
Purpose
Gynecological malignancies are most often treated with radical radiation and concurrent chemotherapy. Brachytherapy has been an integral part of radiation therapy in gynecological malignancies. The inherent property of brachytherapy permits for a steep dose gradient, delivering higher doses to the target and lower doses to organs-at-risk (OARs). Therefore, it contributes significantly to improvement of local control and overall survival in patients with gynecological cancers [1, 2].
Lower urinary tract symptoms (LUTS) consist of irritative symptoms, obstructive symptoms, and bleeding [3, 4]. 56-60% of patients undergoing concurrent chemoradiation for carcinoma cervix suffer from LUTS, which negatively impact their quality of life [5]. LUTS commonly reported by patients include dysuria, frequency, urgency, nocturia, hesitancy, stranguria, incontinence, urinary retention, and pelvic pain. Overlapping symptoms caused by radiation-induced bladder toxicity vs. radiation-induced urethral toxicity make it difficult to identify, and report urethral toxicities separately.
Locally advanced malignancies of cervix, vagina, vulva, and vaginal vault are treated with perineal template-based interstitial brachytherapy (ISBT) or hybrid intracavitary-interstitial brachytherapy (IC-ISBT). High-dose-rate (HDR) ISBT boost after whole pelvic irradiation (WPI) of 45-50 Gy in 25 fractions involves delivery of 5-7 Gy in 3 to 5 fractions. The Groupe Européen de Curiethérapie (GEC), the European Society for Radiotherapy and Oncology (ESTRO), and the American Brachytherapy Society (ABS) have recommended various dose fractionation regimens and dose constraints to OARs, such as rectum, bladder, and sigmoid colon. However, urinary sub-structures other than whole bladder are not routinely contoured, and therefore, studies on dose constraints and dose volume parameters are lacking.
Female urethra measures about 3.5-4.5 cm and pierces the pelvic diaphragm in its course, with about two-thirds of the urethra being cranial to the levator ani [6]. The urethra has been observed to be in a close relation with target volume during ISBT. Paraurethral glands of Skene are a conglomeration of small glands, which lie within a circumference of 1 cm around the urethra. They are arranged in longitudinal duct-like structures, situated in caudal two-thirds of the urethra, predominantly within the dorsal and lateral mucosal stroma [7, 8]. These paraurethral glands are similar to male prostate, and their secretions are proposed to have a role in prevention of urinary tract infection [7-9]. Pelvic magnetic resonance imaging (MRI) is undoubtedly the best imaging modality to delineate female urethra. However, costs and logistics make MRI less pragmatic. Computerized tomography tomography (CT) imaging is routinely done in most centers for brachytherapy planning. With a Foley’s catheter in situ, the urethra can be well-delineated on CT images.
The urethra is in close proximity to the target during ISBT, especially in cases of carcinoma cervix with an involvement of anterior vaginal wall, vaginal, and vault carcinoma. However, doses to the urethra and periurethral regions have been less commonly reported in literature. The current study was a retrospective research to evaluate dose-volume parameters of female urethra during HDR ISBT in locally advanced gynecological malignancies.
Aims and objectives
To assess dose-volume parameters for female urethra as an OAR during ISBT for locally advanced carcinoma of the cervix, vagina, vulva, and post-operative vaginal vault.
Methodology
Records of 24 patients with biopsy-proven locally advanced carcinoma of the cervix, vagina, vulva, and post-operative vaginal vault, registered between July 2019 to March 2020 were selected for the current study. All patients received external beam radiotherapy (EBRT) by 3D-CRT technique, twenty-two patients received a total dose of 50 Gy/25 fractions, and two patients received 45 Gy/25 fractions, accompanied by 4-5 cycles of concurrent platinum chemotherapy.
After completion of EBRT, interstitial brachytherapy boost was applied to all patients. All the involved patients were catheterized using a 14 French (Fr) Foleys’ catheter prior to the commencement of brachytherapy procedure. 7 cc of distilled water was used to inflate Foleys balloon and pulled down to ensure that the bulb touches the bladder neck. ISBT was performed using Syed-Neblett template-guided placement of needles through the perineum. Central tandem was used in cases of Ca. cervix with intact uterus, and whenever uterine sounding was possible.
