

Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease characterised by new bone formation that progressively leads to ankylosis and functional disability [1]. Inflammation and bone formation might be two independent processes in AS. Recently developed drugs including biologic agents ameliorated low back pain in most patients, while improvement of clinical symptoms was not necessarily accompanied by retention of radiologic progression. The functional impairment related with bone formation will eventually have a severe effect on quality of life in these patients.
Promising drugs controlling new bone formation are in urgent demand in the treatment of AS.
The Wnt pathway plays a critical role in the new bone turnover of AS. Dickkopf homologue 1 (Dkk-1), an inhibitory molecule which is a main regulator in the Wingless (Wnt) pathway, is dysfunctional in AS patients [2-6].
MicroRNAs (miRNAs) are a class of 18-24-nucleotide noncoding RNAs that play an important role in modulating gene expression. By binding to target mRNA, miRNAs have been found to regulate a variety of physiological functions and contribute to various diseases, including rheumatic diseases. Our study aims to investigate the altered expression of miRNAs targeting DKK1 in the PBMCs of AS patients and identify potential markers contributing to new bone formation in AS.
Material and methods
Study participants
Twenty AS patients, 20 rheumatoid arthritis (RA) patients, and 20 healthy controls were enrolled in our study. All AS patients in the study, who first visited at Rheumatology Department of our hospitals, fulfilled the modified New York criteria [7]. The enrolled AS patients had spinal involvement and underwent routine treatment of non-steroid anti-inflammatory drugs (NSAIDs) and sulfasalazine. Pelvis, cervical, and lumbar spine X-rays were taken and reviewed independently by two radiologists, for AS diagnosis and mSASSS scoring [8]. RA diagnosis was made according to the 2010 Rheumatoid arthritis classification criteria [9]. All the study protocols and consent forms were approved by the local Ethics Committee. Written permission was obtained from all subjects who participated in the study. Samples from healthy donors were collected from volunteers.
Bioinformatic prediction and database search
Computational miRNA target prediction analyses were carried out using the algorithms mirTarget2 (http://www.microrna.org/microrna/getGeneForm.do), miRanda (http://www.microrna.org/microrna/home.do), TargetScan (http://www.targetscan.org), and PicTar (http://pictar.mdc-berlin.de). “Dkk-1” and “microRNA” were used as keywords in the PubMed search (http://www.pubmed.com) for potential microRNAs targeting Dkk-1.
Quantitative RT-PCR analysis
Quantitative RT-PCR assays were performed according to the manufacturer’s instructions. U6 small nuclear RNA was quantified as a control to normalise differences in total RNA levels. Specific primers of miRNAs selected for real-time PCR were ordered (Applied Biosystems, USA); β-actin was quantified as the control. Real-time PCR condition was 94°C, 5-min denaturing; 50 cycles of 94°C, 15 seconds; 55°C, 30 seconds. The quantitative RT-PCR was performed by using an Opticon-2 Detection System (Applied Biosystems, Carlsbad, CA, USA). All reactions were run in duplicate and repeated three times. A threshold cycle was determined in the exponential phases of amplification, and the comparative threshold cycle method was calculated with 2Δ Δ T and used to calculate the relative gene expression [10]. The value of each control sample was set at one and was used to calculate the fold change in target genes.
Messenger RNA extraction and reverse transcription
Total RNA was extracted from PBMCs using the Trizol method. The purity of RNA was confirmed by the relative absorbance at 260/280 nm ratio using a spectrometer.
RNA was reversed to cDNA by Transcriptor First Strand cDNA kit. For real-time quantitative PCR, 10 μl 2 × SYBR Green Master mix, 0.4 μl primer, 1 μl ROX, 2 μl cDNA, and 6 μl H<sub>2</sub>O were mixed to make a 20 μl reaction volume. Each sample was run in triplicate. Real-time quantitative PCR was performed at 95°C for 10 minutes, followed by 40 cycles at 94°C for 15 seconds, 55-60°C for 15 seconds, and 72°C for 30 seconds.
Ct value of β-actin was used as internal control and compared with that of target gene. The ΔΔCt method for relative quantity was used as previously described to calculate the differences of expression level for each target gene among samples.
Statistical analysis
All statistical analyses were carried out in SPSS version 13.0. Data was presented as mean ±SD. Variables were tested for normality by applying the Kolmogorov- Smirnov test. Independent-samples t test was used for group comparisons. Spearman correlation was conducted, and a dot plot was drawn when applicable. p-values < 0.05 (two tailed) were considered significant.
