
Purpose
Ambulatory anaesthesia is an essential component of modern perioperative care, driven by the need for rapid patient recovery through cost-effective healthcare strategies. Goals extend beyond providing adequate procedural conditions to achieving predictable emergence, haemodynamic stability, early mobilisation, and minimising complications that delay discharge [1-3]. These priorities are vital in gynaecological oncology, where brachytherapy is commonly performed as a short-duration procedure under general anaesthesia with total exposure usually less than 30 minutes [4, 5]. Volatile anaesthetics remain the mainstay for maintenance in ambulatory procedures, with sevoflurane and isoflurane being the most widely used agents [6, 7]. While sevoflurane is valued more for its low blood-gas partition coefficient, which promotes rapid patient recovery [8], its significantly higher cost raises concerns about cost-effectiveness in resource-constrained environments [9, 10]. In comparison, isoflurane provides a more affordable and accessible alternative, possessing a long-established safety record [11-13].
Recovery characteristics may differ in very short procedures. Chiu et al. [14] reported faster emergence with isoflurane compared to sevoflurane in surgical procedures lasting about 20 minutes. This finding is attributed to pharmacokinetic differences at the level of brain tissue. Although sevoflurane’s low blood-gas solubility generally favours rapid offset, its higher brain-tissue solubility may prolong emergence after brief exposures [15, 16]. These observations underscore the need to reassess the choice of anaesthetic for brief oncology procedures. Limited evidence exists explicitly comparing the recovery profiles and cost implications of sevoflurane versus isoflurane in short-duration procedures, such as brachytherapy. Due to high patient volumes, short procedure times, and institutional cost pressures, a re-evaluation of anaesthetic agent selection is necessary.
We conducted a randomised, non-inferiority clinical trial comparing maintenance anaesthesia with sevoflurane and isoflurane in women undergoing intracavitary brachytherapy. The primary endpoint was emergence time, defined as the interval from discontinuation of anaesthesia to eye opening in response to a verbal command. The primary hypothesis was that isoflurane would not prolong emergence time by more than 3.2 minutes compared to sevoflurane. Confirming non-inferiority would support isoflurane as a cost-effective alternative with comparable recovery profiles.
Material and methods
Study design and setting
This prospective, randomised, single-centre, non-inferiority clinical trial was conducted at the Postgraduate Institute of Medical Education and Research, Chandigarh, India, a tertiary care hospital. This manuscript adheres to the applicable CONSORT guidelines for non-inferiority trials.
Ethical considerations
The trial protocol was approved by the Institutional Ethics Committee (IEC approval number: IEC-INT/2022/MD-540) and registered prospectively with the Clinical Trials Registry of India (CTRI/2022/11/047441). The trial registration can be verified by searching the registration number at the CTRI website (https://ctri.nic.in). Written informed consent was obtained from all participants before enrolment, in accordance with the principles outlined in the Declaration of Helsinki.
Study population
Female patients aged 45 to 65 years with American Society of Anesthesiologists (ASA) physical status I–III scheduled for ambulatory intracavitary brachytherapy under general anaesthesia were eligible. All patients underwent pre-anaesthetic evaluation in advance in the pre-assessment clinic or ward, with ASA physical status and comorbidities documented, and reconfirmed by the attending anaesthesiologist on the day of the brachytherapy procedure. The ASA Physical Status Classification is a standardised six-grade system used widely by anaesthesiologists to grade the severity of pre-existing systemic disease and to stratify perioperative risk in clinical practice and research [17]. Exclusion criteria included clinically significant hepatic, renal, or cardiac dysfunction; chronic use of sedatives or narcotics; and contraindications to the use of a supraglottic airway device.
Randomisation and blinding
Using a computer-generated sequence, participants were randomised in a 1 : 1 ratio to the sevoflurane group (Group S) or the isoflurane group (Group I). Allocation concealment was ensured through the use of sequentially numbered, opaque, and sealed envelopes prepared by an independent investigator. The anaesthesiologist administering the anaesthesia was aware of the group allocation, whereas patients and all postoperative outcome assessors were blinded to the treatment assignment.
