
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disease, characterized by the accumulation of fat (> 5%) in the liver cells in the absence of excessive alcohol intake, chronic viral hepatitis, or other liver diseases [1]. It represents a spectrum of liver conditions ranging from isolated fatty liver to fat plus inflammation (non-alcoholic steatohepatitis), which can progress to cirrhosis [2]. NAFLD affects about a quarter of the world’s adult population and poses a significant health and economic burden to all societies [2–4]. Its prevalence parallels trends in obesity and diabetes. NAFLD is closely associated with abdominal obesity, atherogenic dyslipidaemia, hypertension, insulin resistance, and impaired glucose tolerance, all of which are features of metabolic syndrome (MetS) [5–10].
For the last years, NALFD was considered an early hepatic manifestation of metabolic syndrome, while the development of insulin resistance (IR) due to excess central adiposity has been considered as a key event in the origin and progression in the spectrum of NAFLD [11, 12]. However, 1 in 5 patients with NAFLD does not have underlying IR, and cases in this subgroup are younger, thinner (lower body mass index (BMI), waist and hip circumference), and more commonly male with fewer metabolic comorbidities [13]. But this rate of NAFLD without IR was lower than previous reports from Asia, where the prevalence was as high as 46–65.9% [14–16]. Also, epidemiologic research on the association between MetS and NAFLD has provided only limited information to guide the development of targeted interventions, particularly nutrition and pharmacological prevention programs [17].
Diagnoses of alcoholic liver disease (ALD) and NAFLD may overlap, and it is a challenge to distinguish one from the other [18]. The term NAFLD does not indicate the key role of metabolic factors as significant pathogenetic drivers in its name nor in its definition. Recently, experts reached the conclusion that NAFLD does not reflect current knowledge, and they suggest that ‘metabolic (dysfunction)-associated fatty liver disease’ (MAFLD) would be a more appropriate term. With the proposed definition, the role of metabolic dysfunction becomes central [19–21]. The experts proposed also a set of ‘positive’ criteria for the diagnosis of MAFLD – independent of alcohol intake [22].
Several studies have reported the association of NAFLD with subclinical atherosclerosis independent of traditional risk factors and metabolic syndrome [23, 24]. Overall, atherosclerosis is the main trigger of vascular disease, and endothelial dysfunction is the first stage of subclinical atherosclerosis [25, 26]. Atherosclerosis is by far the most frequent cause of coronary artery disease (CAD), with thrombosis-induced plaque disruption being the main cause of the acute coronary syndromes (ACS) [27]. The term ‘subclinical atherosclerosis’ or ‘preclinical atherosclerosis’ was introduced to describe the early stage in the atherosclerosis process, during which within the vascular walls ‘something is starting to change’ [28]. While the disease is still in a subclinical stage, there is a need for a diagnostic tool to estimate the presence and the severity of subclinical atherosclerosis in asymptomatic individuals [28]. Coronary artery calcification (CAC) is the radiological confirmation of the presence of atherosclerotic CAD [29]. The assessment of the CAC can be performed by applying the well-established Agatston score on CT, and it is expressed as a CAC score (CACs) [30].
Because atherosclerosis is a dynamic process, CACs progression provides a better reflection of atherosclerosis progression than the baseline CACs and may help predict future coronary events [31, 32]. It is reported that progression of CAC is strongly associated with the development of CV events, even after adjusting for traditional cardiovascular risk factors [31, 32]. Several studies have demonstrated the association of CAC with NAFLD [33–36].
Aim
The aim of this systematic review and meta-analysis is to assess the association of NAFLD with the progression of subclinical atherosclerotic activity, reflected as the dynamic changes in CACs over time.
Material and methods
Search strategy and inclusion criteria
Two independent authors (GK and DC) searched PubMed/MEDLINE/Embase from database inception until 31 December 2020, only in English language.
The following search terms were used “non-alcoholic fatty liver disease” or “NAFLD” or “fatty liver” AND “cardiovascular disease” or “subclinical atherosclerosis” or “preclinical atherosclerosis” or “coronary calcification” or “coronary artery calcification” or “endothelial dysfunction” or “coronary artery calcification score” or “calcium score”. The electronic search was supplemented by a manual review of reference lists from eligible publications and relevant reviews.
Inclusion criteria were as follows:
published observational studies investigating NAFLD and CAC progression in adults;
prospective or retrospective, longitudinal design;
diagnosis of NAFLD based on ultrasound, CT, or biopsy;
CACs measured by cardiac CT scan using Agatston’s method;
multivariable-adjusted estimates available;
participants without NAFLD used as a reference group.
