
Purpose
Cervical cancer is the fourth most common cancer in women, a disease mainly related to the infection with high-risk human papillomaviruses (HPV). Although most infections with HPV resolve spontaneously, an estimated 570,000 patients were diagnosed with cervical cancer in 2018, and more than a half died from the disease [1]. For early stage cervical cancer, no standard treatment is established, depending on the presence of risk factors. Hysterectomy, definitive external beam radiation therapy followed by brachytherapy, or pre-operative brachytherapy followed by surgery are the main options with excellent clinical results in terms of local and pelvic control rates [2-4]. For locally advanced disease, concomitant chemoradiotherapy (CCRT) followed by brachytherapy (BT) is considered as the standard treatment [5-7]. For many years, hysterectomy (HT) as completion treatment was adopted and performed [8]. Due to radiation-induced inflammation, vascular fibrosis, and adhesions, hysterectomy has an increased risk of significant post-operative entero-vesical and vesico-vaginal fistula, increasing morbidity, and thus compromises the quality of life of patients without clinical benefits [9-14]. Progress has been made in brachytherapy in the last decades. 2D approach based on conventional radiography was replaced by 3D images, and nowadays, magnetic resonance imaging (MRI) to perform image-guided adaptive brachytherapy (IGABT) is mandatory [2,15]. In our center, completion hysterectomy has been abandoned many years ago and simultaneously, brachytherapy implant techniques, i.e., intra-cavitary/interstitial (IC/IS), have been developed mainly in large and poor-responding tumors.