Results
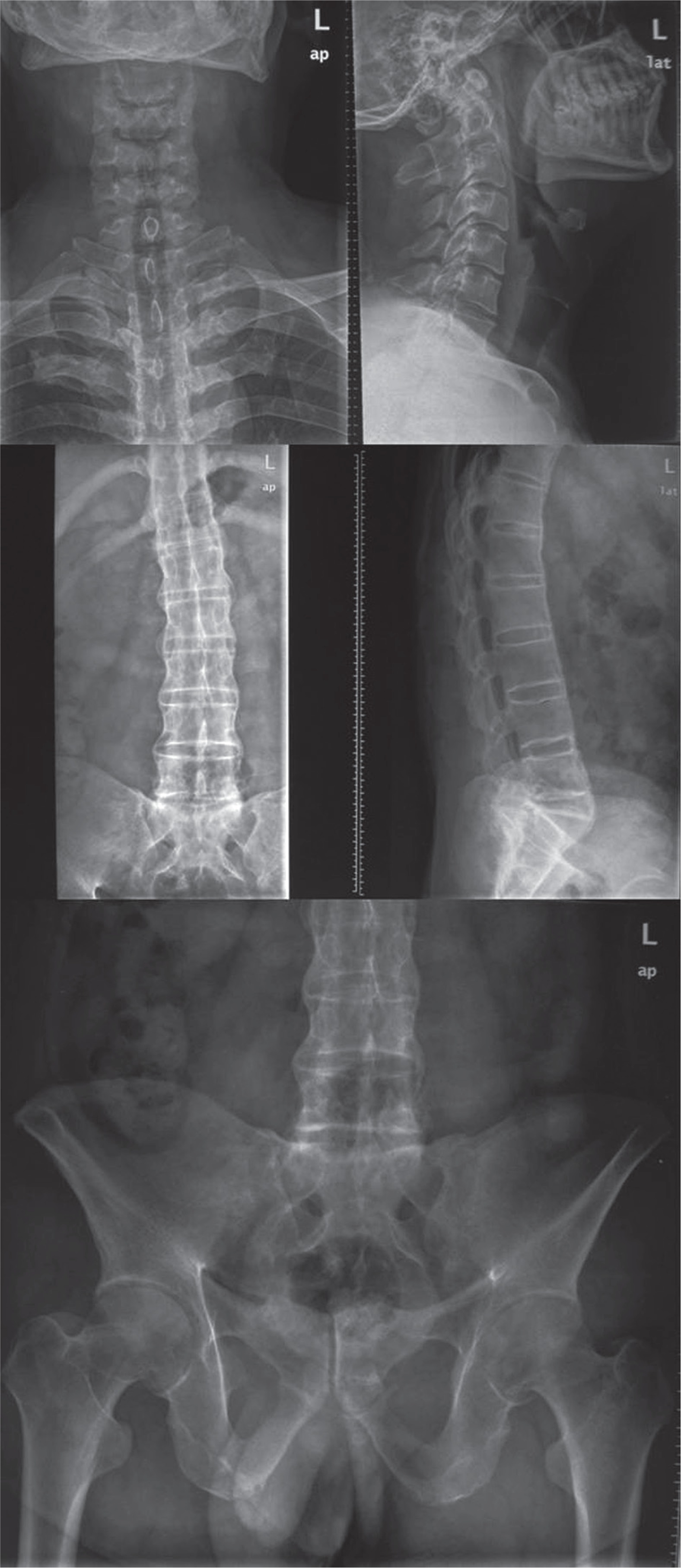
Twenty AS patients and 20 age- and sex-matched healthy controls were included in our study. Characteristics of the study subjects are presented in Table 1. X-ray images showed ankylosis of cervical, lumbar, and spine in the patients (Fig. 1).