We excluded reviews (narrative or systematic), case reports/series, editorials, opinion papers, and letters to the editor. Duplicated or overlapping reports were deleted if referring to the same title, author list, or publication date. Two authors (GK and DC) independently reviewed titles and abstracts of all citations that were identified. After all abstracts were reviewed, data comparisons between the 2 investigators were conducted to ensure completeness and reliability. The inclusion criteria were independently applied to all identified studies. Differing decisions were resolved by consensus between the 2 authors.
Data abstraction
Data on study design, risk of bias by means of Ottawa scale and patient, illness, and treatment characteristics from each study were independently extracted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) standard by 2 independent investigators (GK and DC). Whenever data were missing for the review, the authors were contacted for additional information. Inconsistencies were resolved by consensus.
Data synthesis and statistical analysis
We conducted a random effects meta-analysis of outcomes for which ≥3 studies contributed data, using Comprehensive Meta-Analysis V3 (http://www.meta-analysis.com). We explored study heterogeneity using the χ2 test of homogeneity, with p < 0.05 indicating significant heterogeneity. All analyses were two-tailed with α = 0.05. Categorical outcomes were analysed by calculating the pooled odds ratio (OR).
We conducted subgroup and exploratory maximum likelihood random effects meta-regression analyses of the co-primary and secondary outcomes. The meta-regression variable was the time of follow-up. Finally, we inspected funnel plots and used Egger’s regression test to quantify whether publication bias could have influenced the results.
Results
Search results
The initial search yielded 578 hits. A total of 34 studies were excluded, being duplicates and/or after evaluation on the title/abstract level. Of those, 486 were excluded due to not fitting the inclusion criteria. The primary reasons for exclusion were as follows: reviews (n = 95), basic research studies (n = 82), not relevant to topic (n = 277), not in English language (n = 32), and no data available (n = 5) (Figure 1).
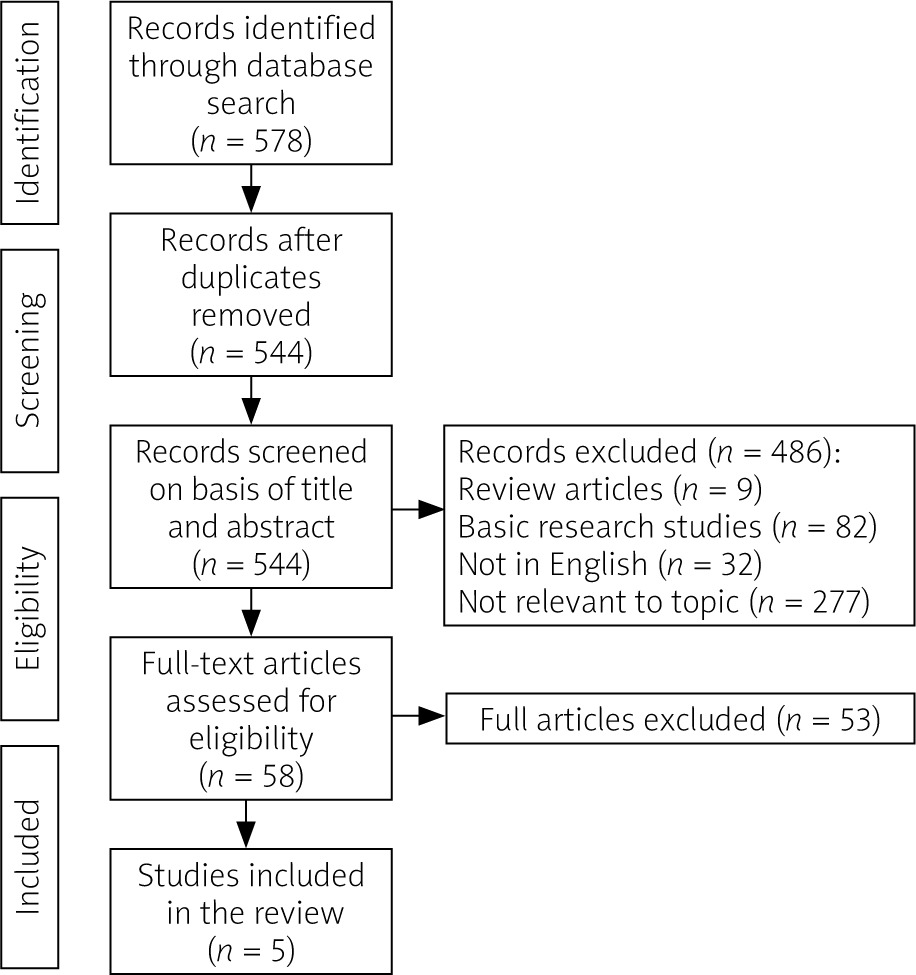
Eventually, 5 studies were included in the meta-analysis.