The aim of this retrospective study was to report and evaluate the feasibility and early outcomes of MR-IGABT in patients with locally advanced cervical cancer in the era of hybrid brachytherapy and dose escalation.
Material and methods
Patients with locally advanced cervical cancer treated with a curative intent by definitive radiochemotherapy and IGABT from November 2017 to December 2020 were included (Fig. 1). Some patients were referred to our hospital after radiotherapy-chemotherapy (RT-CT) to perform brachytherapy in our institution. Patients with early stage, insufficient follow-up, or planned post-irradiation hysterectomy were excluded. Patients were staged according to the International Federation of Gynecology and Obstetrics (FIGO) 2018 criteria. After confirmed biopsy, to evaluate local extension and tumor spread at diagnosis, gynecological examination, biomarkers, and pelvic MRI diffusion-weighted (DWI), and dynamic contrast-enhanced (DCE) were performed. In order to estimate regional and distant disease, all patients were assessed by F18-FDG positron emission tomography-computed tomography (PET-CT). Pelvic lymphadenectomy staging was not routinely performed. According to the extent of disease, laparoscopic para-aortic lymph node staging (PAL) was done, except for patients with severe morbidity or age ≥ 70 years [16]. PAL was completed from the common iliac vessels to the left renal vein. Local institutional ethic committee approved the study design and analysis.
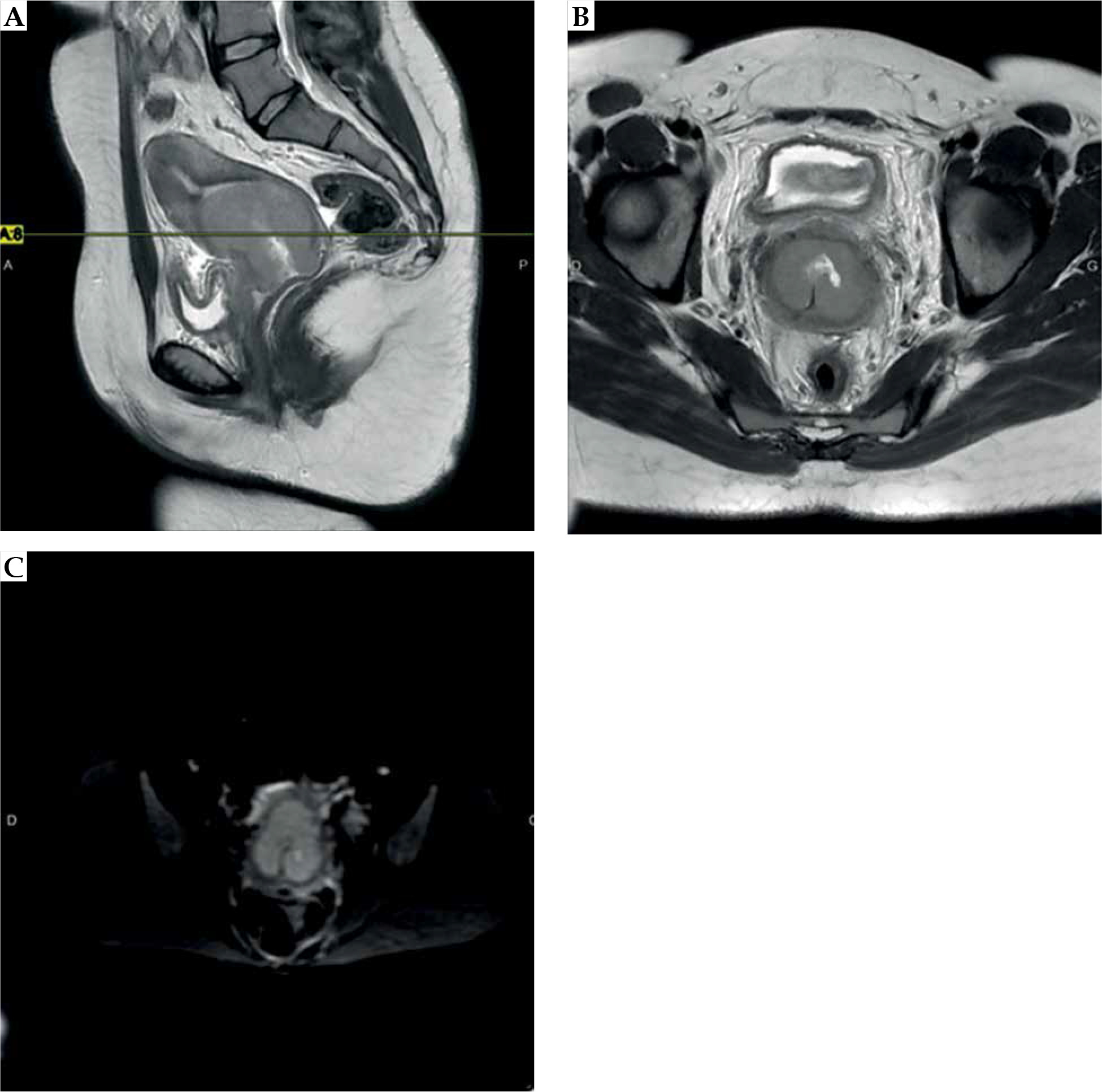
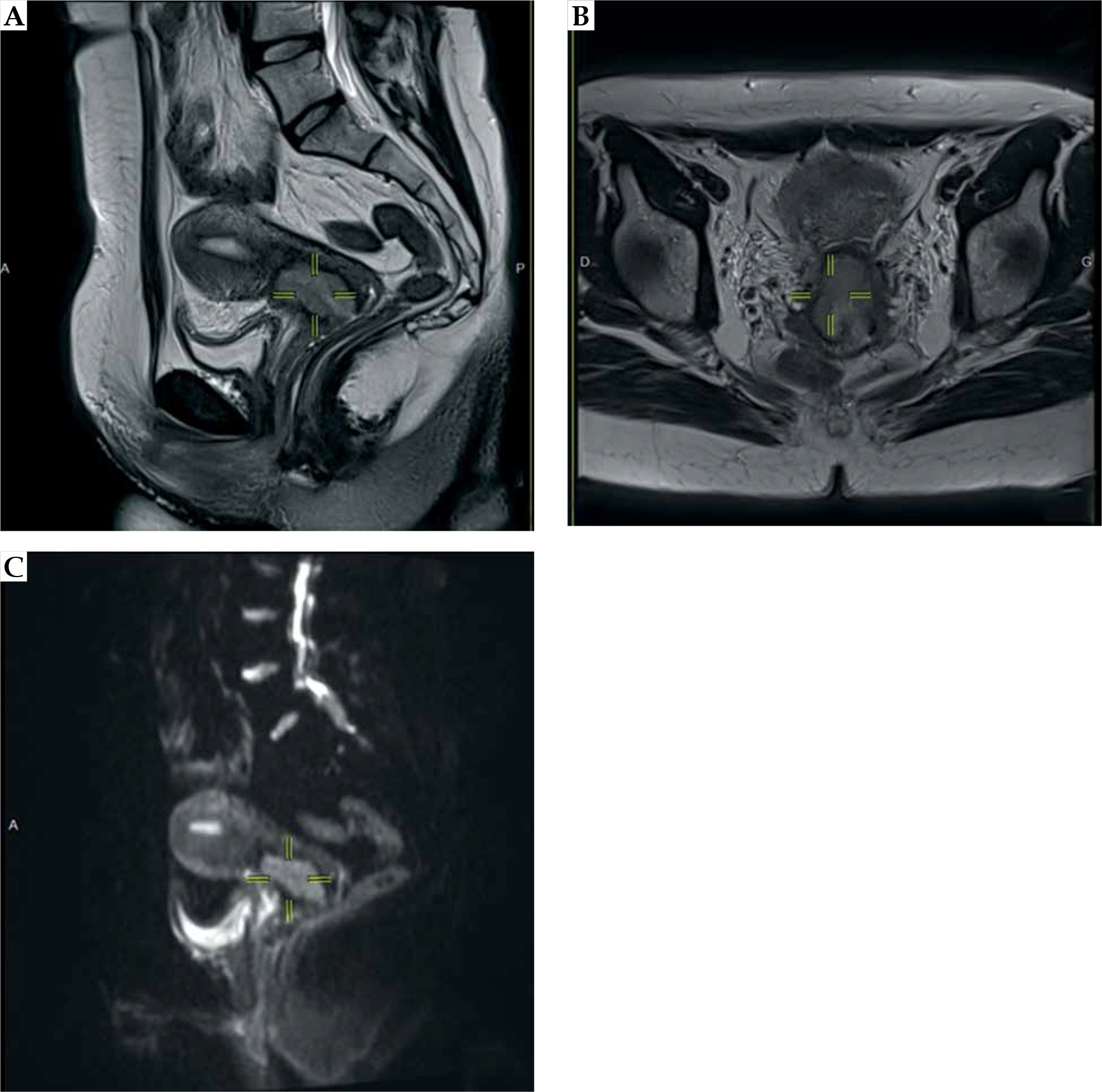
Fig. 1
Locally advanced cervical cancer, MRI at diagnosis. A) Sagittal and B) axial T2-weighted (T2w), and C) diffusion- weighted magnetic resonance imaging (DW-MRI) showing initial tumor extension (grey zones, T2w) and high signal intensity on DWI