Computerized tomography planning scan was performed for all the patients, with a slice thickness of 3 mm. Bladder contrast was obtained using 5 cc of contrast diluted with 20 cc normal saline, administered through Foleys’ catheters in a retrograde manner, just prior to CT scan.
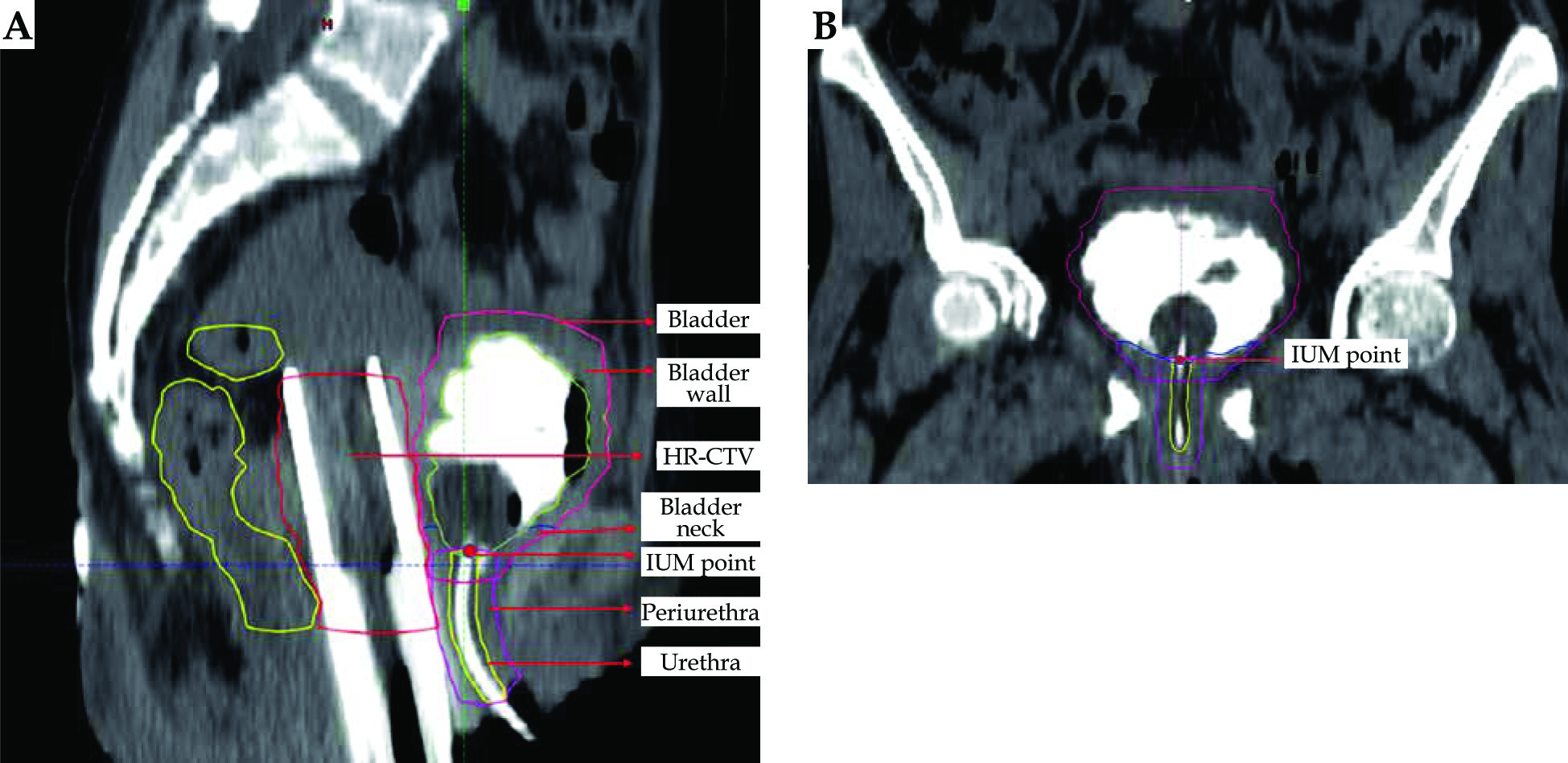
Contouring of high-risk clinical target volume (HR-CTV) was performed in all cases as per clinical findings obtained by examination under anesthesia (EUA), and according to the GEC-ESTRO and ABS guidelines. Urethra and periurethral tissue was contoured retrospectively on planning CT scans of these patients (Figures 1A and B).
