
Introduction
Crohn’s disease (CD) is a chronic inflammatory bowel disease (IBD) characterized by transmural inflammation. The utility of magnetic resonance enterography (MRE) for active inflammatory disease evaluation in children and adolescents with IBD was demonstrated in a recent meta-analysis [1]. MRE was included as the diagnostic tool for assessment of the small bowel in the Revised Porto Criteria (2014) by the Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) [2]. Studies referring to MRE-based indices in adults have been previously reviewed [3]; however, data obtained in the paediatric population have not yet been compiled.
The aim of this paper is to review the developments in MRE-based CD activity indices in paediatric patients and to sum up their diagnostic performance in children.
Methods
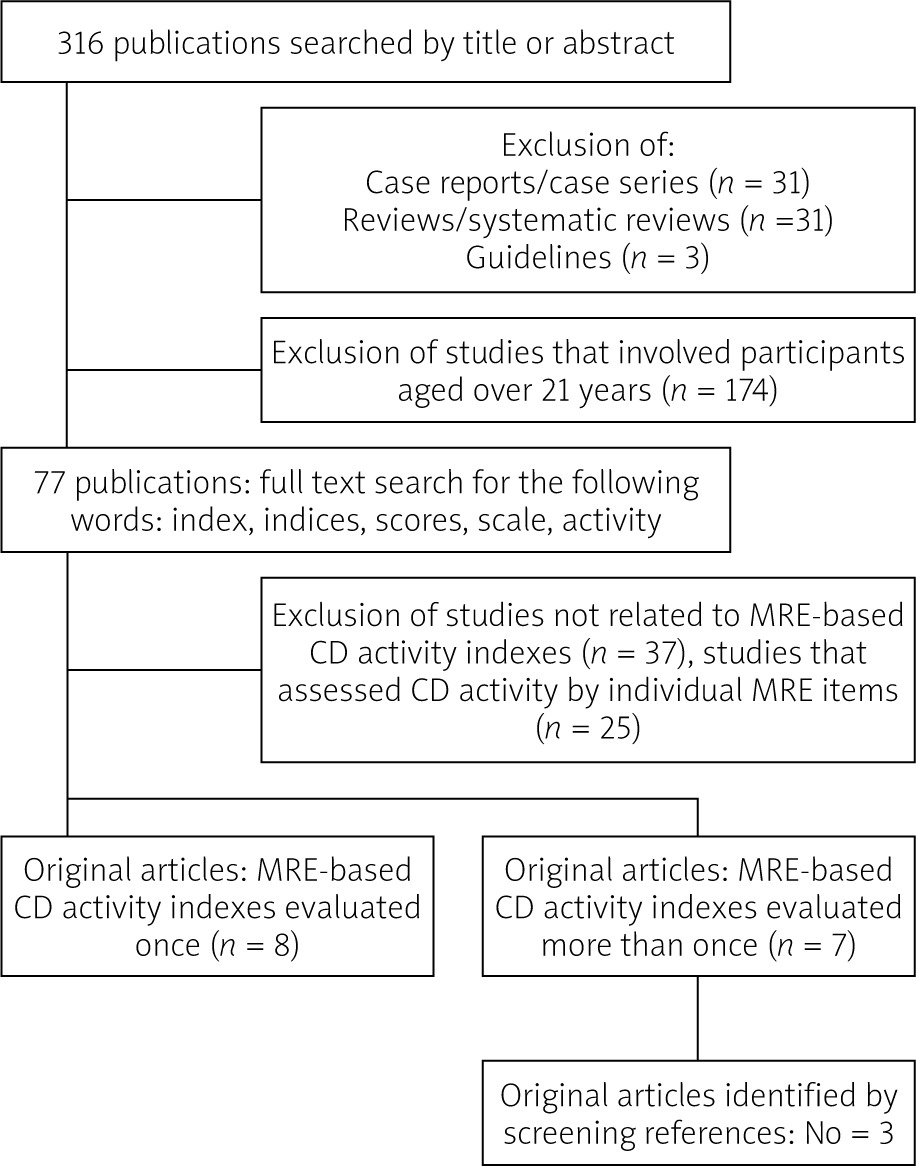
A literature search of the PubMed database (January 2008 – November 2021) was performed to review the developments in MRE-based CD activity indices in paediatric patients (Figure 1). The following MESH terms: (Magnetic Resonance Imaging) AND (Crohn’s disease) as well as the following advanced filters: English, Child: birth–18 years, Infant: birth–23 months, Child: 6–12 years, Infant: 1–23 months, Preschool Child: 2–5 years, Adolescent: 13–18 years were applied. In the first phase (searching by title and abstract), case reports, case series, reviews, and guidelines were excluded. In the second phase, full text screening for words such as (index) or (indices), (score), (scale), and (activity) was performed, and papers that did not refer to MR-based CD activity indices were excluded. In the third phase, only indices that were previously evaluated in adults or those that were used more than once in original research papers, but not by the same author, were included in the analysis. Additionally, indices which were dedicated to assessing perianal CD were excluded. The reference list of the articles chosen for inclusion in the analysis was screened to identify other studies for inclusion. The papers finally selected for the analysis were critically evaluated in terms of their diagnostic accuracy and correlation with the following: the Simple Endoscopic Score for Crohn’s Disease (SES-CD) [4], the Paediatric Crohn’s Disease Activity Index (PCDAI) [5], C-reactive protein (CRP), and faecal calprotectin. Ethical approval and informed consent were not required for this study.