Treatment
External beam radiation therapy and concomitant chemotherapy
All patients underwent normo-fractionated EBRT (1.8-2 Gy per fraction, 5 times a week) for a median total dose of 45 Gy (range, 45.0-50.4 Gy) [20]. Treatment was delivered to the pelvis (cervix, uterus, parametria, upper third of the vagina, or more depending on its’ involvement, bilateral external and internal iliac lymph node areas, ilio-obturator, pre-sacral, and common iliac areas, groins were included in case of distal vaginal invasion). Para-aortic lymph nodes (PAN) were irradiated taking into account findings of PET-CT, MRI, and laparoscopic para-aortic lymph node staging, and patients at high-risk for para-aortic nodal recurrence. Considering internal target motion of the uterus (mainly in anterior-posterior direction), two treatment planning CT scans were systematically performed (empty and filled bladder), and all images set were fused. Internal target volume (ITV) of the initial low-risk clinical target volume of the primary tumor (CTV-T LR) was created with adapted margins (usually: 10 mm anterior-posterior, 10 mm superior-inferior, and 5 mm lateral) for optimal target coverage. Patients were treated with three-dimensional conformal radiotherapy (3D-CRT), intensity-modulated radiation therapy, or volumetric modulated arc therapy (VMAT). Pathological lymph nodes were boosted sequentially or with simultaneous integrated boost (SIB) in a range of 55-65 Gy equivalent total dose in 2 Gy fraction dose (EQD2) [17, 18]. A systematic margin of at least 5 mm in all directions was added to generate planning target volume (PTV). Weekly cisplatin (CDDP) was administrated in a dose of 40 mg/m2 of body-surface area IV, applied during EBRT delivery.