The studies
The main characteristics of the qualified studies in this review are summarized in Table I. The majority of the studies, 4 in total, were from South Korea [37–40], while 1 study was from the USA [41]. In the only study from the USA by VanWagner et al. [41], the cohort consisted of participants from the Coronary Artery Risk Development in Young Adults study (CARDIA study). The CARDIA study recruited, across 4 USA cities, black and white young adults in 1985 and 1986 and at 18–30 years of age. Participants underwent a 25-year follow-up from June 2010 to August 2011. Sung et al. [37] used as a study population an occupational cohort of individuals who had a comprehensive health examination from 2010 to 2012 and who were followed up in 2013. Also, Park et al. [38] used as a cohort subjects who underwent baseline and follow-up CACs assessment between November 2003 and December 2013 during general health exams. In this study the echogenic hepatic fat accumulation was graded semi-quantitatively according to the criteria of Saadeh. In a similar way, a cohort by Sinn et al. [39] consisted of healthy Korean men and women who participated in a health screening examination programme. The repeated scans were performed through December 2014. Finally, Cho et al. [40] examined asymptomatic participants who underwent repeated CACs measurements during routine health examinations. The baseline characteristics of the participant in the qualified studies are provided in Table II.
Table I
Main characteristics of the studies included in the systematic review.
| Study | Country | Study design | Aim | Study sample | Diagnosis of NAFLD | Imaging for CAC | Multivariate analyses of the NAFLD for the development/progression of coronary artery calcification | |
|---|---|---|---|---|---|---|---|---|
| OR (95% CI) | Adjustments | |||||||
| Cho et al., [40] | South Korea; single centre | Retrospective; Longitudinal study | To evaluate whether NAFLD is associated with CAC score independently of obesity | Subjects who underwent health exams | US | MDCT | Model 1: 1.33 (1.001–1.82); Model 2: 1.04 (0.75–1.44); Model 3: 1.05 (0.74–1.48); Model 4: 0.99 (0.71–1.40) | Model 1: age, race, sex, study centre, income level, educational level, alcohol intake (g/day), smoking status (current vs. never; former vs. never), physical activity score; Model 2: Model 1 + body mass index; Model 3: Model 1 + visceral adipose tissue volume; Model 4: Model 1 + diabetes status, systolic blood pressure, total cholesterol, high-density lipoprotein and treatments for hypertension and dyslipidaemia |
| Park et al., [38] | South Korea; single centre | Retrospective; Longitudinal study | To evaluate the association between NAFLD and the progression of coronary atherosclerosis | Subjects who underwent health exams | US | MDCT | Model 1–3: 1.04 (1.02–1.05); Model 4: 1.03 (1.02–1.05) | Model 1: age and sex; Model 2: Model 1 + baseline smoking status (never, former, current, and missing) and alcohol intake (none, moderate, and missing); Model 3: Model 1 + body mass index, systolic blood pressure, total and high-density lipoprotein cholesterol, triglycerides (loge-transformed), diabetes, use of antihypertensive medications, use of lipid-lowering drugs, haemoglobin A1c and estimated glomerular filtration rate; Model 4: Model 1 + time-dependent body mass index, antihypertensive medications, and lipid-lowering drugs |
| Sinn et al., [39] | South Korea; single centre | Retrospective; Longitudinal study | To evaluate whether the combination of fatty liver, IR, and obesity would be associated with an increase in CAC score over time | Subjects who underwent health exams | US | MDCT | 1.28 (0.91–1.80) | Age, sex, alcohol intake, smoking, exercise, education, DM, HTN, LDL-C, eGFR, and hsCRP at baseline, year of study, medication for HTN/DM/lipids |
| Sung et al., [37] | South Korea; single centre | Retrospective; Longitudinal study | To longitudinally associate NAFLD and CAC | Occupational cohort who underwent health exams | US | MDCT | 1.08 (0.84–1.38) | Age, sex, hypertension status, status, diabetes development, hypercholesterolaemia status, triglyceride, HDL cholesterol, glomerular filtration rate, smoking, body mass index, and waist circumference |
| VanWagner et al. [41] | USA; multicentre | CARDIA study; Prospective; longitudinal | To evaluate the association between NAFLD and the progression of the CAC | Caucasian (49.5%) and black (50.5%) adults, 18–25 years old | CT | MDCT | NAFLD(+) MetS(–): Model 1: 1.13 (0.81–1.57); Model 2: 1.17 (0.83–1.63); Model 3: 1.14 (0.81–1.60); NAFLD(+) MetS(+): Model 1: 1.45 (1.01–2.09); Model 2: 1.48 (1.02–2.15); Model 3: 1.45 (1.00–2.11) | Model 1: age, sex and BMI; Model 2: variables included in model 1 plus smoking, drinking, and exercise habits; Model 3: variables included in model 2 plus follow-up interval, LDL-C, and hsCRP |
[i] MDCT – multislice computed tomography, US – ultrasound, DM – diabetes mellitus, HTN – hypertension, SBP – systolic blood pressure, TG – triglyceride, WC – waist circumference, LDL-C – low-density lipoprotein cholesterol, hsCRP – high-sensitivity C-reactive protein, HDL – high-density lipoprotein cholesterol, BMI – body mass index, eGFR – estimated glomerular filtration rate.
