
Purpose
Prostate cancer is the most common cancer in men in developed countries. Brachytherapy as monotherapy is recommended by oncological and urological societies in low- and intermediate-risk groups [1, 2]. The incidence of local prostate cancer recurrences after monotherapy with high-dose-rate brachytherapy (HDR-BT) in all risk groups is very low, estimated at approximately 5% [3]. However, in highly-specialized oncological centers that treat a high number of patients with HDR-BT, a cumulated number of local recurrences during follow-up is naturally observed. Treatment of this group of patients is challenging, as no unequivocal guidelines are available. In case of biochemical recurrence of prostate cancer treated primarily with radiotherapy, treatment with hormonotherapy is accurate. It is known that long-term, and in those cases, life-time hormonotherapy, may lead to sequelae, such as bone loss, metabolic changes, gynecomastia, loss of muscle tissue, hot flashes, and higher incidences of cardio-vascular events [4]. The critical issue is that the treatment is not aimed at fully curing the disease. In most cases, resistance to hormonal blockade occurs, leading to the disease’s progression. In cases of local recurrences after external beam radiotherapy (EBRT) or monotherapy with low-dose-rate brachytherapy (LDR-BT), salvage treatment aims at curing in selected patients. It is possible to use salvage HDR-BT, LDR-BT, or salvage prostatectomy (SRP), previously described in reviews concerning this topic [5, 6]. On the other hand, there are no articles concerning salvage prostatectomy for locally recurrent prostate cancer after monotherapy with HDR-BT, and a report about secondary HDR-BT contains only results of patients treated with an insufficient dose of 1 × 19 Gy [7].
LDR-BT with iodine-125 (125I), which has an average energy of 28 keV, is characterized by higher linear energy transfer (LET) of radiation generated by this element in comparison with radiation generated with HDR-BT, which may be directly linked to higher relative biological effectiveness (RBE) [8, 9]. The given 125I characteristic results in different than other forms of radiotherapy radiobiological mechanisms of cancer cell damage. LDR-BT may be an effective treatment for locally recurrent prostate cancer primarily treated with HDR-BT [10]. This is the basis of our department’s approach to propose salvage 125I LDR-BT to selected patients with local recurrence, who were previously treated with monotherapy HDR-BT. This retrospective study aimed to present early results of the new concept of treatment as well as filling the gap in the literature regarding local recurrences after HDR-BT monotherapy.
Material and methods
Nine patients with low- and intermediate-risk prostate cancer, with a median age of 71 years (range, 59-82 years) were diagnosed with local recurrences after previous monotherapy HDR-BT, 3 × 10.5 Gy scheme with 7 to 14 days of the intra-fraction brake. Primary treatment occurred in the regional cancer center between March, 2010 and August, 2013. Median time to biochemical recurrence (Phoenix definition) [11] after primary treatment was 59 months (range, 21-80 months). Subsequently, in case of radiological recurrence in magnetic resonance imaging (MRI, n = 7) or positron emission tomography (PET-CT, n = 2), the patient had a prostate biopsy performed to confirm a recurrence (Table 1).
Table 1
Patients’ characteristics
[i] ADT – androgen deprivation therapy, BF – biochemical failure, iPSA – initial prostate antigen level, ISUP – International Society of Urological Pathology (ISUP) grading of prostate cancer, GS – Gleason scale, m – months, LR – local recurrence, Mets – clinical failure outside the prostate, n – number of patients, TNM – tumor nodal staging UICC 8th, rPSA – highest PSA level before salvage treatment, * Wilcoxon test
The absence of distant metastases was confirmed by choline PET in 7 cases, including two patients with a prostate recurrence diagnosed solely by this diagnostic modality. PET with choline was performed in 6 cases, and PET-PSMA in one patient. In the other two cases, dissemination of disease was excluded based on PSA kinetics, computed tomography (CT), MRI, and bone scan. Three of the patients had ADT with LHRH analog before salvage treatment in castration-resistance condition. Stage was assessed with MRI in 7 cases, and TRUS in the other two subjects. TNM was applied for recurrence staging (Table 1), and urological symptoms were assessed using International Prostate Symptoms Scale (IPSS). Each patient was qualified to salvage brachytherapy by the multidisciplinary committee, and signed an informed consent to undergo brachytherapy re-treatment. All presented data were obtained retrospectively, and according to recommendation of the local bioethics commission, the results have no features of a medical experiment.