Image-guided adaptive brachytherapy
High-dose-rate (HDR) brachytherapy with MR-compatible hybrid applicators (Utrecht or Venezia, Elekta, Veenendaal, The Netherlands) was carried out in all patients. Implant was performed under general anesthesia, with the patient in low-dorsal lithotomy position. Depending on the operator, to improve the accuracy of the implant and to avoid uterus perforation, real-time trans-abdominal ultrasound-guided tandem placement was employed [19]. Number, position, and tissue depth of needles were planned based on clinical examination and MRI performed at the end of radiochemotherapy (Fig. 2). After general anesthesia recovery, CT-scan and MRI in T2-weighted sequence (axial and sagittal without DWI and DCE analysis) were acquired. Dummy sources were inserted in catheters to facilitate the applicator reconstruction. The images were then transferred to Oncentra® (Nucletron, an Elekta company, Stockholm, Sweden). Delineation of target volumes, including residual gross tumor volume (rGTV), high-risk and intermediate-risk clinical target volume (HR-CTV and IR-CTV) as well as organs at risk (OARs), including bladder, rectum, sigmoid, and bowel, were performed according to the GEC-ESTRO recommendations [20, 21]. Dose and target coverage were adapted to D90 HR-CTV (D90: minimal dose to 90% of clinical target volume) and to D90 IR-CTV. Whenever possible and feasible, dose was escalated systematically. At the time of brachytherapy, combined IC/IS technique were performed, especially in large residual tumors, with the objective of dose escalation and to decrease the dose in OARs. Planning aims were ≥ 80 Gy to D90 HR-CTV and ≥ 60 Gy to D90 IR-CTV (dose in 2 Gy equivalents – EQD2, summing EBRT and BT, and applying linear quadratic model with an α/β ratio of 10 Gy and a half-time repair of 1.5 h). Dose constraints were < 70 Gy to maximally 2 cm3 exposed areas of the rectum and sigmoid colon (D2cm3), and 80 Gy to D2cm3 of the bladder (EQD2, similar model with an α/β of 3 Gy). Optimization was performed manually later, in order to adapt dwell times to the topography of the implant. The dose was prescribed to D90 HR-CTV volume. Depending on the tumor response at the end of CCRT, two BT schedules were applied. For good responders or low-risk tumors, BT was performed with one implant and delivered in 2 fractions per day (6 h apart) during three consecutive days, with prescribed dose of 27.5 Gy in 5 fractions of 5.5 Gy at D90 HR-CTV [22]. For high-risk or poorly responders’ tumors requiring combined intra-cavitary and interstitial (or treatment adaptation due to insufficient target volume coverage during first implant), four fractions in two implants (two fractions each one) of HDR brachytherapy were delivered about 1 week apart (fraction 1, 2 and 3, 4). Prescribed dose was 2 × 7 Gy each week (total 4 × 7 Gy) at D90 HR-CTV, corresponding to a prescribed dose of ≥ 80 Gy EQD2 [23]. Two fractions were delivered at the first and at second hospitalization. The first fraction was delivered as soon as possible after the completion of treatment planning. Twenty-four hours later, before the second fraction, a CT scan was done to evaluate the necessity of gas evacuation to avoid rectal anterior wall displacements towards the cervix and high doses [24, 25]. If the rectum was filled with gas, the gas was evacuated and a new CT scan was completed. A new dose-volume histogram (DVH) value was calculated, and the same dosimetry performed for the first fraction was applied.
Treatment response and follow-up
Patients were evaluated at 8 weeks with an abdominal-pelvic MRI, clinical examination, and biomarkers as squamous cell carcinoma antigen (SCC-Ag) or carcino-embryonic antigen (CEA). In case of doubt of complete response, MRI, PET-CT, and biomarkers were repeated 2 months later, and in case of relapse suspicion, a biopsy was performed. In case of complete remission, patients were followed every 3 months the first year, then every 6 months for 2 years, and thereafter annually, with clinical examination and tumor markers. MRI was repeated systematically at least once a year. Acute and late toxicities were assessed using the National Cancer Institute Common Terminology Criteria for Adverse Events v. 5.0 scale [26].
Data and statistical analyses
All statistical analyses were performed at a significance level of α = 0.05 using SAS® 9.4 software. Patients characteristics were summarized with counts and frequencies (calculated on the number of available data) for categorical variables, and with means ± standard deviations or medians and ranges for quantitative endpoints. Univariate and multivariate logistic regressions evaluated the impact on the occurrence of local relapse (respectively pelvic relapse) of brachytherapy parameters (D90 HR-CTV, D90 IR-CTV, and HR-CTV volume), FIGO 2018 stage (III-IV vs. I-II), and overall treatment time (≥ 50 vs. < 50 days). Only significant factors in univariate analyses were included in the multivariate model. Associated odds ratios (OR) were estimated with their Wald’s bilateral CIs and tests for significance. Similar analyses were performed to evaluate the impact of specific brachytherapy parameters on the occurrence of a grade ≥ 2 global (respectively vaginal) toxicity. Local (respectively pelvic) relapse-free survival was defined as the time from date of diagnosis to date of local (respectively pelvic) relapse. Disease-free survival was defined as the time from date of diagnosis to date of local or pelvic or distant relapse or death. Overall survival was defined as the time from date of diagnosis to date of death. Patients without an event were censored at the date of last follow-up. Pointwise estimations with their bilateral confidence intervals were performed using the classic Kaplan-Meier’s method. Follow-up was estimated with the reverse Kaplan-Meier’s method.
Results
A total of 142 patients were included. Patients’ and tumors’ characteristics are summarized in Table 1. Most patients presented locally advanced disease FIGO stage ≥ II (79.6%). At diagnosis, 39.4% showed pathological PET-CT lymph node uptake. At the end of radiochemotherapy, clinical examination and MRI were performed to plan the brachytherapy strategy, and the mean residual tumor was 26 ±12.9 mm.