Table II
Main characteristics of the participants of the studies included in the systematic review
| Studies | Cho et al. [40] | Park et al. [38] | Sinn et al. [39] | Sung et al. [37] | VanWagner et al. [41] |
|---|---|---|---|---|---|
| N | 1173 | 1732 | 4731 | 2175 | 2424 |
| Age [years] | 54.1 ±7.4 | 57.2 ±7.4 | 52.2 ±7.1 | 42.5 ±5.7 | 50.1 ±3.6 |
| Sex (% male) | 81.5 | 74.4 | 91 | 95.1 | 42.7 |
| BMI [kg/m2] mean ± SD | 25 ±3 | 24.4 ±2.6 | 24.8 ±2.6 | 25.1 ±3 | 30.6 ±7.2 |
| WC [cm] mean ± SD | 87 ±8.2 | 87.7 ±7.2 | 87.3 ±7.4 | n/a | 94.9 ±15.8 |
| Obesity (%) | n/a | n/a | n/a | 48.5 | 46 |
| Hyperlipidaemia (n%) | n/a | 29.5 | n/a | n/a | 14.7 |
| HTN (%) | 33.5 | 44.2 | n/a | 24 | 32.9 |
| DM (%) | 13.2 | 20.3 | n/a | 8.6 | 12.1 |
| Current smoker (%) | 27.4 | 16.4 | 30.9 | 33.9 | 14.1 |
| Alcohol use (%) | 53.1 | n/a | 74.7 | 34.6 | 44.1 |
| AST [U/l] mean ± SD | 25 (22–31) | 23 (20–28) | 26.8 ±16.6 | n/a | n/a |
| ALT[U/l] (median/range), mean ± SD | 23 (17–31) | 23 (18–32) | 24.9 ±10.2 | 25 (18–38) | n/a |
| γ-GT [U/l] mean ± SD | 25 (17–40) | 36.2 ±33.8 | 46.7 ±44.8 | n/a | n/a |
| FPG [mmol/l] mean ± SD | 5.8 ±1 | 99 (93–109) | 97.9 ±19.6 | 100 ±17.5 | 98.9 ±26.8 |
| HbA1c (%) mean ± SD | 5.5 (5.3–5.9) | 5.9 ±0.68 | 5.6 ±0.7 | n/a | 5.7 ±1 |
| Total cholesterol [mmol/l] mean ± SD | 93.6 ±14.4 | 199.4 ±34.6 | 198.9 ±32.7 | 210 ±37.2 | 191.9 ±36.5 |
| TG [mmol/l] mean ± SD | 23.4 (18–32.4) | 108 (76.8–152) | 130 (92–187) | 137 (94–197) | 112.3 ±88.1 |
| LDL-C [mmol/l] mean ± SD | 59.4 ±12.6 | 124.9 ±32.2 | n/a | 133 ±33.5 | 112.7 ±32.5 |
| HDL-C [mmol/l] mean ± SD | 23.4 ±5.4 | 50 (43-59) | 52.6 ±13 | 51 ±12.1 | 57.2 ±17 |
| HsCRP [mg/l] (median/range) mean ± SD | 0.6 (0.3 ±1.3) | n/a | n/a | 0.06 (0.04–0.12) | n/a |
| SBP [mm Hg] mean ± SD | 119.5 ±12.9 | 120.9 ±15.2 | 119.1 ±15.8 | 119.2 ±12.2 | 119.6 ±16.1 |
| DBP [mm Hg] mean ± SD | 76.6 ±10.6 | 78.6 ±10.9 | 75.9 ±10.7 | 76.5 ±9.5 | 74.9 ±11.2 |
| MetS (%) | n/a | n/a | n/a | 26.3 | 28 |
| Lipid-lowering medication (%) | n/a | n/a | 2.7 | 5.4 | 14.8 |
| Anti-HTM medication (%) | n/a | n/a | 19.4 | 11.2 | 27.1 |
| Anti-diabetic medication (%) | n/a | n/a | 5.4 | 3.6 | 6 |
[i] DM – diabetes mellitus, HTN – hypertension, SBP – systolic blood pressure, TG – triglyceride, WC – waist circumference, LDL-C – low-density lipoprotein cholesterol, hsCRP – high-sensitivity C-reactive protein, HDL – high-density lipoprotein cholesterol, BMI – body mass index, eGFR – estimated glomerular filtration rate, MetS – metabolic syndrome, AST – aspartate aminotransferase, ALT – alanine aminotransferase, HbA1c – haemoglobin A1c, γ-GT – γ-glutamyltransferase, FPG – fasting plasma glucose.