Table 1
Characteristics of the study subjects
[i] HLA-B27 – human leukocyte antigen-B27, ESR – erythrocyte sedimentation rate, CRP – C-reactive protein, BASDAI – Bath Ankylosing Spondylitis Disease Activity Index, BASFI – Bath Ankylosing Spondylitis Function Index, mSASSS – modified Stoke Ankylosing Spondylitis Spinal Score, NA – not applicable
Fig. 1
A patient with advanced ankylosis shown in cervical, lumbar, and pelvis X-ray images. Cervical, lumbar, and pelvis X-ray images taken in a patient for diagnosis and mSASSS (modified Stoke Ankylosing Spondylitis Spinal Score) scoring
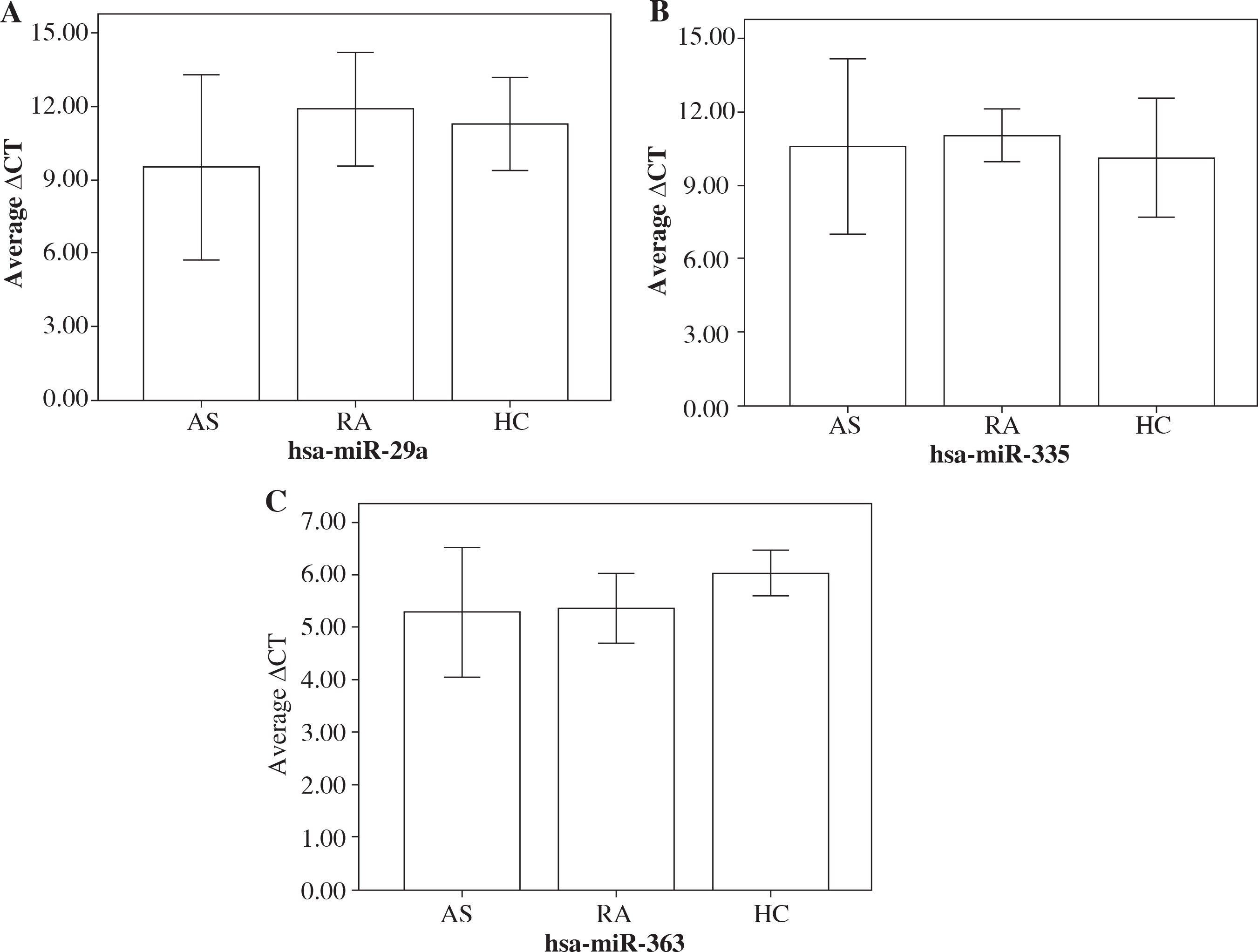
The threshold cycle (Ct) value denotes how many PCR cycles are required for the sample fluorescence to reach the threshold level. Thus, the more target microRNA present in a sample, the lower the Ct value will be, because the threshold is reached sooner. The expression of miR-29a was significantly higher in AS patients than that in RA patients and normal controls (ΔCt: 9.53 ±1.90 vs. 11.31 ±0.95 and 11.71 ±1.16, p < 0.001, Fig. 2A). The difference of miR-335 and miR-363 expression between AS patients, RA patients, and normal controls was not significant (ΔCt: 10.59 ±1.79 vs. 10.14 ±1.23 and 11.06 ±0.54, p > 0.05; ΔCt: 5.30 ±2.92 vs. 6.05 ±0.98 and 5.37 ±1.48, p > 0.05, respectively, Fig. 2B-C). The fold change of altered expression of these miRNAs in AS patients and normal controls was also shown in Table 2. The expression of DKK1 between AS patients, RA patients, and normal controls was not significant (ΔCt: 0.88 ±0.66 vs. 0.95 ±0.87 and 0.99 ±0.64, p > 0.05).