Table 1
Patients and tumor characteristics
IGABT was based on MRI for all the patients and for each implant. Interstitial BT was performed in seventy-six (53.5%) patients. In 43 (30.2%) patients, brachytherapy was performed with one implant and in 99 (69.7%) patients with two implants. In 30 (21.1%) patients treated with two implants, interstitial BT was not necessary. However, when BT implant was planned only with intra-cavitary technique and the volume target coverage was insufficient, a second implant with interstitial technique (and intra-cavitary) was performed in 31 (21.8%) patients, with the aim to rectify the first implant and to reach brachytherapy planning aims. On the contrary, the number of patients treated with planned combined IC/IS technique for both implants was 38 (26.8%) (Fig. 3).
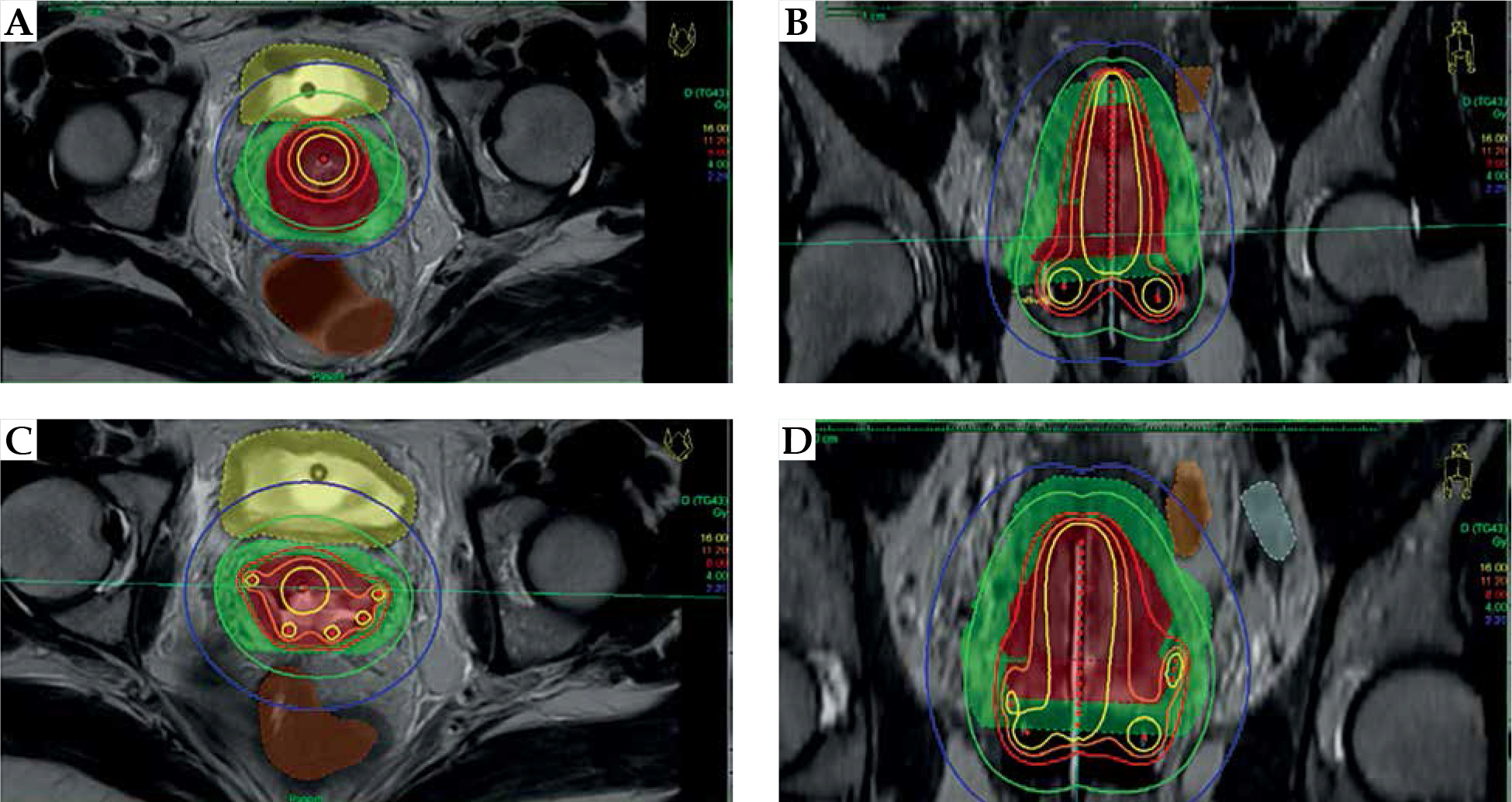
Fig. 3
Intra-cavitary and hybrid brachytherapy. Intra-cavitary brachytherapy: A) first implant, B) unsatisfactory target volume coverage (red and green structures). IC/IS brachytherapy: C) second implant, D) performed with 5 needles to treat a large residual disease post-CCRT, allowing to achieve high-dose to target volumes while sparing organs at risk
The D90 HR-CTV median volume for exclusive IC technique was 17.2 cc (range, 6.3-45.6 cc), and for patients requiring at least one implant with the addition of interstitial technique, the median volume was 24.4 cc (range, 5.1-59.7 cc). Comparing the time of general anesthesia for patients requiring IS BT at the second implant, the addition of IS technique increased significantly the mean general anesthesia time (64 ±14.2 min for IC implants vs. 72 ±15.8 min for combined technique; p < 0.001). In general, for IS BT, the median number of catheters required was 3 (range, 1-6 catheters). Brachytherapy characteristics are described in Table 2.