Brachytherapy technique
All patients received high-dose-rate (HDR) intracavitary brachytherapy for locally advanced cervical carcinoma as part of definitive treatment, following institutional protocol and national guidelines [18]. The brachytherapy component was delivered using intracavitary tandem-ovoid or tandem-ring applicators without interstitial needles, with applicator selection individualised according to uterine anatomy and vaginal dimensions. After applicator insertion under general anaesthesia, planning computed tomography (CT) was performed to verify applicator position and delineate target volumes and organs at risk. An HDR intracavitary brachytherapy schedule of 7 Gy per fraction for a total of four fractions was employed after external beam radiotherapy for locally advanced cervical cancer, an approach that has demonstrated effective local control, acceptable toxicity, and good patient compliance in the Indian setting. The treatment was planned to achieve adequate D90 coverage of the high-risk clinical target volume (HR-CTV), while balancing oncological efficacy and toxicity.
Anaesthesia management
All the participants underwent a standardised pre-anaesthetic evaluation. This included clinical assessment, baseline investigations, and cognitive screening with the Montreal Cognitive Assessment-Basic (MoCA-B). Premedication consisted of oral alprazolam 0.25 mg and ranitidine 150 mg administered the night before and on the morning of surgery. Standard ASA monitors (ECG, non-invasive blood pressure, pulse oximetry) and bi-spectral index (BIS) electrodes were applied in the operating room. Anaesthetic induction was standardised using intravenous fentanyl 1 μg/kg, followed by preoxygenation with 100% oxygen for three minutes. Propofol (1.5-2.5 mg/kg) was used for induction, and an appropriately sized I-gel supraglottic airway was inserted without neuromuscular blockade. These procedures were conducted under general anaesthesia with inhalational maintenance through a supraglottic airway and systemic opioid analgesia, representing an analgo-sedation approach within a general anaesthesia framework rather than simple procedural sedation.
Maintenance anaesthesia was conducted as follows:
Group S (sevoflurane): sevoflurane at 1 MAC with 40% oxygen and 60% nitrous oxide, titrated to maintain BIS 40-60;
Group I (isoflurane): isoflurane at 1 MAC with 40% oxygen and 60% nitrous oxide, titrated to maintain BIS 40-60.
At skin closure, volatile anaesthetic delivery was discontinued, and nitrous oxide was stopped after 30 seconds. The I-gel was removed once the patients demonstrated spontaneous eye opening and adequate spontaneous ventilation.
Outcome measures
The primary outcome was emergence time, defined as the interval between discontinuation of the volatile anaesthetic and eye opening in response to verbal command. Secondary outcomes were time to I-gel removal, intraoperative haemodynamic changes, duration of PACU stay, postoperative cognitive function assessed by MoCA-B, adverse events, and total inhaled anaesthetic agent consumption extracted from the Dräger Primus workstation log [19] and associated costs.
Statistical analysis
The sample size was estimated to demonstrate non-inferiority in emergence time with a margin (Δ) of 3.2 minutes, assuming a pooled standard deviation of 3.3 minutes, 95% power, and a one-sided α of 0.025, which required 49 patients per group. To account for dropouts, 100 patients were enrolled. The non-inferiority margin was derived from previous studies by pooling the difference in means of emergence times between sevoflurane and isoflurane [10, 20, 21] Data were analysed using SPSS version 25.0 (IBM Corp., USA) and RStudio (R Foundation). Continuous variables are reported as mean ±SD or median (IQR) and compared using an independent t-test or Mann-Whitney U test, as appropriate. A two-tailed p-value < 0.05 was considered statistically significant.