NAFLD and baseline CAC
VanWagner et al. [41] found at baseline a higher prevalence of CAC in NAFLD subjects compared to controls: 37.9% vs. 26%, respectively; p < 0.001. Among those with CAC, there was no significant difference in means of log-transformed CACs between NAFLD (3.59 ±1.65) and without MAFLD (3.59 ±1.7), p = 0.97. Sung et al. [37] investigated the relationship between NAFLD, insulin resistance (IR), and obesity with change in CAC over time. They divided their cohort into subjects in whom CACs increased from baseline to the follow-up period and those in whom CACs did not change. In their study, Park et al. [38] observed that the baseline CAC score was higher in NAFLD subjects than in non-NAFLD, 50.7% vs. 43.8%, p < 0.001. In the study by Sinn et al. [39], CAC at baseline was noticed in 58.1% of subjects with NAFLD and in 51.2% of subjects without NAFLD, p < 0.001. Median CACs at baseline was higher in subjects with NAFLD compared with those without NAFLD, median values: 4.0 vs. 1.0, p < 0.001. Cho et al. [40] investigated the impact of NAFLD and MetS on CAC progression. The proportion of subjects with CAC at baseline was higher in the NAFLD group (42.2%) compared to the control group (34.4%), p < 0.05. Baseline CACs in the NAFLD group was higher than in the control group (0–10 vs. 0–19, respectively; p < 0.001).
NAFLD and CAC progression
All the included studies assessed the effect of NAFLD on CAC progression. VanWagner et al. [41] showed that NAFLD participants had increased prevalence of CAC progression compared to those without NAFLD, 37.9% vs. 26.0%, respectively; p < 0.001. NAFLD remained associated with CAC after adjustment for demographics and health behaviours. Sung et al. [37] showed that in 592 (27.2%) participants, CACs increased from baseline while in the remaining 1583 subjects CACs did not change or improved during follow-up, p < 0.001. After adjusting potential confounders, the combination of IR, obesity, and fatty liver was independently associated with an increase in CAC score over time. Park et al. [38] noticed that more subjects with NAFLD than without showed CAC progression: 48.8 vs. 38.4%, respectively; p < 0.001. But the important result in his study was the fact that the impact of NAFLD on the change in CAC score significantly differed according to the CAC score at baseline. In subjects without calcification at baseline, NAFLD significantly affected the development of calcification after adjusting for traditional metabolic risk factors. However, in subjects with baseline CAC, NAFLD did not significantly affect progression. Sinn et al. [39] found that the annual rates of CAC progression in subjects with and without NAFLD were 22% and 17%, respectively; p < 0.001. In a similar way, the average annual progression of CACs in subjects with and without NAFLD was 17.8 (16–19.5) and 12.8 (11.5–14) Agatston units, respectively; p < 0.001. According with Sinn et al. [39], the association between NAFLD and CAC progression was observed both in subjects with CACs = 0 and in those with CACs > 0 at baseline. NAFLD was significantly associated with the development of CAC independently of cardiovascular and metabolic risk factors. In the study by Cho et al. [40], CAC progression was seen in 28.3% of subjects with NAFLD and in 18.6% of subjects in the control group. Also, the study showed that NAFLD is an independent risk factor for CAC progression irrespective of the presence of MetS. The data of CAC progression in NAFLD patients over time in the analysed studies are presented in Table III.