Table 2
Brachytherapy parameters
[i] CTV – clinical target volume, D2cm3 – minimal dose to the most exposed 2 cm3, D90 HR-CTV – dose delivered to D90 of high-risk clinical target volume, D90 IR-CTV – dose delivered to D90 of intermediate-risk clinical target volume, Gy – Gray, TRAK – total reference air kerma, PIBS – posterior-inferior border of symphysis
Local and pelvic control
The primary endpoint was local control, and complete response was achieved in 133 patients (93.7%). Local control was not achieved in nine patients (6.3%), four of them showed locally persistent and progressive disease, with three concomitant pelvic relapses and one patient with concomitant distant relapse; one patient had concomitant progressive disease and distant relapse and four were exclusives local failures. Local relapse occurred after a median time of 12.3 months (range, 4.8-20.2 months) (Table 3). Twenty-three patients presented a bulky residual disease at the time of brachytherapy (HR-CTV volume ≥ 30 cc), and local control was achieved in 95.7% of the patients.
Table 3
Patterns of local relapse
In univariate analysis for local control FIGO stage (OR = 0.10, 95% CI: 0.01-0.84%, p = 0.034), overall treatment time (OR = 0.11, 95% CI: 0.01-0.92%, p = 0.042), HR-CTV volume (OR = 0.94, 95% CI: 0.89-1.0%, p = 0.47), and D90 IR-CTV (OR = 0.83, 95% CI: 0.70-1.0%, p = 0.47) appeared to be the main risks factors for local control, without independent significant factor in multivariate analysis (Table 4).
Table 4
Univariate and multivariate analyses for local control
Nodal metastasis was present in 56 (39.4%) of patients at the time of diagnosis, out of which, 48 patients were treated with simultaneous integrated (SIB) or sequential boost, seven patients underwent surgical staging without boost, and one patient was not boosted (referred to BT, EBRT in another center). Laparoscopic para-aortic lymph node staging (PAL) was performed in 86 (60.6%) patients, and positive para-aortic lymph nodes were found in 4 (2.8%) patients.
Pelvic relapse occurred in twelve (8.5%) patients, eight of them in non-boosted lymph nodes. The mean time to pelvic relapse was 7 ±5.6 months. Six pelvic relapses occurred simultaneously with distant relapse, two were concomitant with local failure, and three had isolated pelvic relapse; one patient showed a multi-site recurrence. Univariate analyses for pelvic relapse showed FIGO stage (OR = 0.16, 95% CI: 0.03-0.76%, p = 0.022) and overall treatment time (OR = 0.91, 95% CI: 0.83-1.0%, p = 0.042) were considered the main risks factors for pelvic relapse; however, the multivariate analysis did not reveal independent significant factors.
Recurrence-free and overall survival
The median follow-up was 21.6 months (range, 19.1-23.5 months). The estimated 2-year local and pelvic relapse-free survival were 92% (95% CI: 84-96%) and 90% (95% CI: 83-94%), respectively. The estimated 2-year disease-free survival for the entire population was 80% (95% CI: 71-87%). The 2-year OS rate for the entire population was 92% (95% CI: 84-96%). Clinical outcomes are described in Table 5.
Table 5
FIGO stage and clinical outcomes
Morbidity
Interstitial brachytherapy-related complications
Needles implantation for IS BT was technically feasible for all patients requiring this approach. At the end of each implant/treatment and to prevent bleeding complications, applicator removal was performed at the operation room; if bleeding was observed at discharge, continuous compression for at least 5 min was sufficient and the patients were observed overnight. None of the patients (53.5%) required invasive intervention, such as operative hemostasis or arterial occlusion.