Results
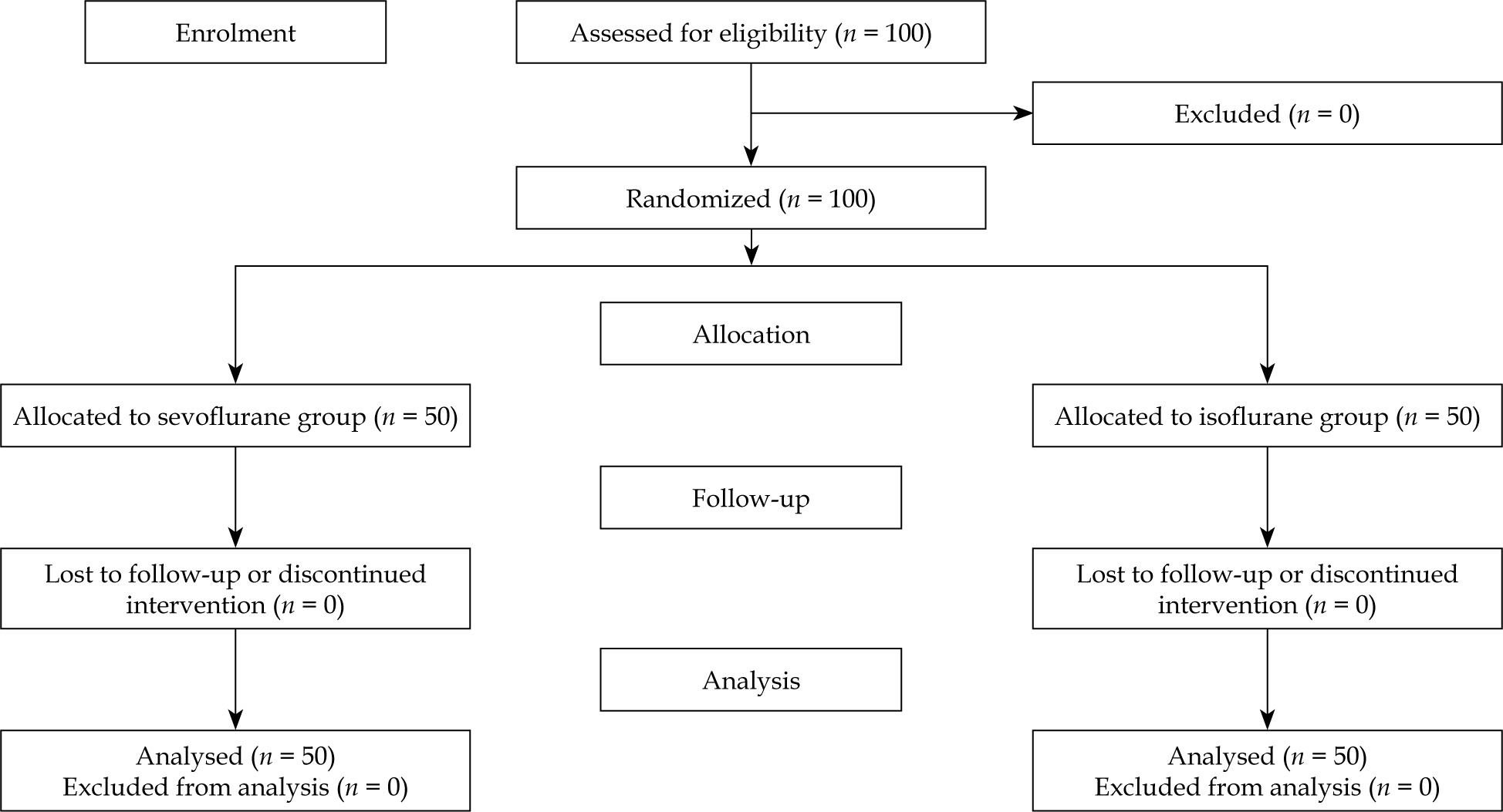
One hundred patients were enrolled and randomized, with no exclusions or dropouts (Figure 1). Equal allocation resulted in 50 patients per group. Baseline demographic and clinical characteristics were well matched between groups (Table 1). Mean age was 56.34 ±6.29 years in Group I and 55.78 ±6.06 years in Group S. Hypertension and diabetes mellitus were the most common comorbidities, without significant intergroup differences. Applicator type and brachytherapy technique were also similar between groups, with no clinically relevant differences in the distribution of intracavitary applications. Disease characteristics and brachytherapy technique were comparable between groups (Table 2). All patients underwent HDR intracavitary brachytherapy for carcinoma cervix, and the distribution of FIGO stages was similar in the isoflurane and sevoflurane arms. The intracavitary technique was used exclusively in both groups, with no interstitial needles, and the proportions of tandem-ring and tandem-ovoid applicators did not differ significantly between groups.