Fig. 1
A) Sagittal section of pelvic CT scan with interstitial brachytherapy (ISBT) application in situ demonstrating contours of urethra and periurethral tissue as organs-atrisk (OARs). B) Coronal section of pelvic CT scan with ISBT application in situ demonstrating contours of urethra and periurethral tissue as OARs
Urethral contouring
Urethra was identified by 14 Fr Foleys’ catheters, with contrast inside on the axial, sagittal, and coronal images. Measurement of the outer diameter of 14 Fr Foleys’ catheters was 4.62 mm (1 Fr = 0.33 mm). Muscular tissue of the urethra around Foleys’ catheters was identified, which had a ‘target-like’ appearance on axial images. The contour extended cranially, from just below Foley’s balloon marked by the junction of the neck of bladder, with internal urethral meatus (IUM). Moreover, the intra-mural part was traversing the wall of bladder neck and extending caudally up to the external urethral meatus (EUM) [6]. The urethra was divided into two parts, one above PIBS (posterior inferior border of pubic symphysis) point and one below. Recommendations provided by Spampinato et al. [10] for contouring urinary sub-structures on MRI were used as a guide for extrapolation on CT scan.
Periurethral tissue was contoured with a circumferential expansion of 5 mm around the urethral circumference to include all soft tissue around the urethra from the level of bladder neck to EUM, and to encompass the periurethral glandular tissue. The whole urinary bladder, bladder wall, and the bladder neck were also delineated.
Dose-volume parameters, including volume of urethra, periurethral tissue, and total length (above and below PIBS) were recorded. IUM point was adapted according to internal urethral ostium point reported by Spampinato et al. as the point of intersection between the bladder neck and urethral midline [10].
Maximum dose received (Dmax), mean dose received (Dmean), and minimum dose received by the most exposed 2 cc, 1 cc, 0.5 cc, 0.2 cc, and 0.1 cc (D2cc, D1cc, D0.5cc, D0.2cc, and D0.1cc, respectively) of the urethra and periurethral tissue were recorded. Dose-volume histogram (DVH) parameters were also documented for the urinary bladder, bladder wall, and bladder neck.
Statistical analysis
Results of continuous measurements were studied by mean ± standard deviation (SD), and dosimetric parameters were expressed using median ± interquartile range (IQR). Unpaired t-test was applied for comparison of means. Pearson’s correlation was used to measure degree of association between dose-volume parameters.
Results
Baseline parameters of the 24 patients are presented in Table 1, with 20 Ca. cervix patients, 1 Ca. vagina, and 3 Ca. vaginal vault patients. 25% (5/20) patients of Ca. cervix had lower third vaginal extension post-EBRT, whereas 80% (16/20) cases showed residual parametrial involvement up to lateral pelvic wall, thus mandating the use of ISBT. All the patients were treated using 3D-CRT technique. 92% of patients received a total EBRT dose of 50 Gy in 25 fractions, followed by 6 Gy × 4 ISBT fractions. Urethra and periurethral tissue contoured on the planning CT images of ISBT are demonstrated in Figures 1A and B. Dose-volume parameters of urethra are shown in Table 2, and dose-volume parameters obtained for periurethral volume are presented in Table 3.
Table 1
Baseline characteristics (n = 24)
Table 2
Dose-volume parameters for urethra as organ-at-risk
Table 3
Dose-volume parameters for periurethral tissue
Patients with residual disease involving anterior vaginal wall were expected to have higher urethral and periurethral doses, owing to anatomical proximity of HR-CTV. Nine patients had involvement of anterior vaginal wall among whom, 5 were Ca. cervix IIIA, 3 presented with Ca. vault, and 1 was Ca. vagina. Urethral and periurethral doses in these 9 of 24 patients were significantly higher in comparison to the remaining 15 cases with no involvement of anterior vaginal wall, using Student’s unpaired t-test (Tables 4 and 5).