Toxicity
High-grade (grade ≥ 3) toxicity was observed in 10 (7%) patients, and acute toxicity G3, including blood toxicity (anemia) related to CCRT was reported in two (1.4%) patients before brachytherapy. High-grade late toxicity (grade ≥ 3) was reported in 8 (5.6%) patients, including three vaginal toxicity G3 (stricture), four bone G3 fracture (increased fracture incidence due to osteoporosis), and one symptomatic lymphocele G3. No late grade 4/5 toxicity was observed.
Brachytherapy dosimetric analyses for toxicity
Dosimetric parameters in patients presenting at least one toxicity G ≥ 2 were reviewed. Univariate analyses were performed taking into account: IS BT (present vs. absent), D90 HR-CTV (≥ 85 vs. < 85 Gy), HR-CTV at the time of brachytherapy (≥ 30 vs. < 30 cc), D90 IR-CTV (≥ 60 vs. < 60 Gy). No factor increasing the risk of toxicity was observed. Regarding vaginal toxicity, a more specific univariate analysis was performed with dedicate parameters, such as International Commission on Radiation Units & Measurements (ICRU) recto-vaginal point, ICRU bladder point, posterior-inferior border of symphysis (PIBS) and PIBS + 2 point, bilateral vaginal point dose at 5 mm, and dwell times (%) (tandem, ring/ovoids, and needles). None of these dosimetric factors were significantly associated with vaginal toxicity.
Discussion
During the last decades, the development of IGABT provided clinical evidence of improved clinical outcomes of modern brachytherapy in cervical cancer [2, 15, 27-32]. The use of MRI plays an important role in the accurate delineation of tumor and critical organs, allowing dose escalation to clinical target volumes (CTVs) [20-23]. In small tumors and those with a favorable response to chemoradiotherapy, intra-cavitary brachytherapy is an adequate and effective modality of brachytherapy [2]. On the contrary, unfavorable situations are usually present with large residual advanced disease, leading to insufficient target volume coverage at the time of brachytherapy. In the past, this group of patients has been treated with EBRT (parametrial boost), exposing organs at risk (rectum, sigmoid, and bladder) to high doses without optimal doses to target volumes [33, 34]. Nowadays, for ‘unfavorable situations’, hybrid technique (IC/IS) is mandatory [35]. The addition of interstitial brachytherapy for cervical cancers represents an opportunity to improve local control, transforming adverse situations into a favorable scenario [15]. In the RetroEMBRACE protocol (1998-2012) [15], IC/IS BT was performed in 23% of patients, and in EMBRACE-I protocol (2008-2015) [35], 43% of patients underwent combined intra-cavitary and interstitial brachytherapy. Approximatively, 70% of patients in both protocols were staged as FIGO IIB-IIIB (73% and 67%, respectively). In our study, 53.5% of the patients required IC/IS BT technique to achieve correct target volume coverage. This high requirement of IS BT was due to the characteristics of our patient population and the BT modality (four fractions in two implants), allowing for correction and improvement of first unsatisfactory IC implant.
Fokdal et al. [36] investigated 58 patients, and reported the feasibility of combined IC/IS BT performing a virtual pre-planning of the interstitial component. They found that the combined treatment was reproducible, and clinical goals were acquired without significant acute morbidity at 3 months. We presented results of IC/IS BT at 21.6 months, and 2 cases of anemia grade 3 (post-radiochemotherapy) were observed with no late grade 4/5 toxicity. Furthermore, the mean time in general anesthesia was on average 8 min longer in IC/IS implants, without compromising the operating room efficiency.
Residual tumor disease after CCRT is a challenge. In this sense, even in adverse situations as large HR-CTV volume at the time of BT, IS BT technique allows appropriate target volume coverage. Mahantshetty et al. [37] showed that distal parametrial/pelvic wall disease can be treated by IC/IS BT. However, intra-operative and during applicator removal complications were frequent (active bleeding, uterus perforation, vaginal lacerations). Generally, this type of complications can be managed without invasive treatments, and in our center, applicator removal is systematically performed at the operating room to avoid urgencies related to acute bleeding.
With the evidence supported by the RetroEMBRACE and EMBRACE-I studies, IGABT is thoroughly validated in clinical practice. The prospective observational study Retro-EMBRACE demonstrated excellent local and pelvic control results. The mean HR-CTV volume was 37 ±24 cm3 and the mean D90 HR-CTV was 87 ±18 Gy. The total 3/5-years actuarial local and pelvic control rates were 91%/89% and 87%/84%, respectively [15]. EMBRACE-I [35], a prospective, observational and multicenter cohort study was recently published, with a median HR-CTV volume of 28 cc (95% CI: 20-40 cc) and median dose to D90 HR-CTV of 90 Gy (95% CI: 84-94 Gy). Moreover, actuarial overall 5-year local control and pelvic control were 92% (95% CI: 90-93%) and 87% (95% CI: 85-89%), respectively. Although 25% of patients received less than 85 Gy to the target volume (D90 HR-CTV), the acquired control local was excellent and superior to the results of RetroEMBRACE. In our study population, 26.7% of the patients received a dose lower than 85 Gy. Despite early results, the present study, showed promising clinical outcomes, with an estimated 2-year local and pelvic relapse-free survival of 92% and 90%, respectively.