Table 1
Baseline demographic and clinical characteristics of patients
Table 2
Brachytherapy characteristics of the study groups
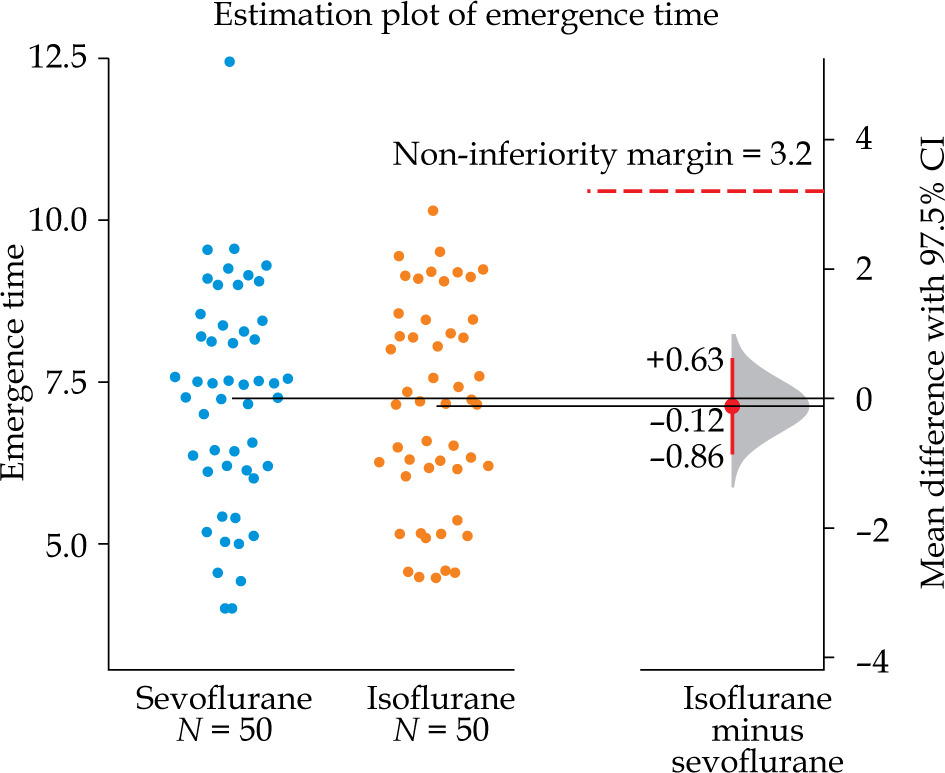
The mean emergence time was 7.13 ±1.60 minutes in Group I and 7.24 ±1.70 minutes in Group S, with a mean difference of −0.12 minutes (97.5% CI: −0.86 to +0.63) (Figure 2). The lower confidence limit did not cross the prespecified non-inferiority margin of 3.2 minutes, demonstrating that isoflurane was non-inferior to sevoflurane. As the confidence interval included zero, no statistically significant difference was observed between agents in terms of emergence time. These findings establish isoflurane as clinically equivalent to sevoflurane for recovery from brief anaesthetic exposures.
Fig. 2
Estimation plot of emergence time: individual val ues for sevoflurane (blue) vs. isoflurane (orange; n = 50 each) with group means; right-hand plot shows mean difference (isoflurane − sevoflurane) −0.12 min (97.5% CI: −0.86 to +0.63) and noninferiority margin (3.2 min, dashed line); noninferiority demonstrated with confidence inter val including zero
Time to I-gel removal was similar between groups (7.28 ±1.61 minutes in Group I vs. 7.49 ±1.83 minutes in Group S; p = 0.554) (Table 3). While the difference in the total volatile agent consumption was small (isoflurane: 4.45 ±0.56 ml/case; sevoflurane: 4.87 ±0.67 ml/case; p = 0.001) (Table 3), the cost disparity was substantial. Analysis of cost per case revealed a striking difference between the two agents. Isoflurane’s average cost was 22.2 ±2.77, whereas sevoflurane’s was 57.8 ±9.35. This difference was statistically significant (p < 0.001, with sevoflurane costing approximately 2.6 times more than isoflurane (95% CI: 2.46-2.76) (Table 3). Postoperative cognitive outcomes showed no differences between groups (Table 3).