Table 4
Comparison of dose-volume parameters for urethra between patients with and without anterior vaginal wall involvement (*p < 0.05 – statistically significant)
Table 5
Comparison of dose-volume parameters for periurethral tissue between patients with and without anterior vaginal wall involvement (*p < 0.05 – statistically significant)
DVH parameters of the bladder, bladder wall, and bladder neck are demonstrated in Table 6. A moderate positive correlation could be established between the point dose at IUM vs. DVH parameters of the urethra (Table 7). DVH parameters of the bladder neck revealed a moderate positive correlation with corresponding DVH parameters of the periurethral region (Table 7).
Table 6
Dose-volume histogram (DVH) parameters for bladder, bladder wall, and bladder neck
Table 7
Pearson’s correlation between dose-volume histogram (DVH) parameters for urethra and periurethral regions
Discussion
Template-based ISBT has been used in locally advanced malignancies of the cervix, vagina, vulva, and vaginal vault post-EBRT. Female urethra is an important, but underestimated OAR, which is closely related to HR-CTV during interstitial brachytherapy. In cases of Ca. cervix and vaginal vault carcinomas with a residual disease involving anterior vaginal wall and vaginal cancers, the urethra would be in extreme proximity to high-dose regions. However, doses to the urethra have been reported in only some studies [11-13].
In a study, Spampinato et al. [10] have proposed a method to contour the urethra on MRI taken at the time of image-guided brachytherapy planning. The current study was conducted in a high-volume regional cancer center, with a single-diagnostic MRI machine, and MRI at the time of brachytherapy was not available due to logistic issues. The urethra was delineated on the planning CT scan obtained at the time of brachytherapy planning, similiar to Amsbaugh et al. [11] and Rajagopalan et al. [12]. The use of uniform size Foley’s catheter and that of fixed volume with 25 cc of bladder filling at the time of CT planning has ensured reproducibility. On T2-weighted MRI axial images, four distinct layers were described, such as outermost layer of longitudinal smooth and circular striated muscle cells (hypointense), middle sub-mucosal layer of vascularized connective tissue and smooth muscle cells (hyperintense), inner mucosal layer of epithelial cells (hypointense), and innermost layer of hyperintense urine or secretions, which may or may not be seen [10]. Cranially, the urethra was delineated from just below Foley’s balloon. Corresponding to pre-prostatic or intra-mural part of male urethra, the cranial most part of urethra traverses through muscular wall of the bladder neck, which is called ‘intra-mural part of the urethra’, accounting for nearly 20% of urethral length [6], as shown in Figures 1A and B. PIBS-urethra (PIBS-U) point has been defined in literature as an intersection of PIBS plane and urethra mid-line [13]. PIBS-U point has been used as inferior level of urethral contour in order to maintain uniformity in other studies [10]. However, urethral extension below PIB-U was visible on CT images; therefore, an attempt was made to contour this lower third of the urethra, until visible EUM.
Rajagopalan et al. [12] have reported a mean urethral volume of 1.31 cm3 in 16 patients treated with ISBT for vaginal carcinoma, with BT dose per fraction of 3.9 Gy (1.4 to 6.9 Gy) and 0.60 Gy (0.0 to 3.2 Gy) to 0.1 cc and 1 cc of urethral volume, respectively. Total EQD2 doses to urethral 0.1 and 1 cc were 76.2 Gy (49.4 to 111.2 Gy) and 48.9 Gy (43.2 to 68.1 Gy), respectively. Extrapolating from α/β values of late reacting OAR, such as bladder and rectum, a value of 3 has been used for calculation of EQD2 values. The current study observed a mean urethral volume of 1.14 ±0.27 cc, with similar doses of 3.54 ±1.09 Gy to 0.1 cc and 1.50 ±1.21 Gy to 1 cc of the urethra per fraction. Nine of 24 patients presented with anterior vaginal wall involvement, which was a part of HR-CTV. EQD2 to 0.1 cc and 1 cc of the urethra in these cases were 45.18 Gy and 28.08 Gy with ISBT. Assuming the urethra to have received full dose in EBRT, a total EQD2 of 90.18 Gy and 78.08 Gy to 0.1 cc and 1 cc of the urethra were obtained. Among various DVH parameters, including Dmax/Dmean/D1cc/D0.1cc, the optimal parameter is yet to be defined, based on clinical correlations.