Procedure
All patients were treated with salvage LDR-BT monotherapy between 2016 and 2019. Prescribed dose was 145 Gy to the prostate capsule.
Treatment was performed under general anesthesia using 125I (Eckert & Ziegler BEBIG® stranded seeds Isocord®), trans-rectal ultrasonography (BK Medical Pro Focus 2202), and sonographic planning of oncology treatment (SPOT Pro 3.1, Nucletron, an Elekta company, Elekta AB, Stockholm, Sweden). From 2018 on, the treatment was performed using BK Medical Pro Focus 3000 trans-rectal ultrasonography and OncentraProstate v. 4.1 (Elekta Company, Elekta AB, Stockholm, Sweden) planning system.
Dose was specified for the prostate capsule and cancer infiltration during the procedure. In 4 cases, margin of 2-3 mm was added to create clinical target volume (CTV). Dose constraints for CTV were V100 (volume of CTV covered with 100% of the total dose) > 95% (90% acceptable), and V150 (respectively) < 50% (55% acceptable). Dose constraints for organs at risk were D10 for urethra (dose in 10% of the most irradiated volume of organ) < 160%, and D0.1cc (the highest dose in 0.1 cc of organ) for rectum < 100% of the total dose. Dosimetric verification with CT was performed the day after the application of seeds with a catheter present in the urethra, and without a catheter after one month and six months.
Follow-up
All patients received a prescription for tamsulosin 0.4 mg once daily after the procedure to reduce treatment toxicity. After treatment, patients were followed in the outpatient clinic one month after discharge, then every three months for six months, and every 3-6 months depending on symptoms and preference. Voiding symptoms were assessed on each control visit using IPSS questionnaire. Other urological symptoms, toxicity, and gastrointestinal indicators were retrospectively evaluated based on patients’ records following CTCAE v. 4.0 scale [12]. In case of biochemical failure (Phoenix definition) or clinical recurrence, ADT was initiated as well as any symptomatic treatment if needed [11].
Statistics
Data was collected using MS Excel, which was also applied to obtain various descriptive statistics. Further tests and figures were made using Statistica v. 13 (Statsoft, Tulusa, USA). Wilcoxon signed-rank test was applied to compare paired variables. Kaplan-Meier analysis was done for survival evaluation. P-values below 0.05 were considered statistically significant. The number of cases was low, but enough for the tests used. However, in terms of the number of cases and retrospective nature of the study, the results of statistical analysis should be considered with cautiousness.
Results
Staging
In the analyzed group, rT2a (recurrence TNM stage) occurred in 3 cases, rT2c in 3 cases, rT3a in 2, and rT3b in one patient. A significant rise in the TNM stage was observed (p = 0.01, Table 1). The mean level of PSA before salvage treatment (rPSA) was 6.3 ng/ml (range, 2.3-11.14 ng/ml). Additionally, a significant rise in Gleason score was observed. The second histopathological records showed 3+3 (ISUP 1) in one case, 3+4 (ISUP 2) in 2 cases, 4+3 (ISUP 3) in 2 cases, and 1 case of 4+4 (ISUP 4), 3+5 (ISUP 4) as well as of 4+5 (ISUP 5) (p = 0.04, Table 1).
Dosimetry
A plan from implant day is presented in Table 2. Moreover, the recommended dosimetry was performed one month (range, 4-6 weeks) after the application. The mean V100 was 91.9% (range, 89.3-96.7%), and the mean V150 was 47.5% (range, 42.3-60.3%, Table 2). The mean D10 in the urethra was 134.6% (range, 123.6-151%). The D0.1cm3 in the rectum was 99.6% (range, 64.8-148.5%), the D2cm3 was 60% (range, 40-75%), and the D1cm3 in the bladder was 63.5% (range, 45.2-79.2%, Table 2).