Table 3
Primary and secondary outcomes
a Non-inferiority demonstrated: mean difference –0.12 min (97.5% CI: –0.86 to +0.63); margin = 3.2 min, bTwo-sample t test, cMann-Whitney U test, dChi-square test, BIS – bispectral index, MOCA-B – Montreal Cognitive Assessment-Basic, PACU – post-anaesthesia care unit, PONV – postoperative nausea and vomiting
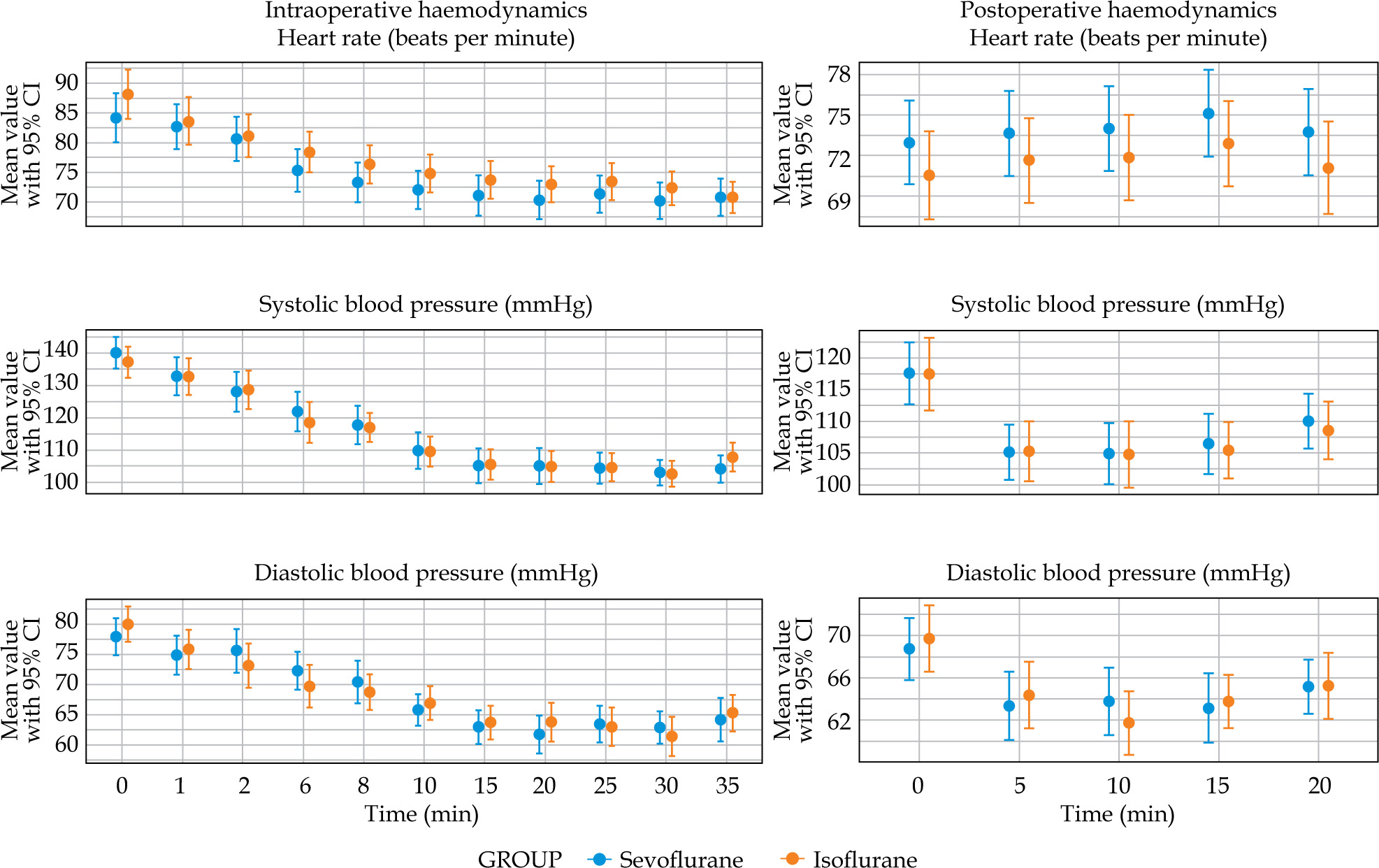
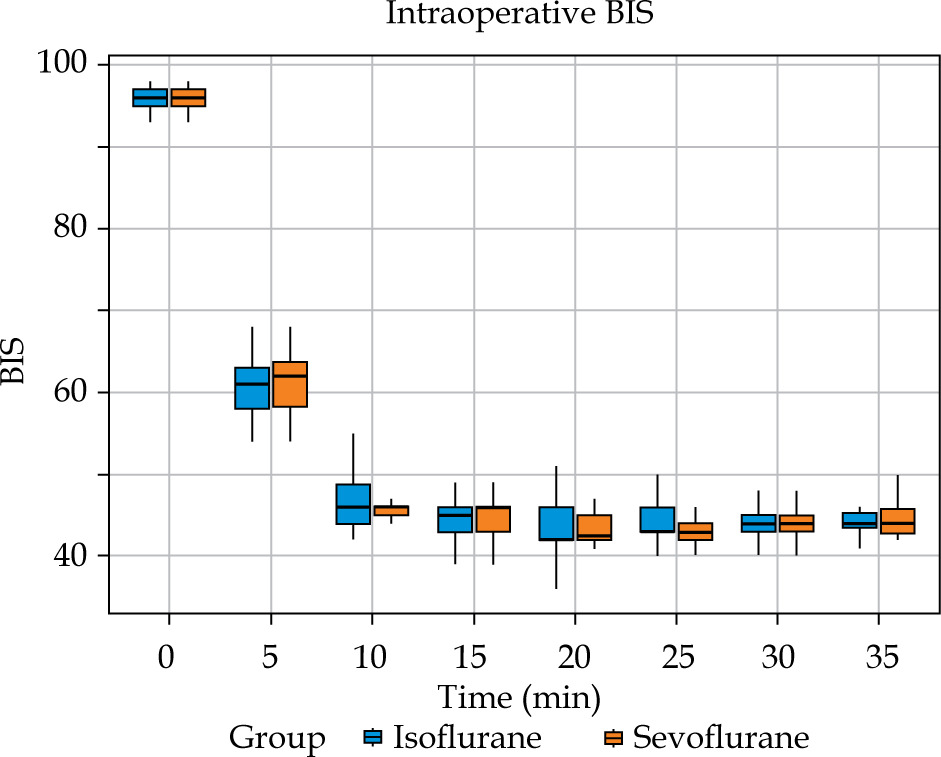
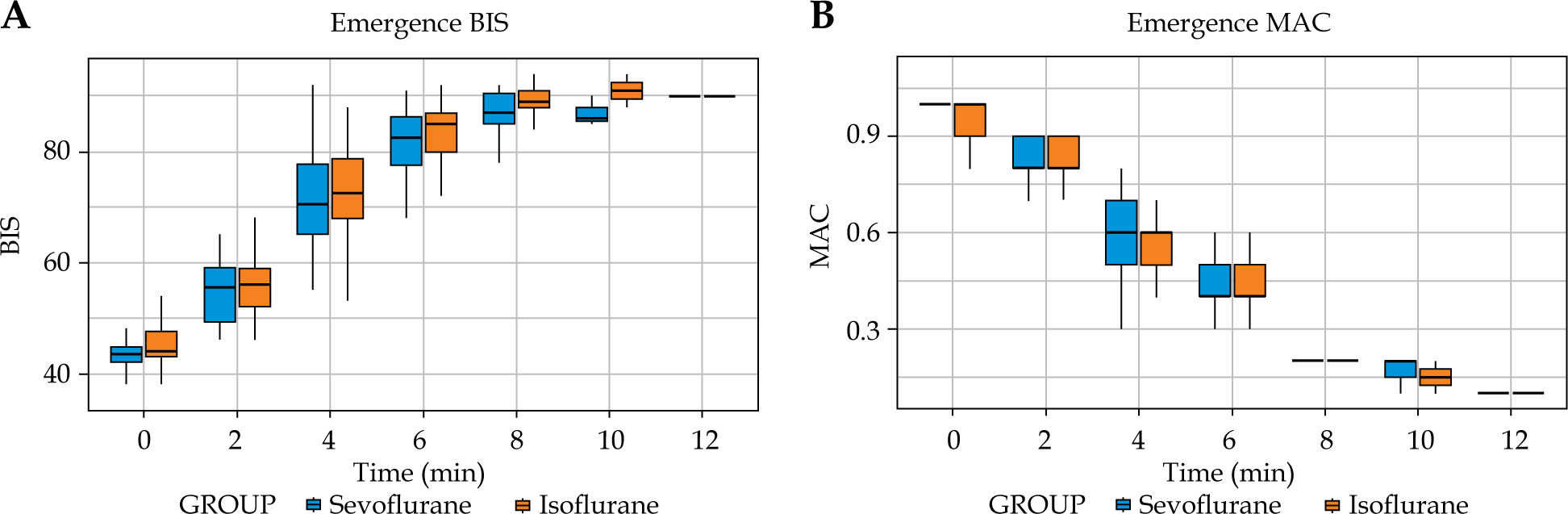
Analysis of intraoperative haemodynamics revealed no significant differences between groups in mean heart rate, systolic blood pressure, or diastolic blood pressure (Figure 3). The depth of anaesthesia was consistently maintained within target BIS limits, with nearly identical proportions of recorded time in the BIS range of 40-60 (85.9% in both groups) (Table 3). Intraoperative BIS values remained equivalent at all time points (Figure 4). During emergence, BIS recovery and MAC reduction did not differ between agents (Figure 5). The incidence of adverse events was low across both groups. Postoperative nausea and vomiting (PONV) occurred in 1 patient (2%) in the isoflurane group vs. three patients (6%) in the sevoflurane group (p = 0.617) (Table 3). No instances of shivering or significant airway complications were observed.