Table 2
Altered miRNAs in ankylosing spondylitis patients and normal controls
Fig. 2
Average delta Ct value of 3 microRNAs targeting Dkk-1 in ankylosing spondylitis (AS) patients and healthy controls. Results of miR-29a (A), miR-335 (B), and miR-363 (C) expression shown as Ct value (mean ±SD) in AS patients and healthy controls (HC) measured by qRT-PCR
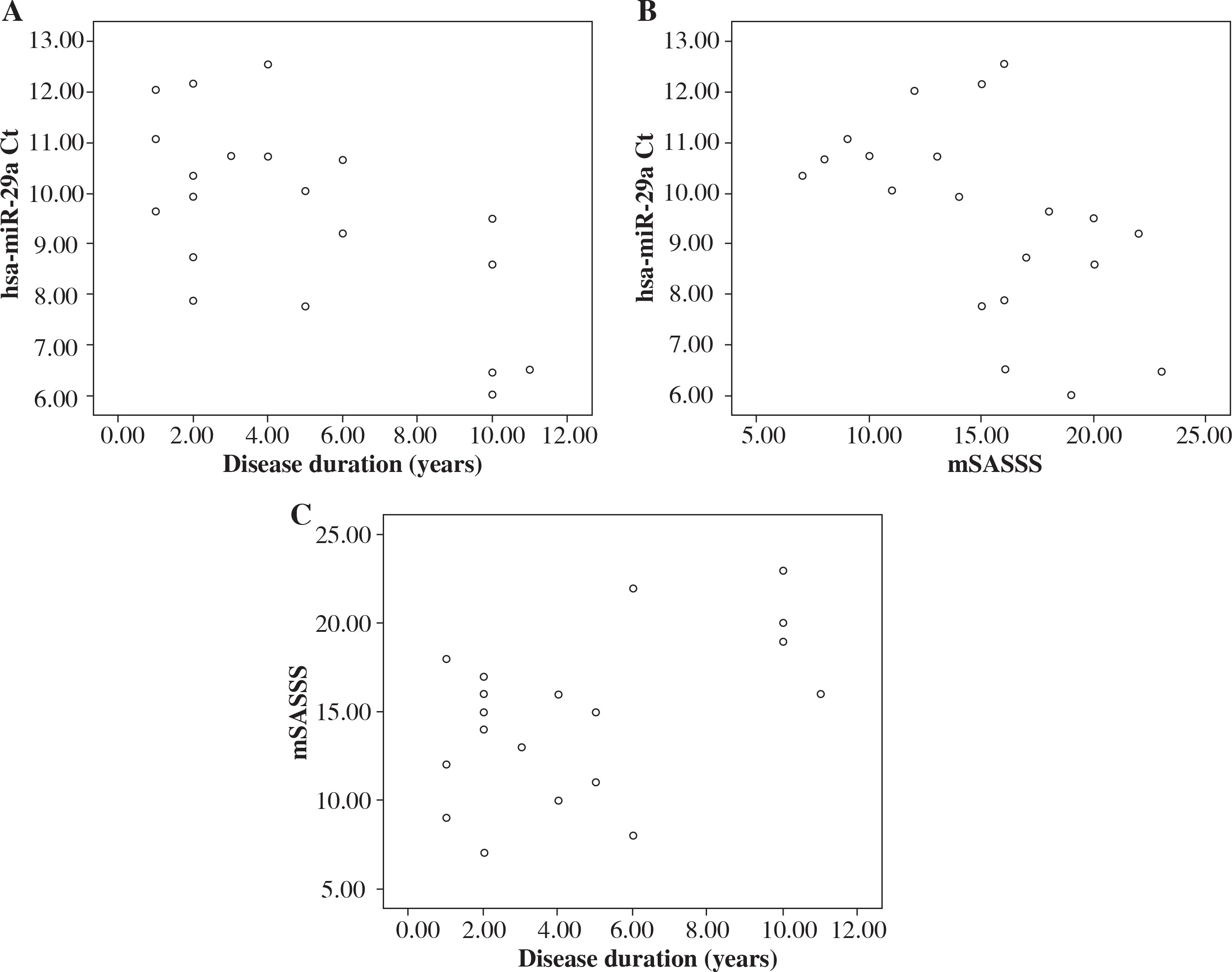
No correlation was observed between miR-29a and DKK1 (r = –0.074, p = 0.758), ESR (r = –0.331, p = 0.074), CRP (r = –0.259, p = 0.168), BASIDAI (r = –0.100, p = 0.676), and BASFI (r = –0.127, p = 0.595). The miR-29a Ct value was correlated with disease duration (r = –0.579, p = 0.008, Fig. 3A) and mSASSS (r = –0.621, p = 0.003, Fig. 3B). Meanwhile, disease duration was positively correlated with mSASSS (r = 0.473, p = 0.035, Fig. 3C).