Table 2
Dosimetry of salvage low-dose-rate brachytherapy
[i] CTV – clinical target volume, D0.1cc – dose in 0.1 cm3 of the rectum in % of PD, D1cc – dose in 1 cm3 of the blader in % of PD, D10 – dose in 10% of the urethra in % of the prescribed dose (PD); D2cc – dose in 2 cm3 of the rectum in % of PD; D30 – dose in 30% of the urethra in % of PD, D90 – dose in 90% of CTV in % of PD, V100 – % of the volume of CTV covered with 100% of PD, V150 – % of the volume of CTV covered with 150% of PD, V200 – % of the volume of CTV covered with 200% of PD 145 Gy, *only seven cases were analyzed because two dosimetry data were lost after planning system update
Clinical outcomes
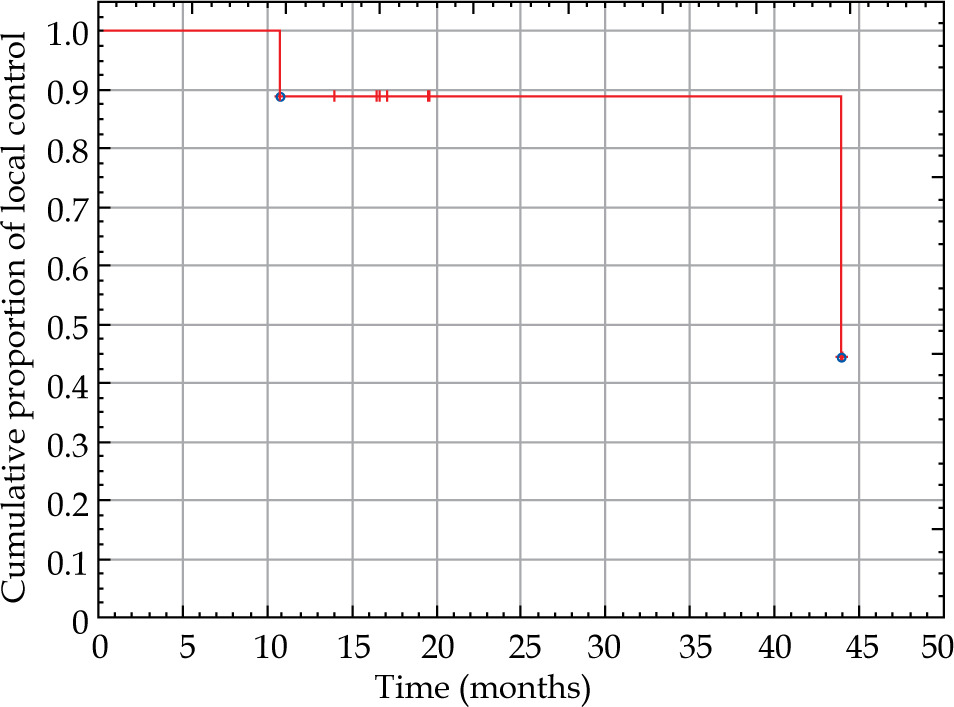
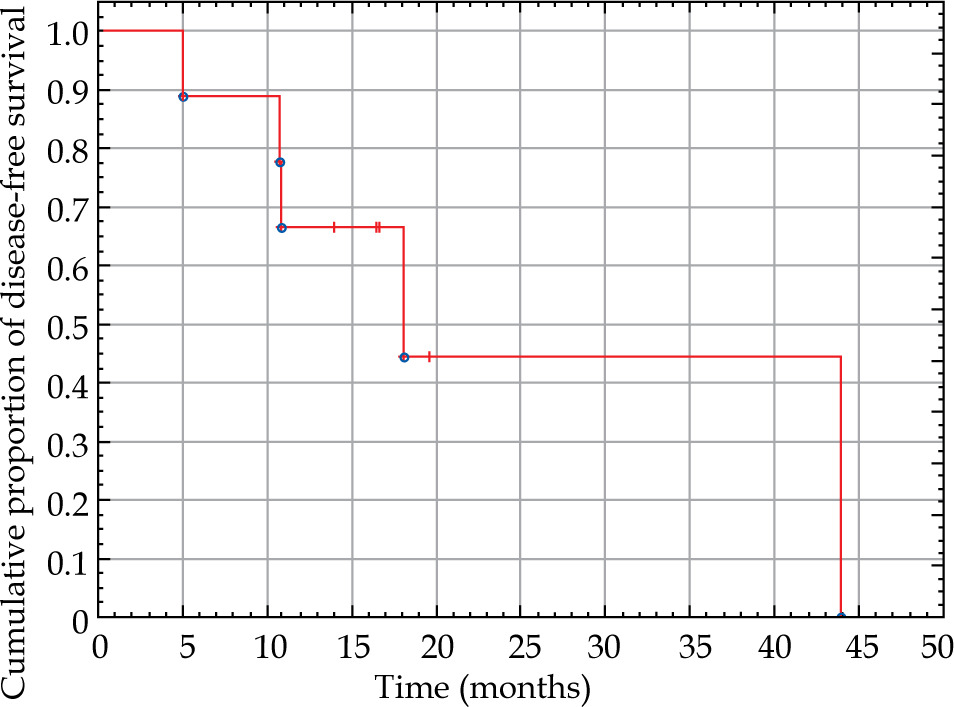
The median follow-up was 30 months (range, 17-63 months), and local recurrences were detected in 2 cases. The actuarial 2-year local control was 88% (Figure 1, Table 1), and distant metastases were observed in 2 patients. A local recurrence was observed after ten months in patients who initially were considered low-risk patients. First recurrence occurred as the invasion of seminal vesicles (T3b) and Gleason 3+5. Second local recurrence was diagnosed after 45 months in initially considered intermediate-risk patient, but the recurrence was T2c and Gleason 4+5. The patient had a distant metastasis as well. In one case, only distant metastases were diagnosed. Biochemical failure without any other sign of clinical recurrence was observed in 2 cases (22%). Four patients had no biochemical and clinical failure of the disease. The 2-year disease-free survival (DSF) was 58.3% (Figure 2, Table 1).
Toxicity
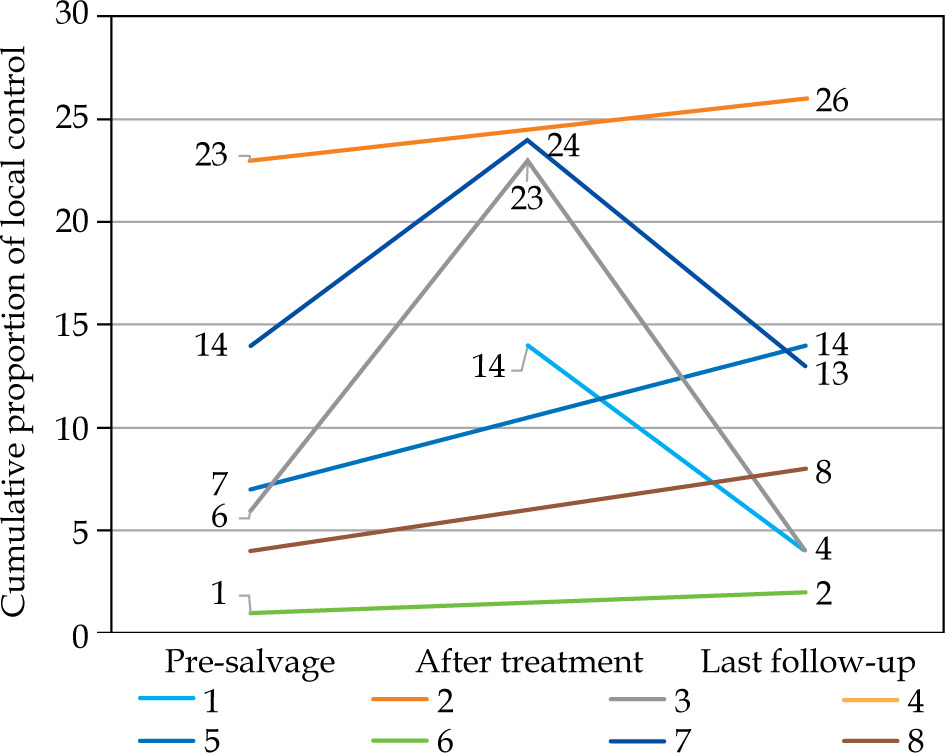
Before salvage treatment, the patients after primary HDR-BT presented a median of 6.5 points (range, 1-23 points) of urological symptoms on IPSS scale. Data were available in records of 66% of cases (n = 6). One patient had been receiving hemodialysis for many years, and since he was producing only trace amounts of urine, the intensity of his urological symptoms was not assessed. In the other two