
Purpose
Annually, over 300,000 women are diagnosed with cancers of the uterus worldwide, representing 3.2% of all new cancer diagnoses [1]. Many women have endometrial cancers that are detected at an early stage with excellent long-term prognosis [2]. Some of these women will be treated with vaginal cylinder brachytherapy after surgery, with or without external beam radiation, if their risk for recurrence is high [3]. Adjuvant vaginal brachytherapy is a well-established therapy [4], and offers a decrease in local recurrence in curative treatment of some endometrial cancers [5] and cervical cancers [6].
In treatment planning for high-dose-rate (HDR) single-channel vaginal cylinder brachytherapy, the dose distribution along the cylinder is invariably influenced by the anisotropy of the source [7]. Prescribing dose to the surface of the cylinder has been shown to provide uniform dose to adjacent vaginal mucosa and associated tissues [8]. Multiple source and cylinders exist, and guidance for planning and accounting for dosimetric uncertainty is established in the TG-138; however, dosimetric differences between these systems has not been reported.
Our health system has two different afterloaders and treatment planning systems, i.e. VariSource iX (using BrachyVision v.15.6 from Varian Medical Systems, Palo Alto, CA) and Elekta Flexitron (using Oncentra v. 4.6, Elekta, Stockholm, Sweden). Flexisource consists of a 3.5 mm long iridium-192 (192Ir) core, with a diameter of 0.6 mm enclosed in a 0.85 mm diameter stainless steel capsule. Active length of this source is 3.5 mm [9]. VariSource VS2000 consists of two symmetric 2.5 mm long radioactive iridium sources. Each source is made up of 2.16 mm long cylindrical section, with a 0.34 mm in diameter and active length of 5 mm [10]. Angular dose distribution at a distance from the center of the source as a result of the anisotropy is known to vary as much as ±20% for the VariSource afterloader and ±10% for the Elekta afterloader. This variability in source characteristics may significantly impact dose distribution and treatment-related toxicity [11, 12]. Understanding the impact of different afterloaders and treatment planning systems on variability in the administration of vaginal cylinder brachytherapy is imperative for individualizing therapy, especially when multiple systems are available for use. The purpose of this study was to compare HDR vaginal cylinder brachytherapy treatment plans from two systems, with specific attention to dose at the cylinder tip, the dome, and along the cylinder length.
Material and methods
Plans were generated for cylinders from Varian and Elekta in BrachyVision and Oncentra, respectively. Prescription was to the cylinder surface. Cylinder diameters ranged from 2 and 4 cm, and prescribed treatment lengths varied from 3 and 5 cm, each in steps of 0.5 cm.
In order to quantify the influence of source characteristics alone on the dose along the cylinder, we generated plans for alternate source in each cylinder model. Varian cylinders were also planned in Oncentra using Elekta v.3 source model. This resulted in a comparison of a total of 75 plans, i.e., 5 different cylinder diameters × 5 different treatment lengths × 3 combinations of source/applicator. Dose calculations were according to the TG-43 formalism for photon emitting brachytherapy sources with average energy higher than 50 KeV. Details regarding the source models have been provided in previously published reports 13. We compared Varian cylinder/Elekta source with Elekta cylinder/Elekta source to dose in two cylinders using the same source to isolate the effect of cylinder geometry. Finally, we compared Varian cylinder/Elekta source to Varian cylinder/Varian source to compare the dose in the same cylinder due to use of two different sources to confirm our findings. Optimization points were placed at the tip following the contour of the dome of the cylinder at 3 mm spacing in the superior-inferior direction. Points were also placed along the length of the cylinder at 5 mm intervals in the superior-inferior direction corresponding to dwell positions. Points along the length of the cylinder were only defined up to the length of treatment. The treatment length was equal to active length (distance, over which dwell positions were activated), plus the distance from the farthest dwell position to the tip of the cylinder. The treatment length was found to be approximately 1 cm greater than the active length for both the Elekta and Varian cylinder models. Initially, dwell times were set to equal weights, followed by optimization of dose to the above created points, adjusting dwell time gradient and then graphical optimization.
Mean relative isodose was calculated for each point as well as for the dome and length of the cylinder. Points were modeled after a schema for PORTEC-414, but with all points on the surface of the applicator except A3, which was 5 mm lateral to A1 (see Figure 1). A1 was at the tip, and A2 was at 1/2 the treatment length. Parallel to central axis, A4 was at the first dwell position, and A5 was 1/2 the distance between A2 and A4. A6 was equidistant from A2 in the opposite direction. Patient’s points (P1-3) were distributed along the surface of the dome between A1 and A4 (Figure 2).