Comparing the dose to the target volume between patients who underwent IC BT vs. IC/IS BT, the hybrid technique allowed to increase the dose of D90 HR-CTV (80.8 Gy vs. 83.2 Gy, respectively). The principal benefit of the hybrid technique is the possibility to correctly treat residual disease without increased morbidity. No impact of needle implantation on acute toxicity was found. Interstitial catheters were generally inserted up to three centimeters into the parametrial residual disease, to decrease the risk of arterial and ureteral perforations [38].
Morbidity is a challenge in brachytherapy. Dose-volume (D2cm3, D0.1cm3) and dose point (DICRU) parameters are crucial to estimate and predict the risk of toxicity. Mazeron et al. [39] showed that a D2cm3 ≤ 65 Gy was associated with minor rectal morbidity, whereas a D2cm3 ≥ 75 Gy was associated with major rectal morbidity. Regarding vaginal morbidity, Kirchheiner et al. [40] assessed this parameter from the EMBRACE study. A planning aim of ≤ 65 Gy EQD2 (EBRT + brachytherapy dose) to ICRU recto-vaginal point can reduce and decrease the risk of vaginal morbidity. In the same way, vaginal dose de-escalation to the upper vagina is feasible with IGABT without compromising target dose [41]. Our study showed a mean ICRU recto-vaginal and bladder point of 63.8 ±5.6 and 64.2 ±12.0, respectively, and a mean vaginal loading (ovoid/ring) of 33.9 ±6.5%. These dosimetric recommendations had a favorable impact regarding chronic toxicity in our population; three (2.1%) vaginal toxicities G3 (stricture) were reported without late grade 4/5 toxicity.
In locally advanced cervical cancer (LACC), pelvic and para-aortic positive lymph nodes treatment and control are crucial, and nodal relapse seems to be a relatively early event after treatments. In 2010, Beadle et al. reported a median time to regional recurrence of 13 months (range, 2-85 months), with a mean follow-up of 24 months [42]. In a more recent study, Vargo et al. reported the clinical results of PET/CT positive pelvic nodal disease treated by pelvic and para-aortic irradiation. Patients were assessed by PET/CT at 12 to 16 weeks. The median time to recurrence was 14 months (range, 10-36 months), with a 3-year regional control rate of 94%. Authors found that the nodal remission at the first PET/CT after treatment was a strong predictor for favorable long-term outcomes [43]. In our study, nodal metastasis was present in 56 (39.5%) patients at the time of diagnosis, and most of them received a lymph node boost. In our cohort, 4 patients (2.8%) relapsed in boosted lymph nodes, with the mean time to pelvic relapse of 7 ±5.6 months.
Overall treatment time (OTT) in LACC is one of the most significant prognostic factors. The Retro-EMBRACE study showed that increasing the overall treatment time by one week was equivalent to a loss of 5 Gy in D90 HR-CTV [15]. In order to avoid schedule and logistic-related problems, patients who were referred at our center to underwent only brachytherapy (post-CCRT) received a first consultation before CCRT. The mean OTT in our study was 49.8 ±5.6 days.
Our study found that hybrid technique allows for excellent rates of local control without impact on toxicity, even in large residual tumors after CCRT. On the contrary, distant control remains to be improved. An Outback trial randomized CCRT and BT vs. CCRT, BT, and adjuvant chemotherapy, with 4 cycles of carboplatin and paclitaxel in LACC. At 5 years, overall survival and progression-free survival were similar in both groups: 72% vs. 71%, p = 0.91 and 63% vs. 61%, p = 0.61, respectively. Patterns of disease recurrence were similar in these two treatment groups [44]. Immune check-point inhibitors, such as PD-1/PD-L1 inhibitors, can be a promising approach for cervical cancer treatment [45, 46]. In France, evidence is awaited form ongoing AtezoLACC study (EudraCT Number: 2017-003622-33), a randomized phase II trial evaluating the benefits of the addition of immunotherapy (given concurrently and as adjuvant treatment) compared to standard CCRT and BT.
Our study has some limitations, such as single-center study and the retrospective nature of the data susceptible to biases. Although longer follow-up remains necessary in our analysis, early clinical outcomes of this report confirm the safety and routine application of interstitial brachytherapy for LACC.