patients, there were no data on IPSS scores in medical history. At the first follow-up visit after one month, the mean IPSS score was 20, and at the last follow-up visit, it was 8 points (range, 1-26 points); IPSS was assessed for the whole group. There was no significant change in the IPSS scale before and after treatment (p = 0.68, Figure 3). Urinary retention occurred in one case, and trans-urethral electro-resection was necessary at ten months after salvage LDR-BT (grade 3 toxicity according to CTCAE v. 4.0). In histopathological record, the residual disease was described, and in this case, the patient had a salvage LDR-BT in stage T3b and ISUP 5. Voiding symptoms were caused most likely due to cancer infiltration rather than treatment. Currently, the patient receives ADT treatment and continues his follow-up visits with no significant symptoms. In all other cases, urological toxicity was not higher than 2 in CTCAE v. 4.0 assessment. Two patients had grade 1 toxicity from the gastrointestinal tract according to CTCAE v. 4.0, which in both cases was reported at the first follow-up visit, one month from treatment, and were also present at the last follow-up visit. No other toxicity from the gastrointestinal system was reported, which shows that the treatment was well-tolerated regarding gastrointestinal toxicity.
Fig. 3
The graph presents IPSS scale of each patient. One patient was excluded because of chronic kidney disease and lack of urine production. Case 1 was not assessed before treatment. Cases number 2, 4, 5, 6, and 8 were not assessed on the first follow-up visit after treatment. However, any severe side effects were not mentioned during the visit in the medical history report. There was no difference between pre-salvage and last follow-up in IPSS scale (p = 0.91, Wilcoxon test)
Discussion