Fig. 1
Coronal schematic view of standard vaginal applicator. Modeled after PORTEC-4 [13], but with all points on the surface of the applicator, except A3, which was 5 mm lateral to A1. A1 was at the tip, and A2 was at 1/2 the treatment length. Parallel to central axis, A4 was at the first dwell position, and A5 was 1/2 the distance between A2 and A4. A6 was equidistant from the A2 in the opposite direction. Patient’s points (P1-3) were distributed along the surface of the dome between A1 and A4
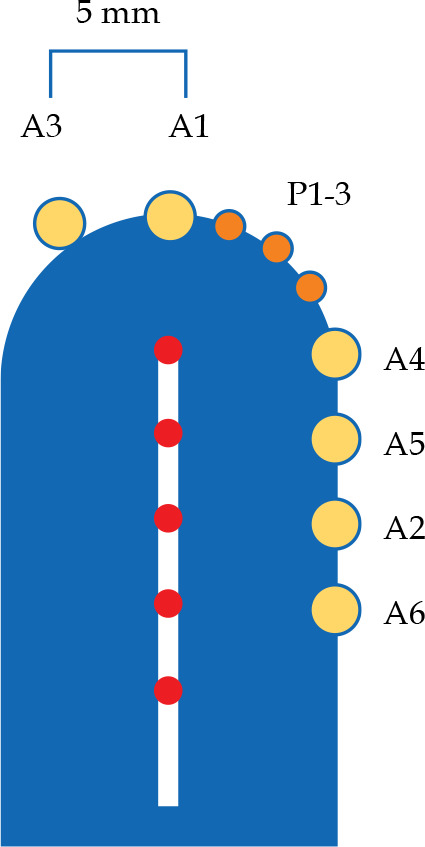
Fig. 2
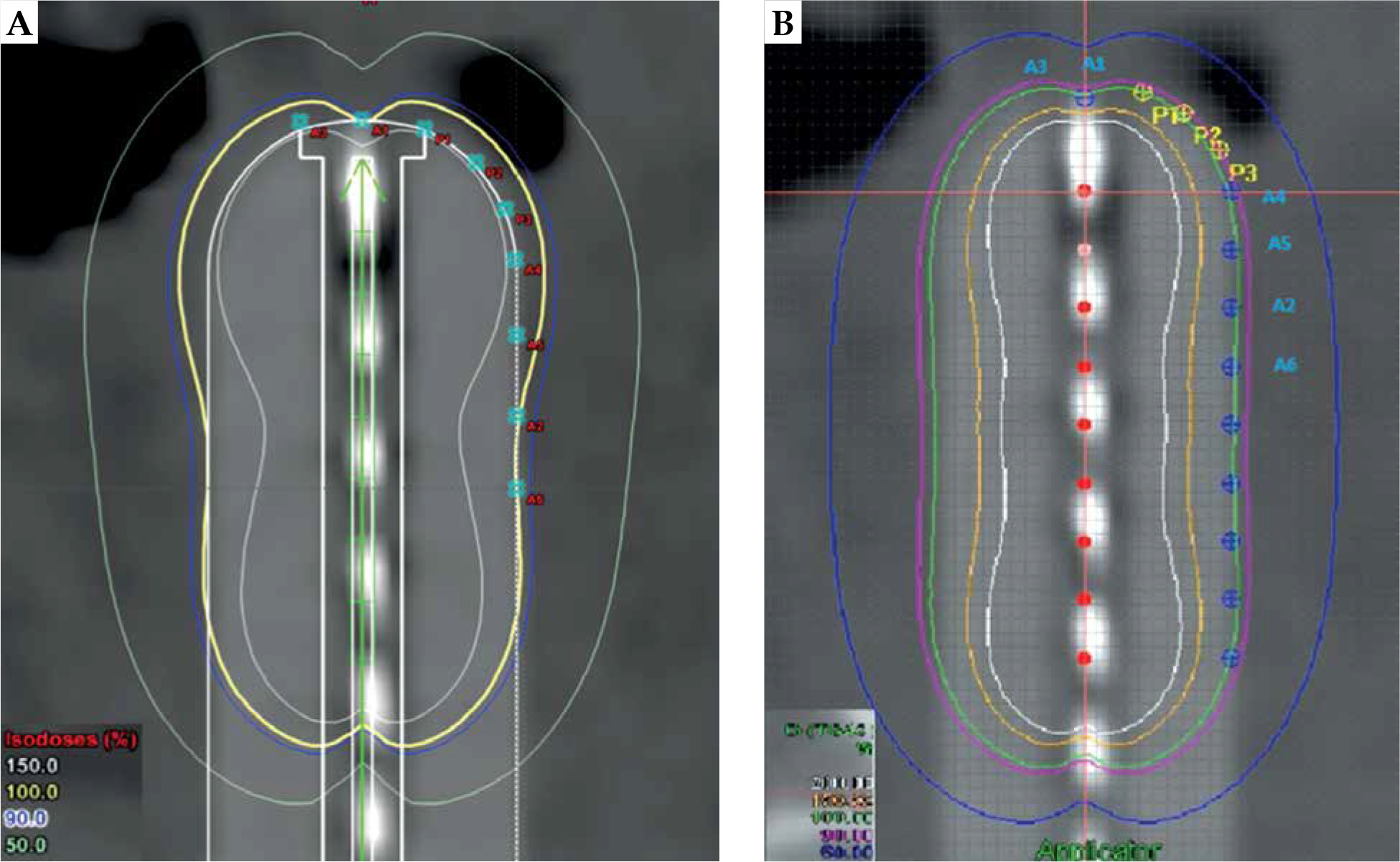
Comparison of dose distribution for Varian 2.5 cm cylinder planned with VariSource (A) vs. Elekta (B) afterloaders
Related-samples Wilcoxon signed-rank tests were performed comparing the mean relative dose between the systems. A two-tailed p value of < 0.05 was considered significant for all tests. Tests were corrected for multiple comparisons. Analyses were performed using SPSS (version 25, IBM Corp., Armonk, NY, USA).
