [34, 35]. In ours series, the median age of patients was 65 years (range, 29-87), with 67 years (range, 29-87) and 61 years (range, 38-82) in the ISBT and EBRTb groups, respectively (p = 0.05). Moreover, the analysis of fecal incontinence did not show an increased risk of incontinence in relation to age (p = 0.36) and disease stage (p = 0.39).
Recently, a systematic review comparing 651 patients, who underwent EBRTb or ISBT after CRT for the treatment of anal canal cancers, was reported [36]. The authors found superior clinical outcomes in patients treated by brachytherapy compared with EBRTb: 5-year loco-regional control (87.8% vs. 72.8%), cancer-specific survival (91% vs. 78%), overall survival (74.6% vs. 67.7%), disease metastasis-free survival (92.9% vs. 85.6%), and cancer-free survival (76.8% vs. 63.1%). Chronic toxicity was similar between both groups.
Patients undergoing brachytherapy as boost have a double benefit: excellent rates of colostomy-free survival and low toxicity. In a recent study, Kent et al. reported on fifty-two ACC patients, who underwent CRT + boost delivered by ISBT vs. EBRTb. Cancer-related stoma rate at 5 years was 3% for the brachytherapy group and 20% for the EBRTb group, with no treatment-related stomas at 5 years [37]. ISBT delivered by either LDR, PDR, or HDR showed CFS median rates at 5 years of 84% (range, 61-95%), 79% (range, 65-89%), and 80% (range, 79-84%), respectively [38-48]. Furthermore, HDR brachytherapy boost demonstrated a late toxicity rate of 25.7%, with a grade 3-4 toxicity between 2.2% and 8.9% [49, 50].
Even in patients with lymph node involvement (stage ≥ IIIA), brachytherapy boost as treatment option must be offered and discussed. Moureau-Zabotto et al. reported results of 99 ACC patients with lymph node involvement receiving a boost with EBRT or ISBT. They found a significant difference for 5-year cumulative rate of local recurrence (CRLR) in favor of patients treated with ISBT boost [51]. This is in line with our study, where no significant differences in terms of LC, DFS, and OS in patients with early stages vs. patients with locally advanced stages were observed.
Taking into account that overall treatment time is a prognostic factor for the local control of ACC, acute toxicity is a challenge [52, 53]. In our study, to maintain the compliance and avoid an unplanned gap in the treatment, our patients were mainly treated with modern EBRT, including intensity modulated radiation therapy (IMRT) or volumetric modulated arc therapy (VMAT) (91.4%). EBRTb was a sequential boost modality without planned gap. To reduce GI and GU acute adverse events, the RTOG 0529 clinical trial evaluated the rates on toxicity of dose-painted IMRT, with simultaneously integrated boost (SIB) and 5-FU/mitomycin, compared with 3D-CRT and 5-FU/mitomycin from the RTOG 98-11 in ACC patients. The authors found significant reductions in acute grade 2+ hematologic events (73% vs. 85%; p = 0.032), grade 3+ GI events (21% vs. 36%; p = 0.008), and grade 3+ dermatologic events (23% vs. 49%; p < 0.0001) [54]. Long-term evaluation with a median follow-up of 49 months demonstrated grade 3 and 5 toxicities of 16% and 4%, respectively [55]. Since then, several schedules have been retrospectively assessed to avoid treatment break due to toxicity. The ongoing PLATO trial (ISRCTN88455282), an integrated protocol comprising three separate trials, aiming to optimize concomitant chemotherapy and EBRT dose for low-, intermediate-, and high-risk ACC patients, could establish the optimal dose/fraction for each clinical stage [56]. Similarly, definitive results of the French CANAL-IMRT-01 phase 2 clinical trial (NCT02701088), assessing the safety and efficacy of continuous SIB-IMRT without planned breaks and concurrent chemotherapy, are awaited [57].
Dose escalation for ACC do not appear to increase local control. The ACCORD 03 French protocol failed to exhibit the benefit of high-dose radiation on colostomy-free survival, although a small increase in CFS and LC in high-dose-rate brachytherapy arm did not reach statistical significance (p = 0.067) [58]. Accordingly, in our study, the majority of patients underwent HDR brachytherapy boost, receiving a summed dose (EBRT + ISBT) of 58.3 Gy (EQD2 α/β = 10). To avoid the mechanisms of sphincter impairment, the dose delivered to the contralateral sphincter was as low as possible (< 50 Gy).
A controversial indication for brachytherapy is the tumor topography at 4-6 cm from the anal verge (frequently overflowing to low rectum). We performed a sensitive analysis, excluding such patients and those with a circumferential involvement of > 50%, to compare the same cohort with the same theoretical eligibility for ISBT. Univariate and multivariate analyses found ISBT as a protecting factor to develop fecal incontinence (p = 0.0077).
The strength of this study is that clinical outcomes of both boost techniques were in the range of what is seen in the literature, and the efficacy and safety of high-dose-rate brachytherapy boost were shown. Personalized strategies are necessary to decrease GI toxicity rates in these patients; even if a lower rates of late GI toxicity and fecal incontinence in favor of ISBT was found, anal manometry is mandatory to confirm our results in a large, randomized trial.
As monocentric research, our study has certain limitations, such as retrospective nature of data, lack of the anal manometry at diagnosis, and the use of a prospective tool to measure quality of life specific to anal cancer treatment. To our knowledge, this study is the largest series of patients comparing digestive toxicity and the impact of boost technique on fecal incontinence in the conservative treatment for ACC. Prospective randomized trials with quality of life and manometry assessments are necessary to confirm our results.
Conclusions
Interstitial brachytherapy boost appears to have a favorable effect on fecal incontinence, a key component of GI toxicity, compared with EBRT boost. The overall impact on digestive toxicity is less pronounced and should be interpreted cautiously due to the limited number of events. The low impact of brachytherapy in fecal incontinence should be assessed in prospective trials.