Re-irradiation after HDR-BT is controversial, probably due to the aspect that the primary treatment is highly hypofractionated. On the one hand, clonogenic cells responsible for recurrence are considered to be highly radio-resistant. In contrast, despite small volumes of healthy tissue irradiated with a high fraction dose during primary treatment, there is a significant risk of acute and late toxicities. As mentioned, the radio-resistance of cancer cells is multifactorial and not yet fully known process. However, it is believed that the main mechanism of radio-resistance is overexpression of ATM gene (ataxia-telangiectasia mutated), which leads to overproduction of H2AX protein and intensified repair of double-strand brakes (DSBs) caused by re-irradiation [13, 14]. An exciting and rarely discussed fact is that in the case of low- and very low-dose-rates of irradiation, the so-called ‘inverse dose rate effect’ took place and was first observed in the seventies of the last century. Fewer cells survive in similar cell lines when irradiated with a lower dose-rate [15]. In the case of LDR-BT with 125I, with initial mean radiation energy of 28 keV, this effect may occur due to many factors. As already mentioned in the introduction, one of them is a higher LET of X radiation generated by this element, which directly leads to its higher RBE [8, 9].
Additional advantages of re-irradiation with LDR-BT are different radiobiological processes, including absence of proliferation stop of cells in G1/S control point (which leads to cells going through further phases of the cellular cycle), the consequence of longer irradiation time may be, in this case, accumulation of cells in radiosensitive G2/M control point [10], much more efficient production of final products of the lipid peroxidation after biological membranes irradiation [8], significantly higher effect of membrane Na/K-ATP enzyme inactivation [9], and what is the most important in the context of re-irradiation, an absence of ATM kinase activation, thanks to which, DSBs induced by low-dose-rate radiation are ‘invisible’ to repair systems of cell [16]. Moreover, in the case of 125I, dose intensity is reduced more rapidly than with a quarter of the distance [17], which, similarly to increased repair of sublethal damage in healthy tissue exposed to prolonged irradiation, may reduce toxicity of treatment [18].