Fig. 3
Intraoperative (0-45 min) and postoperative (0-20 min) haemodynamics: heart rate, systolic BP, and diastolic BP for sevoflurane vs. isoflurane as mean ± 95% CI; no statisically significant intergroup differences
Discussion
This randomised, non-inferiority trial proves that isoflurane is a clinically effective and economically advantageous alternative to sevoflurane for maintenance anaesthesia in women undergoing intracavitary brachytherapy. We demonstrated that isoflurane was non-inferior to sevoflurane in terms of emergence time, with clinically equivalent recovery profiles and comparable outcomes in terms of haemodynamic stability, cognitive recovery, and PACU stay. The typical recovery advantage associated with sevoflurane was not observed in procedures lasting less than 30 minutes, with both agents showing similar emergence profiles.
Multiple studies have consistently shown that sevoflurane offers a faster recovery profile compared to isoflurane [10, 22-26]. This advantage is primarily explained by its lower blood-gas partition coefficient, enabling more rapid washout and emergence. Our observation of clinical equivalence aligns with pharmacokinetic theory and prior work by Chiu et al. [14], suggesting that in brief anaesthetic exposures, differences in brain tissue solubility may supersede blood-gas kinetics [15, 16]. Isoflurane, despite having higher blood-gas solubility, has lower tissue solubility, which may result in reduced accumulation and a more rapid offset when exposure time is minimal.
To our knowledge, no previous investigation has specifically evaluated patients undergoing procedures of approximately 30 minutes within a non-inferiority trial framework. The inhalational anaesthetic concentration was carefully adjusted to maintain BIS values within the target range of 40 to 60, preventing excessive delivery of the inhalational agent. The uniformity in recovery times can likely be attributed to these individualised adjustments. Consistent with our findings, Seitsonen et al. [27] reported that when guided by BIS monitoring, isoflurane and sevoflurane resulted in similar recovery profiles in outpatient gynaecological procedures.