Table III
CAC progression in NAFLD patients over time
| Ref. | Baseline CAC > 0 prevalence | CAC score baseline | Follow up period | Progression of CAC over time | CAC score after follow-up | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| NAFLD cases | NAFLD n | Non-NAFLD cases | No-NAFLD n | NAFLD cases | NAFLD n | Non-NAFLD cases | No-NAFLD n | ||||
| Cho et al., 2018 [40] | 232 | 544 | 216 | 629 | Total: 0.0 (0.0–21.3); NAFLD(–) MetS(–): 0.0 (0.0–10.0); NAFLD(+) MetS(–): 0.0 (0.0–19.0); NAFLD(–) MetS(+): 1.0 (0.0–94.0); NAFLD(+) MetS(+): 1.0 (0.0–57.5) | 3.0 (2.0–3.8) years | 144 | 544 | 128 | 629 | Total: 0.6 (0.0–47.9); NAFLD(–) MetS(–): 0.0 (0.0–26.1); NAFLD(+) MetS(–): 1.5 (0.0–47.2); NAFLD(–) MetS(+): 7.0 (0.0–146.0); NAFLD(+) MetS(+): 9.0 (0.0–112.2) |
| Park et al., 2016 [38] | 429 | 846 | 368 | 866 | CAC score = 0: Total: 915 (52.8) vs. NAFLD 417 (49.3) vs. No NAFLD: 498; CAC score < 100: 507 (29.3) vs. 264 (31.2) vs. 243 (27.4); CAC score ≥ 100 < 400: 225 (13.0) vs. 123 (14.5) vs. 102 (11.5); CAC score ≥ 400: 85 (4.9) vs. 42 (5.0) vs. 43 (4.9) | Median 39 months (interquartile range, 25–55 months | 413 | 846 | 340 | 866 | CAC score 0: progressors – 713 (56.8%) vs. non-progressors – 202 (26.8%); p < 0.001; CAC score < 100: 219 (22.4%) vs. 288 (38.2%); CAC score ≥ 100, < 400: 26 (2.7%) vs. 199 (26.4%); CAC score ≥ 400: 21 (2.1%) vs. 64 (8.5%) |
| Sinn et al., 2016 [39] | 1212 | 2088 | 1353 | 2643 | CAC score > 0: Total: 2565 (54.2); No NAFLD: 1353 (51.2); NAFLD: 1212 (58.1); CAC score (Agatston units) Total: 2.0 (0–43.0); No-NAFLD: 1.0 (0–38.0); NAFLD: 4.0 (0–50.0) | Average 3.9 years | 267 | 2088 | 230 | 2643 | The annual rates of CAC progression (95% CI) in participants with and without NAFLD at baseline: 22% (20% to 23%) and 17% (16% to 18%), respectively |
| Sung et al., 2016 [37] | nd | 1142 | nd | 1033 | CAC score for Total: 19.2 ±79.6 | Median 2.3 years | 705 | 1142 | nd | 1033 | CAC score for total: 29.5 ±111.6 |
| Van Wagner et al., 2014 [41] | nd | nd | nd | nd | nd | 25 years | 88 | 232 | 570 | 2192 | CAC score > 0: NAFLD: 37.9% vs. no NAFLD: 26.0% |
Severity of NAFLD and CAC progression
Park et al. [38] found that the proportion of CAC progression was higher according to the severity of NAFLD (p < 0.001). But when subgroups were created according to the baseline CACs, the CAC progression did not significantly differ according to the severity of NAFLD (p = 0.2). Multivariate analysis showed that NAFLD severity was not associated with CAC progression. Conversely, Sinn et al. [39] showed that progression of CACs increased across categories of NAFLD severity as defined by the NAFLD fibrosis score [40].