In the current study, the periurethral region was delineated, which has not been performed in earlier studies. This region was observed to have significantly high-dose areas in patients with residual disease involvement within anterior vaginal wall. Nine patients had involvement of anterior vaginal wall at the time of brachytherapy. The impact of these hot spots on the urethral support tissue is yet to be studied. According to Macura et al. [14], four key anatomic factors of the urethra responsible for continence include coaptation (inner mucosal seal), compression (collagenous extracellular matrix along with urethral smooth and striated muscles), periurethral support, and neural control. Stress incontinence often results from urethral sphincteric abnormality caused by damage to any of these above-mentioned four anatomic components. Weakening of proximal urethral sphincter within the periurethral region may lead to widening of IUM at the bladder neck, called ‘funneling’, which is commonly associated with stress incontinence. The extrinsic voluntary sphincteric mechanism surrounding the middle-third of urethra is composed of striated muscles in this periurethral region [14]. Whether high-dose points within this periurethral region weaken the sphincter support of urethra is an unanswered question, which requires to be determined in forthcoming studies.
The periurethral region is a surrogate marker of periurethral glandular tissue, which contributes to the normal urethral secretion and homeostatic anti-microbial effect. A cadaveric study by Clohosey et al. [15] revealed that periurethral space has several PAS-positive mucus glands, nerves, and blood vessels. The secretions of para-urethral glands were suggested to play a role in prevention of urinary tract infection [7, 8]. Female urethral syndrome is a common clinical entity with symptoms resembling lower tract urinary infection, but without significant bacteriuria with a conventional pathogen [16]. Inflammation of paraurethral glands and urethral spasm are two of many different etiologies. Tenderness along anterior vaginal wall over paraurethral glands is considered a sufficient evidence of infection of these glands, as suggested by Gittes et al. [17].
Cranial most part of the urethra traverses through muscular wall of the bladder neck, which is called ‘intra-mural part of the urethra’ [6]. Therefore, DVH parameters of the bladder wall and bladder neck were also analyzed in the present study. It has been reported that during ICBT, the bladder neck receives lower doses compared to the trigone [10]. In the current study with ISBT, the bladder neck received a mean dose of 3.29 ±0.79 Gy per fraction (total EQD2 at brachytherapy = 16.65 Gy, range, 12.31-22.42 Gy) to D2cc at brachytherapy. However, D0.1cc was significantly higher, resulting in 5.19 ±1.08 Gy per fraction (total EQD2 at BT = 35.73, range, 30.73-39.02 Gy). The trigone of bladder could not be distinctly identified, as the entry of ureters into the bladder could not be delineated clearly on a non-contrast CT scan performed post-brachytherapy application. Therefore, a comparison was not possible. DVH parameters of the bladder neck also presented a moderate positive correlation, with D2cc of the periurethral region. This might be explored further in relation to urethral incontinence in future studies. IUM point at a point of intersection between the bladder neck and urethral midline has been suggested as a surrogate marker for the urethral dose in ICBT [13]. However, in the current study, moderate positive correlations between IUM point dose and D1cc, D0.5cc, D0.2cc, and D0.1cc of urethral doses were revealed.
The symptoms of female urethral syndrome correspond to both acute and late radiation cystitis. While acute radiation cystitis and possible urethritis result from mucositis, multiple pathophysiological mechanisms, involving vascular ischemia, perivascular fibrosis, urothelial injury, fibroblast proliferation, and collagen deposition within smooth muscles of the lower urinary tract, have been suggested for late radiation cystitis [18]. Proximal two-thirds of the urethra, being lined by the same urothelium, would demonstrate similar radiation-induced changes, thus resulting in an increased frequency of micturition, dysuria, and pain during micturition.
Limitations of the current study include its’ retrospective nature, dosimetric reporting only, and single-institution reporting. The patients will be followed up, and a clinical correlation of toxicity will be reported separately.
Conclusions
Female urethra receives significant doses during interstitial brachytherapy for gynecological malignancies, especially when the anterior vaginal wall is the target volume. In such cases, one must consider the urethra as an organ-at-risk for future toxicity evaluation. This would enable to develop clinical correlation and dose-volume constraints for the urethra as an OAR in future.