Haemodynamic parameters and depth of anaesthesia remained comparable between the agents throughout the study. Our findings are consistent with prior research, which reported no clinically meaningful differences [6, 27]. No significant differences were noted in postoperative cognitive function or PACU stay duration. This is supported by a meta-analysis of 1,562 patients [22] which found no difference in discharge readiness times. Both groups showed comparable safety profiles, with minimal adverse events observed.
The Dräger Primus consumption display provides reliable measurements of inhalational agent usage [19], enabling pharmacoeconomic assessments. This study highlighted a striking cost disparity: isoflurane was approximately 2.6 times less expensive per case than sevoflurane, corresponding to a 61.6% reduction in cost. This economic advantage becomes particularly relevant in resource-limited and high-volume clinical environments when patient outcomes are equivalent. Our findings corroborate the consistent cost-effectiveness of isoflurane, as documented in earlier studies [22, 28]. Clinical equivalence and substantial cost savings provide compelling evidence for the use of isoflurane in appropriate clinical settings.
Interventional radiotherapy (brachytherapy) is increasingly recognised as a complex [18], multidisciplinary procedure, in which anaesthesiologists play a pivotal role in ensuring patient immobility, comfort, and safety, often in non-operating-room environments [4, 29]. The recently proposed COMIRI (Complexity Index of Interventional Radiotherapy Implants) classification systematically scores brachytherapy procedures by implant type, imaging, and team composition, and explicitly links higher-complexity categories with a greater need for anaesthesiologist involvement [30]. Within this framework, short-duration intracavitary gynaecological brachytherapy, as in the current study, represents a lower-to-intermediate complexity scenario but still requires reliable emergence and efficient turnover; demonstrating that a substantially less expensive volatile agent such as isoflurane can provide non-inferior recovery has direct implications for resource allocation in high-volume interventional radiotherapy centres. This study successfully demonstrated the non-inferiority and clinical equivalence of the intervention using a robust, adequately powered randomised design, thereby achieving its primary objective. Bias was minimised through the use of standardised anaesthetic protocols and blinded outcome assessors. Consistent anaesthetic depth verified by BIS values mitigated investigator bias. The inclusion of cost assessment adds clinical relevance.
The study has several limitations. The single-centre design inherently limits the external validity and generalizability of our findings. The small sample size may have also hindered the detection of subtle effects on secondary endpoints. While patients and outcome assessors were blinded, the unblinded attending anaesthesiologists introduced a risk of performance bias, despite the use of standardised protocols. The cost assessment was also limited, focusing solely on anaesthetic agent costs rather than a comprehensive scope of perioperative resource utilisation. Furthermore, patient satisfaction was not measured, indicating a need for future studies with validated assessment tools. For definitive validation, future multicentre trials with larger cohorts and more expansive economic analyses are warranted.
This study establishes isoflurane as a viable anaesthetic for short-duration brachytherapy, particularly in resource-constrained, high-volume oncology environments. Given its clinical equivalence to sevoflurane, the financial benefits of using isoflurane can directly influence procurement decisions and lead to reduced healthcare costs. This trial provides new evidence on anaesthetic performance in brief procedures, showing that isoflurane allows for prompt emergence and challenges the notion that sevoflurane is always superior for rapid emergence. Our work highlights how procedural duration affects the performance of anaesthetic agents and underscores the need for broader research on cost-effectiveness.
Conclusions
In women undergoing short-duration gynaecological brachytherapy, the demonstrated non-inferiority of isoflurane to sevoflurane with clinically equivalent emergence times offers a significant clinical and economic advantage. Our findings confirm that isoflurane provides similar haemodynamic stability and cognitive function recovery while enabling comparable PACU discharge profiles for procedures under 30 minutes. The profound cost differential between the two inhalational agents positions isoflurane as a highly effective, evidence-based alternative in resource-constrained or high-volume oncology settings.