Results
Treatment plans with the VariSource iX source and cylinder demonstrated 16.2% lower (p < 0.001) dose at the tip compared to the Elekta v.3 (Table 1). Average dose to the points along the dome of the cylinder was 128.4% ±17.9% the prescription with VariSource iX source and cylinder, while with the Elekta v.3, the source and cylinder dose was 99.9% ±4.3% (p < 0.001) prescription dose. This difference between systems was noted to be largest with the 2 cm cylinder diameter, 162% and 105%, respectively, as compared with 4 cm cylinder diameter, 104% and 94%, respectively.
Table 1
Treatment plans with VariSource iX source and cylinder compared to Elekta v.3 source and cylinder
Table 2 shows a comparison between the Elekta cylinder and Varian cylinder when using the Elekta v.3 source in both cylinders. When both cylinder types were planned with the same source, no significant differences in dosimetry were observed due to cylinder geometry. Similarly, Table 2 compares the VariSource iX and Elekta v.3 source when using the Varian cylinder. Figure 2 presents a comparative dose distribution. For the same cylinder geometry, the effect of source characteristics on average produced as much as a 36.8% difference in dose homogeneity. All significant differences were maintained when comparing the two different sources in the same cylinder.
Table 2
Comparison between Varian vs. Elekta cylinders using the same source and same cylinder
Discussion
Our study aimed to document the differences in dose delivered along the cylinder surface using two common afterloaders as well as their respective treatment planning systems and cylinders/sources, both of which are available to patients at our institution. Depending on the afterloader, our study shows that the dose at the tip of the cylinder in proximity to the vaginal apex can be as low as 81.3% prescription dose or 97.5% prescription dose. The dose delivered along the cylinder dome in proximity to other areas of the vaginal wall can be more than 30% prescription dose, up to 36.8%, or within 5% prescription dose. The VariSource iX source and cylinder demonstrated greater dose inhomogeneity compared to the Elekta cylinder and source model. While differences in source anisotropy are well-documented [11,15], we quantify the differences between the two systems at our institution that can be taken into account when providing individualized care. For example, while toxicity rates are generally low [16-22], concern for a specific toxicity may be mitigated by greater or less homogenous dose distribution at the tip, dome, or along the length [23, 24].
As expected, there were no significant differences when comparing dosimetry using each cylinder and the same source (e.g., the Varian cylinder and Varian source model and the Elekta cylinder and Elekta source model). In addition, all comparisons remained significant when comparing the Varian source and cylinder versus the Elekta source model and Varian cylinder. Therefore, we conclude that the difference in cylinder geometry between the two systems has little impact on dose distribution, therefore is not an additional factor to be considered when potentially individualizing patients’ care.
These differences in source model anisotropy and resulting variations in dose delivered to the vaginal mucosa may have important significance for tumor control and toxicity [4, 22, 23]. Decreased dose at the tip is important to account for when considering tumor control, while greater dose along the dome and wall may increase treatment-related toxicity, including vaginal toxicity related to increased dose per fraction [10]. Decisions on source selection and considerations regarding dose across two afterloader/treatment planning systems, when available, may be individualized based on the clinical scenario.
Limitations of this study include the focus on dosimetric parameters of the systems and cylinder geometry without assessing clinical outcomes. Clinical studies are needed to demonstrate improvements in dosimetric parameters and clinical outcomes when selecting a system based on documented differences in dose homogeneity.
Conclusions
Our analysis demonstrates that the effect of source characteristics produced up to 37% difference in dose homogeneity when comparing two afterloader/treatment planning systems. We also confirmed that these differences were independent of cylinder geometry. With this comparative insight on variation in dose between two systems, informed decisions around source selection and dosimetry should be made for patients’ individualizing treatment. Further research in treatment planning protocols to optimize dose distribution in vaginal HDR brachytherapy is warranted, especially as prescribing dose to the surface becomes more common.