Discussion
AS is an inflammatory disease that predominantly affects axial joints and inter-vertebral spaces. Sacroiliitis is the hallmark of AS. The disease is characterised by tight interplay between chronic inflammation and bone formation, which is only partly understood.
The mechanisms controlling new bone formation in AS are not yet fully defined, but some evidence indicates that the Wnt pathway may be the main regulator of this process. DKK-1, which can be induced by TNF and is a key inhibitor to the classic Wnt pathway, could be a link between inflammation and bone formation processes in AS [11]. The balance between proteins involved in bone formation such as Wnt proteins and that suppressing bone formation such as DKK is apparently one of the decisive steps in joint remodelling, particularly in determining whether an affected joint faces erosive damage or build up of bony spurs [12].
Dkk-1 is an inhibitory molecule that regulates the Wnt pathway, which controls osteoblastogenesis. Dkk-1 suppresses bone formation by interfering with the Wnt pathway. Dkk-1 is essential for the maintenance of skeletal homeostasis as an inhibitor of Wnt signalling and osteogenic differentiation. DKK-1 is a regulator of bone mass, with increased expression linked to osteopaenia and decreased expression to high bone mass.
Evidence that Dkk-1 is dysfunctional in AS was proven by several studies [2-6]. Dkk-1 level is lower in patients with AS than in healthy people, which might be related to the pathogenesis of new bone formation in AS. AS patients with no syndesmophyte formation show significantly higher functional Dkk1 levels, suggesting that blunted Wnt signalling suppresses new bone formation and consequently syndesmophyte growth and spinal ankylosis [13]. Similar to serum sclerostin levels, the functional Dkk1 level thus emerges as a potential biomarker for structural progression in patients with AS. Blockade of DKK1 promotes ankylosis of the sacroiliac joint [14]. DKK1 influences inflammatory of sacroiliac joints by prevention of joint ankylosis. This may indicate an important role of the Wnt signalling pathway in the structural bone changes of axial joint disease.
Increasing evidence indicates that aberrant expression of miRNAs is implicated in the pathogenesis of autoimmune diseases. We used the PubMed search tool combined with bioinformatics analysis as a strategy for screening potential miRNAs targeting DKK-1. Three miRNAs including miR-29a, miR-335, and miR-363 were selected for subsequent study.
Dkk-1 is a direct target of miR-29a. MiR-29 promotes osteoblastic differentiation, and its ability to down-regulate the expression of key Wnt signalling inhibitor Dkk-1 likely contributes to this effect by promoting Wnt signalling [15]. MiR-363 was increased more than two-fold by a change in CD4+ T cells of SF from rheumatoid arthritis (RA) patients, whereas miR-29a was significantly downregulated in a previous microarray data, with a possibly similar bone turnover mechanism involved [16]. MiR-335-5p activates Wnt signalling and promotes osteogenic differentiation by down-regulating DKK1. MiR-335 might interact with Dkk-1 in canonical Wnt signalling pathway, indicating that DKK-1 could be a potential target gene of miR-335 [17, 18].
Our results showed that only miR-29a was significantly and specifically elevated in AS patients, as compared to disease controls (RA patients) and normal controls. And the elevated miR-29a expression is positively correlated with disease duration and mSASSS. Because the mSASSS is an index reflecting structural changes weighting on new bone formation and indicating radiologic progression, the elevated miR-29a expression accompanied by advanced radiologic progression with prolonged disease duration might imply the contribution of miR-29a to new bone formation in AS.
One limitation of our study is the small sample size enrolled. The preliminary results require further investigation. The expression of miR-29a was not negatively correlated with DKK1 as expected, and miR-29a might target dozens of other genes. Meanwhile, further studies should focus on whether miR-29a can suppress the expression of Dkk-1 using western blotting as well as in vitro functional studies, in order to obtain more convincing data for the miR-29a modulation on Dkk-1.
In conclusion, miR-29a might be a specific microRNA for AS, which might contribute to the new bone formation of AS by targeting DKK-1.