Results
In the first phase, out of 316 studies, 77 papers matched the selection criteria. In the second phase, we found 15 publications that referred to MRE CD activity indices. In the third phase, we excluded the indices that were used only once or those which were not evaluated previously in adults. One score, the Enterography Activity Index (EAI) [6], was excluded because it was used twice by the same author. At the end of the selection process, 10 original research papers were included in the analysis (Figure 1). Four MRE scoring systems were reviewed: the Magnetic Resonance Index of Activity (MARIA), the Crohn’s Disease Magnetic Resonance Imaging Index (CDMI), the Magnetic Resonance Enterography Global Score (MEGS), and the Visual Analogue Scale (VAS). The MARIA, MEGS, and VAS were evaluated against the SES-CD (Table I) [7–16].
Table I
Summary of main results
| Reference | Index | Main results |
|---|---|---|
| Kang et al. [7] 2017 No. of patients: 17 Type of article: Prospective | MARIA |
|
| Pomerri et al. [8] 2017 No. of patients: 32 Type of article: Retrospective | MARIA MEGS | |
| Weiss et al. [9] 2019 No. of patients: 175 Type of article: Prospective | VAS and MARIA |
|
| Weinstein-Nakar et al. [10] 2018 No. of patients: 151 Type of article: Prospective | VAS and MARIA | |
| Lee et al. [11] 2020 No. of patients: 30 Type of article: Retrospective | CDMI |
|
| Radhakrishnan et al. [12] 2020 No. of patients: 24 Type of article: Retrospective | CDMI and MEGS | |
| Cococcioni et al. [13] 2021 No. of patients: 25 Type of article: Retrospective | CDMI | |
| Zheng et al. [14] 2020 No. of patients: 52 Type of article: Retrospective | MEGS |
|
| Barber et al. [15] 2016 No. of patients: 15 Type of article: Retrospective | MEGS | |
| Barber et al. [16] 2018 No. of patients: 20 Type of article: Retrospective | MEGS |
[i] MARIA – Magnetic Resonance Index of Activity, CDMI – Crohn’s Disease Magnetic Resonance Imaging Index, MEGS – Magnetic Resonance Enterography Global Score, VAS – visual analogue scale, PCDAI – Paediatric Crohn’s Disease Activity Index, SES-CD – Simple Endoscopic Score for Crohn’s Disease, MH – mucosal healing, CRP – C-reactive protein, AUROC – area under receiver operating characteristic curve, CI – confidence interval.
Magnetic Resonance Index of Activity (MARIA)
The first analysed index, the Magnetic Resonance Index of CD Activity (MARIA), was created in 2009 by Rimola et al. for adult patients [17]. As a reference standard, the researchers used ileocolonoscopy assessed by the Crohn’s Disease Endoscopic Index of Severity (CDEIS) [18]. Radiological assessment was based on changes in MRE images observed prior to and after intravenous contrast administration. The global and segmental MARIA scores are represented by the following formulas:
The global and segmental MARIA score is recommended by the ECCO-ESGAR Guidelines for Diagnostic Assessment in adult IBD [19]. MARIA was also evaluated in the paediatric population. Pomerri et al. [8] were the first to assess the accuracy of MARIA and MEGS. As their reference standard, they used PCDAI. They found that global MARIA showed weak-to-moderate correlation with PCDAI. In 21 patients, they assessed the correlation between global MARIA and SES-CD, which was moderate to strong [8]. In the multicentre clinical project (ImageKids) sub-study, moderate correlations were found between ileal MARIA sub-score and SES-CD as well as between global MARIA and SES-CD. The authors concluded that MARIA can be used to impute the ileal simple endoscopic score of CD in paediatric patients in whom ileal intubation was not achieved. They proposed the following regression model: CD ileum = 1.145 + 0.169 × MARIA ileum rounded to the nearest whole number [9].