Meta-analysis and meta-regression
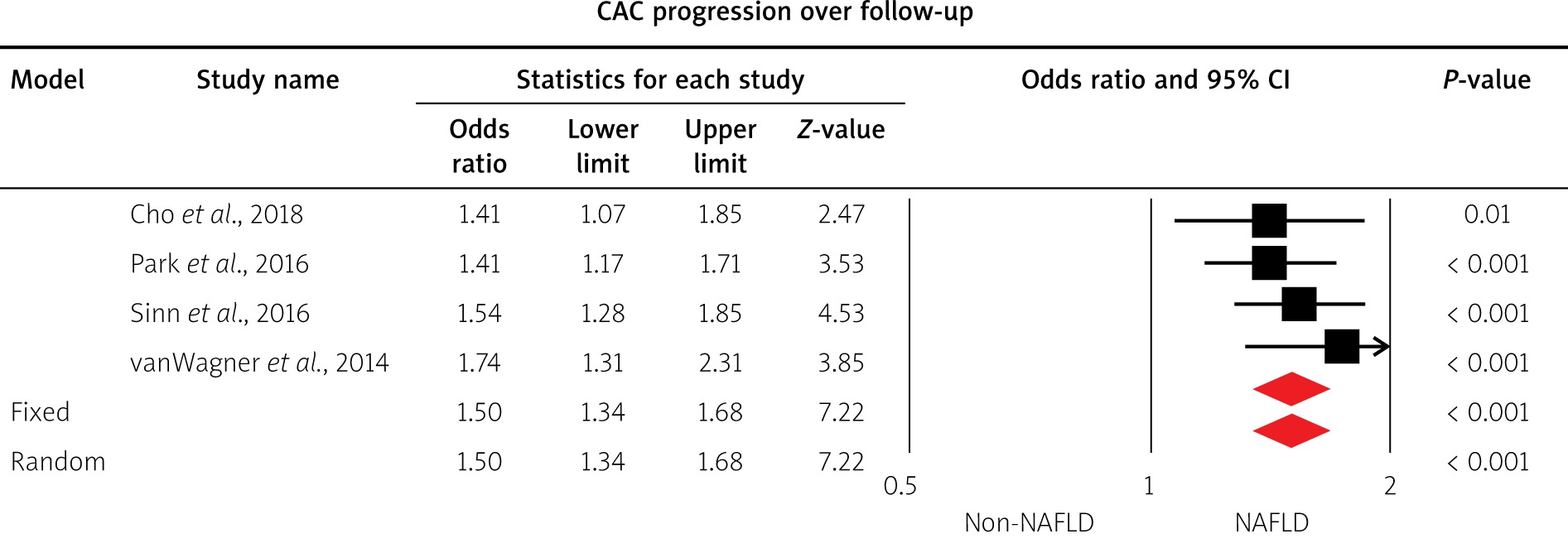
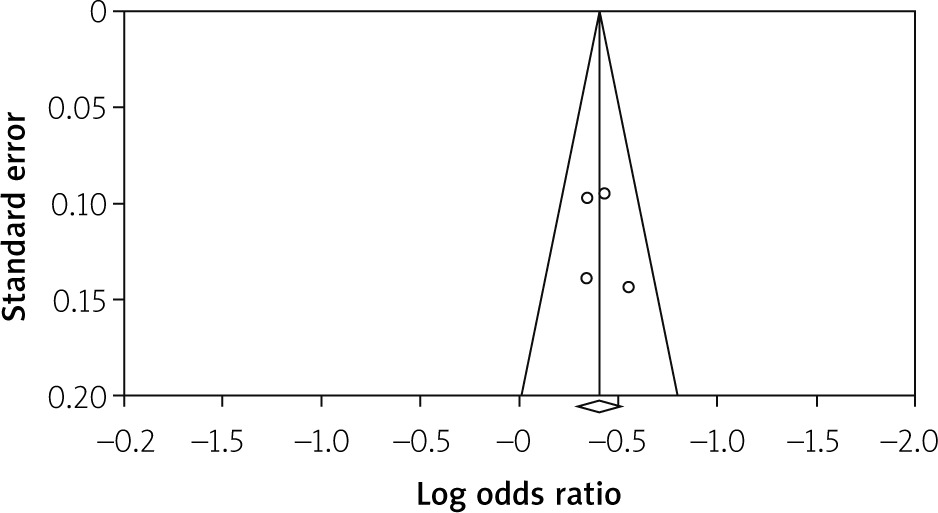
Four studies [38–41] comprising 10,060 patients provided data regarding the association of NAFLD with the progression of CAC. The analysis showed that NAFLD is associated with significant odds of CAC progression; OR = 1.5, 95% CI:1.34–1.68, p = 0.001; Figure 2. No publication bias was detected (Egger’s test p = 0.6), as depicted in Figure 3. Meta-regression analyses proved that the OR toward CAC progression was not significantly influenced by the time of follow-up (coefficient = 0.0083, Z = 1.14, p = 0.25).
Risk of bias
The quality of studies was found to be high, predominantly with a score of 7. Details are provided in Table IV.
Discussion
In our review, we found that NAFLD is associated with the progression of subclinical atherosclerosis as expressed by CAC. The statistical analysis that was performed confirmed the above findings. All the included studies concluded that this association was independent of CV risk factors. Furthermore, it was confirmed again that subjects with NAFLD have a higher prevalence of coronary atherosclerosis compared with those without NAFLD even after adjustment for demographics and health behaviours. Controversy was observed regarding the association of the progression of CAC with the severity of NAFLD. As mentioned above, only 2 studies focused on this association [38, 39]. This controversy may be related to the retrospective nature of both studies.