On the other hand, in the linear-quadratic model of LDR-BT, an intensive decrease of biologically effective dose (BED) is observed in case of high α/β of tumors [19-21]. The prostate α/β ratio is low, and even 1.55 Gy [20-22]. Aggressive tumors have higher proliferation than low Gleason score cancers. The proliferation influences the α/β ratio because of its definition. In a study of Proust and Lima, there was a discussion that cancers with high Gleason scores could have a higher α/β ratio. The α/β ratio for Gleason > 7 was around 14 Gy in the sub-group analysis. However, the hypothesis was not statistically significant in this study. The study analyzed the PSA response as an endpoint, and cancers with high Gleason scores more often did not release PSA compared with less aggressive cancers, which was minority in the group [22]. These facts could affect the analysis and make the results not significant. In our study, the observation time was too short to conclude treatment effectiveness fully. However, we observed more recurrences of aggressive and rapidly dividing tumors, e.g., ISUP 4-5/Gleason 9-10, but actuarial 2-year local control was 88% for all the patients (Figure 1).
In clinical practice, re-irradiation with modern LDR-BT has been used for many years. First data was presented by Wong et al. in 2006, where seventeen patients, primarily treated with EBRT with doses from 64.8 Gy to 70.2 Gy, with a pre-salvage PSA level of 4.7 ng/ml, were given salvage treatment with LDR-BT (total dose, 126 Gy). Despite the low total dose of EBRT, grade 3 toxicity was observed in 41% of patients [23].
In several articles regarding salvage brachytherapy, groups of subjects who previously had received HDR-BT were analyzed. However, those were only HDR-BT boost after EBRT. In Wojcieszek et al. study, 83 cases were analyzed, of which 61% were primarily treated with EBRT only and 31% with EBRT (54 Gy), with HDR-BT boost (1 × 10 Gy). Salvage treatment was HDR-BT in 3 fractions, 10 Gy each. Retrospective analysis showed that five-year DFS was 67%, with a median follow-up of 3.4 years. Grade 3 or higher toxicity was observed in 13% of cases [24]. In addition, one patient previously treated with BT-HDR was reported in the phase I trial of Nguyen et al. in 2007 as well as in the work of Kollmeier et al. in 2017. In both cases, it was a boost after EBRT [25, 26]. There was no information if any patient with primary HDR-BT treatment, as in our group, was enrolled [25, 26].
Outcomes of salvage treatment after primary HDR-BT monotherapy were presented by Maryata et al. in 2021. Twelve patients treated previously with 1 × 19 Gy scheme were presented [7]. Patients were enrolled in phase II prospective trial, and had histopathologically confirmed prostate cancer recurrence [27]. In contrast to our group, they were given salvage treatment with HDR-BT, two fractions of 12 Gy each. A decrease in PSA was observed in 90% of cases. Grade 1 or 2 acute urological toxicity was reported in 4 patients (33%), and late in 2 patients (16.7%). There was no gastrointestinal toxicity. Two biochemical recurrences were reported during a median follow-up of 26 months [7].
All analyzed reports did not show outcomes of salvage treatment with LDR-BT after recommended HDR-BT monotherapy scheme, which makes our report unique. Presented radiobiological basics of LDR-BT suggest that prospective trial in patients previously treated with HDR-BT monotherapy or after very high fraction doses (e.g., SBRT) is justified. Our findings showed that this treatment seemed to be well-tolerated with acceptable urological toxicity of grade 2 or less in 87% and gastrointestinal in 100% of patients.
Assessment of the effectiveness of LDR-BT after HDR-BT was not the goal of our report, and the presented outcomes are preliminary. Local control of 88% is promising. However, DFS was 57% with a 30-month median follow-up. It should be noted that our group, with a local stage (33% ≥ T3a) and histopathological diagnosis (33% ≥ ISUP 4) deviates from the present recommendations of qualification criteria to salvage treatment [6]. In 2 of the patients, the local stage was assessed with TRUS, not MRI. Furthermore, 3 of the patients (33%) had castration-resistant prostate cancer at the time of salvage LDR-BT. First had biochemical recurrence without clinical recurrence, and the second had biochemical recurrence with local failure. The third patient had no evidence of disease without androgen deprivation therapy. Despite that, the authors believe that LDR-BT salvage treatment after primary HDR-BT may be a good alternative for well-selected patients.
The main limitation of this report is its retrospective nature and the lack of various data. However, we believe that the reported patient group is unique, therefore the results should be presented to the medical society.