MARIA was also used to monitor treatment response in children with luminal moderate-to-severe CD. Kang et al. showed that after 1 year of treatment with combined immunosuppression (infliximab (IFX) and azathioprine (AZA)), delta MARIA correlates with delta SES-CD (R = 0.817, p < 0.001) [7]. Moreover, delta MARIA correlates with delta CRP, erythrocyte sedimentation rate (ESR), and albumin values [7].
MARIA is the best validated MRE-based CD activity index, but it also has significant limitations in the paediatric population. Firstly, it requires peroral and rectal preparation. In paediatric studies, rectal preparation was not performed, which is understandable because an additional water enema in children can significantly jeopardize the feasibility. However, avoiding rectal enema resulted in low correlation between MARIA and SES-CD in the per segment analysis [8, 9]. Secondly, MARIA requires the use of gadolinium contrast to assess relative contrast enhancement of the intestinal wall. Moreover, MARIA does not evaluate the entire small bowel, nor does it take into account extraintestinal complications. In the assessment of the therapeutic response, normal segments contribute to the global MARIA score, while resected segments cause underestimation. Because of these limitations, and with the increasing use of diffusion-weighted imaging (DWI) in radiological evaluation, a modification of MARIA index, called the Simplified Magnetic Resonance Index of Activity (MARIAs) for CD, has recently been developed and validated in adults. This index provides an accurate tool (high correlation between MARIAs and CDEIS: R = 0.83; p < 0.001) for identifying patients’ response to therapy, a tool which does not require paramagnetic contrast. However, the validity of the simplified MARIA in children is yet to be established [20].
Crohn’s Disease Magnetic Resonance Imaging Index (CDMI)
In 2012, Steward et al. proposed the Crohn’s Disease Magnetic Resonance Imaging Index (CDMI). This index was evaluated against pathology, and in adults it showed sensitivity of 81%, specificity of 70%, and AUROC of 0.77 for predicting acute inflammation [21]. CDMI is calculated using the following formula: CDMI = 1.79 + 1.34 × mural thickness + 0.94 × mural T2 score.
In the study of Lee et al., the CDMI score significantly differed between children with active and inactive CD. This study revealed also a weak-to-moderate correlation between endoscopic findings and CDMI (R = 0.42; p < 0.05), although the endoscopic findings were evaluated with the help of a scoring system other than SES-CD [11]. The correlation between CDMI and PCDAI was estimated in 2 studies, and their results were similar: (R = 0.661; p = 0.0004) and (R = 0.656; p < 0.01) [11, 12]. Cococcioni et al. showed a negative correlation between terminal ileum motility and CDMI [13]. Despite its simplicity, CDMI requires peroral preparation and contrast administration. The main limitation of CDMI may stem from the fact that it was designed to evaluate active CD changes only in the terminal ileum and not in the entire small bowel. What is more, CDMI does not include extraintestinal manifestations.
Magnetic Resonance Enterography Global Score (MEGS)
The Magnetic Resonance Enterography Global Score (MEGS) is based on the CDMI. It was designed to better evaluate the extent of the disease. Calculating the global MEGS score is far more complicated than CDMI. It requires summing segmental MEGS scores for each of the 9 gastrointestinal segments (jejunum, ileum, terminal ileum, cecum, ascending, transverse, descending, sigmoid, and rectum) [22].
Several studies evaluated the associations between MEGS and endoscopy in paediatric patients. Zheng et al. validated MEGS against SES-CD and showed that MEGS has a strong correlation with SES-CD. The diagnostic accuracy of MEGS for identifying inflammation in the terminal ileum with endoscopy as the reference standard was high [14]. The study by Barber et al. [15] proved that the accuracy in determining the presence of active inflammation on biopsy was comparable for segmental MEGS (specificity 90% (95% CI: 79.5–96.2%) and sensitivity 60% (95% CI: 40.6–77.3%)) and for colonoscopy (specificity 85% (95% CI: 73.4–92.9%) and sensitivity 53.3% (95% CI: 34.3–71.6%)). This study reported that increasing bowel distention did not significantly change the accuracy of detecting active inflammation, although, due to a small number of patients involved, there were large confidence intervals [15]. In another study, Barber et al. [16] showed that the reproducibility of MEGS was poor, both at the segment level and the total patient level. The authors also found a significant positive correlation between MRE and the clinical activity consensus score (R = 0.598, p = 0.0053) [16]. MEGS showed a weak-moderate correlation with PCDAI (R = 0.46; p = 0.007) [8]. There are many advantages of MEGS such as the detection of extraintestinal manifestations and a comprehensive evaluation of the entire gastrointestinal tract including the length of segments affected by the disease, which is claimed to be an important indicator of the total burden of the disease [22]. The main disadvantages of the above-mentioned score involve the requirement of contrast administration and the complexity of calculations, which makes the evaluation of MEGS time-consuming.