In this review, all the retrospective studies shared the same limitations. Firstly, the study populations consisted of subjects who repeated a second CT scan as part of their health examination. Subjects who did not receive a second scan were excluded. Furthermore, different CT scanners and radiology personnel were involved in the performing of CACs. The study personnel were unaware of the studies’ aims. As a result, measurement errors cannot be excluded. Finally, NAFLD includes a spectrum of diseases from simple steatosis to steatohepatitis and fibrosis, which cannot be diagnosed with standard US. The US scan leads to a false diagnosis in 10% to 30% of cases. In a recent study Park et al. documented that liver stiffness as assessed in NAFLD patients by magnetic resonance (MRE) was an independent predictor of the presence of CAC [42]. The authors postulated that all NAFLD patients with significant fibrosis should be referred for detailed cardiovascular risk assessment regardless of the 10-year risk of cardiovascular disease (FRS) [42].
In South Korea, employees are required to participate in annual or biennial health examinations by the Industrial Safety and Health Law [37]. Some people pay for these examinations privately, and in other instances, employers pay for these health evaluations. This fact might explain why the majority of the studies originated from South Korea.
NAFLD reflects a progressive condition in many instances, and its prevalence parallels trends in obesity and diabetes. Until now, based on numerous studies from the past 20 years, NAFLD was considered as the hepatic manifestation of MetS [11, 12]. But controversy arose because on the one hand NAFLD was defined as liver fat content > 5–10% by weight in the absence of excess alcohol consumption or any other liver disease, and on the other hand MetS is actually an aggregation of different conditions that require the presence of 3 clinical and metabolic parameters. Furthermore, only 33% of patients with NAFLD fulfil the criteria for complete diagnosis of Mets [12]. Recently, a group of experts have proposed a new name for NAFLD, which is metabolic-associated fatty liver disease [19–21]. Their definition clearly establishes this disease as a metabolic disorder. The required criteria for the establishment of diagnosis is evidence of hepatic steatosis accompanied by 1 of 3 features: a) overweight or obesity, b) T2DM, and c) lean or normal weight with evidence of metabolic dysregulation [20, 21].
Despite the extensive research conducted so far, the pathophysiology of the association between NAFLD and CAC progression remains unclear. Several mechanisms have been suggested to explain this association [10, 24, 43]. Endothelial dysfunction of systemic circulation, the first step in the process of coronary atherosclerosis, has also been observed in NAFLD [26, 44].
Recently, Mouries et al. showed that disruption of the intestinal epithelial barrier and gut vascular barrier (GVB) were early events in the development of NASH, associated with bacteria or bacterial product translocation into the blood circulation [45]. Of note, epidemiological evidence that higher levels of bacterial endotoxins constitute a strong risk factor of early atherogenesis in subjects with chronic or recurrent bacterial infections was published more than 20 years ago [46]. More recent studies have shown the association between the presence of hypercoagulability [47, 48] and small bacterial overgrowth (SIBO) [49] with NAFLD. This procoagulant imbalance or dysbiosis in NAFLD may represent a causative link between NAFLD and CV disease. Greater oxidative stress may also explain the high CV risk associated with NAFLD [48]. Finally, because the liver contains a large number of macrophages and immune cells, cytokines secreted by the injured liver have been proposed as one of the major pathogenic mechanisms generating systemic inflammation that leads to CV disease [50, 51]. The causative role of new infectious pathogens, in particular SARS-CoV-2 [52, 53] or pandemic-related stress and other lifestyle factors [54, 55], in NAFLD-related cardiovascular pathogenesis remain to be reported.
Atherosclerosis is a chronic, progressive, inflammatory disease that begins early in life and follows a long asymptomatic phase. Post-mortem evaluation of hearts of young (mean age: 22.1 years) men killed during the Vietnam conflict demonstrated that almost 50% had some evidence of coronary atherosclerosis [56]. Clinically, the CACs reflects the presence and the extent of coronary atherosclerosis and is a useful tool for individualized risk stratification. It is known that the predictive value of CACs for future cardiac events is superior to the Framingham Risk Score when used in asymptomatic subjects [57]. CACs can be used to re-classified patients at intermediate risk and to identify a considerable number of people who could benefit from statin treatment as primary prevention [58].
All asymptomatic individuals with NAFLD should be evaluated for CV disease risk, and accordingly preventive target therapies are introduced to those who would benefit most from them, including aggressive lifestyle changes and the use of antiplatelet therapy and/or cholesterol-lowering agents. This assessment can be repeated regularly. Further clinical studies are required in order to identify the optimal management pathway.