Visual Analogue Score (VAS)
The Visual Analogue Score (VAS) is a subjective assessment of the global inflammatory activity shown by MRE at the patient level. In a 2014 conference poster, Focht et al. proposed implementing VAS as an MR-based diagnostic tool to assess CD activity in paediatric patients. However, their results showed low correlation with SES-CD (R = 0.37; p < 0.003) [23]. In the multicentre ImigeKids sub study, VAS was assessed for each bowel section and globally for the entire bowel. The severity of inflammation was assessed on the basis of bowel wall thickness, T1 enhancement, T2 hyperintensity, diffusion-weighted imaging signal, mucosal signs of ulcerations, and mesenterial signs [9]. Another study, conducted by Inbar Weinstein-Nakar et al., also assessed the degree of MRE inflammation using the VAS score. To define transmural healing by VAS, they used the MARIA score as a reference standard. Eventually, the best cut-off for VAS indicating an inactive disease was < 19.5 mm with AUROC 0.84; 95% CI 0.74–0.94. Additionally, the interobserver agreement for the per-segment VAS scoring assessment was high: R = 0.81 (95% CI: 0.78–0.83; p < 0.0000001), and for the entire bowel global assessment it was R = 0.76 (95% CI: 0.65–0.83; p < 0.0000001) [10]. Further use of VAS in CD paediatric patients is a subject of debate.
Discussion
The main drawback of MRE in assessing CD activity is the subjectivity of evaluation. This review revealed that there are not many original papers using MRE-derived CD activity scores in the paediatric population and even fewer comparing different MRE-based indices. There are more publications that evaluate individual MRE signs to assess CD activity [24] than those which evaluate MRE-based scoring systems. MRE-based CD activity scores correlate with endoscopic findings and clinical activity scores. The reviewed indices were designed to be used in adult patients and were not initially dedicated to assessing CD activity in children. The distribution and aetiology of paediatric IBD is different from adult-onset disease, and MRE examination tolerability in children is lower. Moreover, there are reported differences in MRE imaging findings between adult and paediatric populations [25]. At present, there is no preferred paediatric MRE-based CD activity index that would be accepted and approved for better monitoring of paediatric patients, or which could predict disease course and help in clinical decision-making. In response to the increasing demand for more comprehensive MRE measurement methods of CD activity and bowel damage, the multicentre prospective ImageKids study was designed. The ImageKids study aims to construct new MRE-based scoring systems dedicated to paediatric patients: the Paediatric Crohn’s Disease MRE Index (PICMI), the Paediatric MRE Damage Index in Crohn’s Disease (pMEDIC) and the already published Paediatric MRE-based Perianal Crohn’s Disease (PEMPAC) Index. The development of PICMI is underway [9]. It might reduce the frequency of enema and gadolinium contrast use. Unlike the ImageKids study, the other reviewed studies were conducted on relatively small numbers of patients. What is more, there is inconsistency when it comes to the methodology used in the analysed papers, which makes evaluating the capacity of the MRE-based CD activity indices difficult.
Transmural healing is reported to be associated with better long-term outcomes in small bowel Crohn’s disease than mucosal healing alone. In adult patients, CDMI and MARIA were able to reflect the responsiveness to anti-tumour necrosis factor treatment on transmural inflammation and stenotic lesions [26, 27]. MARIA was found to predict mucosal healing in adult patients with a specificity of 85.3% [28]. It is assumed that MRE may be also useful in identifying relapse in clinically asymptomatic patients and therefore in supporting clinicians in decision-making [29]. The results from studies performed on adult populations seem to indicate that, although ileocolonoscopy with histopathological examination remains the gold standard for the evaluation of mucosal healing, the radiological assessment of transmural involvement should also be an integral part of the examination, especially in asymptomatic Crohn’s disease patients on treatment.
Conclusions
The available evidence on MRE-based CD activity indices in children is insufficient, and the small numbers of patients involved in most studies do not allow for definitive conclusions. However, the reviewed results are encouraging. The studies published over the last 13 years showed the advantages of using CD activity indices in children. The reviewed MRE-based indices integrate imaging findings in a systematic and reproducible manner and help to standardize measured outcomes in clinical trials and academic research. They can provide a quantified clinical decision tool for estimating mucosal and transmural healing and therefore be supportive in the decision-making process regarding therapy. There is an urgent need to develop a specific MRE index of activity for the paediatric population.











