
Introduction
During the last two decades, anti-tumour necrosis factor α agents (anti-TNF-α) have revolutionised the management of Crohn’s disease (CD). Even though newer classes of biologic therapies have become available, anti-TNF-α agents remain most effective in treatment of moderate to severe luminal and fistulising CD [1, 2]. Because of their high cost, biosimilar drugs were developed. Biosimilar are, as the name implies, similar (but not identical) to already licensed biological therapies and, after registration by European Medicines Agency (EMA), are commonly used in treatment. In Poland, according to our National Health Fund Therapeutic Program in patients with CD we can use two anti-TNF-α agents: infliximab or adalimumab (ADA). Treatment with infliximab is possible with biosimilar drugs or infliximab originator (IFX). Recently, studies have shown that biosimilar infliximab (BIFX), used in the treatment of ulcerative colitis (UC) patients, is equivalent to its biologic originator in terms of efficacy and safety [3]. It was also proven that BIFX is as safe and effective as IFX and ADA not only during induction and 1 year of therapy, but also during 12 months of follow-up in a cohort of patients with inflammatory bowel diseases (IBD). In this study relapse rates after BIFX were even lower than in patients receiving the originator drug [4]. Data directly comparing response between IFX and BIFX in anti-TNF-α naïve and non-naïve patients with CD are still needed.
Aim
The aim of our study was to assess the efficacy, tolerability, and safety of a biosimilar infliximab in comparison to the biologic originator in anti-TNF-α naïve and non-naive CD patients. The following were evaluated in both groups: achievement of clinical remission, assessment of relapse rate, side effects of biological treatment.
Material and methods
Patients
This was a retrospective, single-centre study that enrolled 168 consecutive adult CD patients between March 2013 and September 2017. All patients were enrolled into the National Health Fund Therapeutic Program, according to pre-specified criteria. We included patients older than 18 years, presenting with moderate and severe CD defined as CD Activity Index (CDAI) score above 300 points with insufficient response to standard treatment including glucocorticoids, 6-mercaptopurine (6-MP), or azathioprine (AZA), not tolerating standard treatment, or with contraindications to it. The second indication for anti-TNF-α therapy was an active perianal fistula unresponsive to antibiotics, thiopurines, and surgical treatment. Patients were given either of two medications: BIFX – Inflectra® (n = 95) or IFX – Remicade® (n = 73). The activity of the disease (CDAI and/or transrectal ultrasound – TRUS) was assessed at the qualification for treatment, after finished therapy (12 months), and after an additional year of observation (total period of follow-up 24 months). Clinical remission was defined as CDAI < 150 or a non-active fistula in TRUS after 12 months of treatment. Relapse was defined as CDAI > 150 with an increase of more than 70 points or a recurrent fistula. Patients treated before May 2014 received IFX, while those starting treatment later received either BIFX or IFX (no switching), because of the national funding of the treatment program.
Statistical analysis
For statistical analysis, descriptive statistics were used including the median, 25th and 75th percentiles, and mean values with standard deviation and range, Student’s t-test for differences between groups for quantitative variables with normal distribution, U-Mann-Whitney test for variables with non-normal distribution, and χ2 test. Statistical significance was assumed for p < 0.05.
Results
Forty-seven patients from the IFX group and 68 from the BIFX group were anti-TNF-α naïve. The non-naïve patients were previously treated with originator infliximab (n = 35) and adalimumab (n = 18). They had all stopped treatment after 1 year because of the Polish reimbursement system at that time and not due to loss of response or adverse reactions.
Both groups (IFX and BIFX) did not differ in age at the beginning of treatment, gender, disease duration, concomitant medications, and tobacco smoking distribution (p > 0.05) (Table I).
Table I
Clinical and demographic data
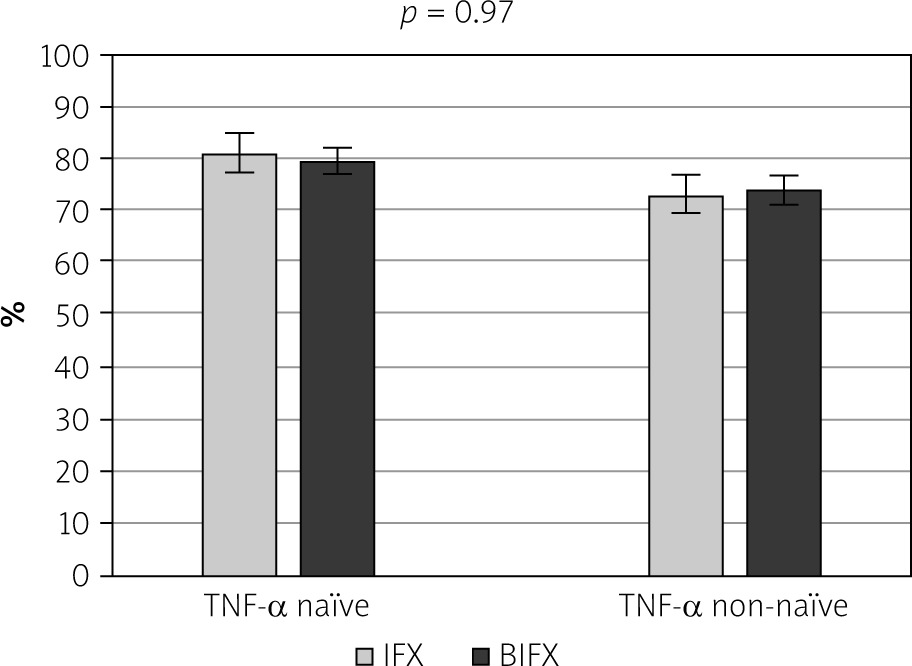
There were no differences between anti-TNF-α naïve and non-naïve patients in respect to clinical remission rate after induction and 1 year of treatment (79.3 vs. 70.3, p = 0.17 and 80.0% vs. 73.6%, p = 0.97, respectively). There were no statistical differences in achieving remission between two groups: IFX – 80.9% vs. 79.4%, p = 0.85, BIFX – 73.1% vs. 74.1%, p = 0.93 anti-TNF-α naïve and non-naïve patients, respectively (Figure 1).
Figure 1
Remission after 12 months of treatment with anti-TNF-α drugs – differences between infliximab and biosimilar patients
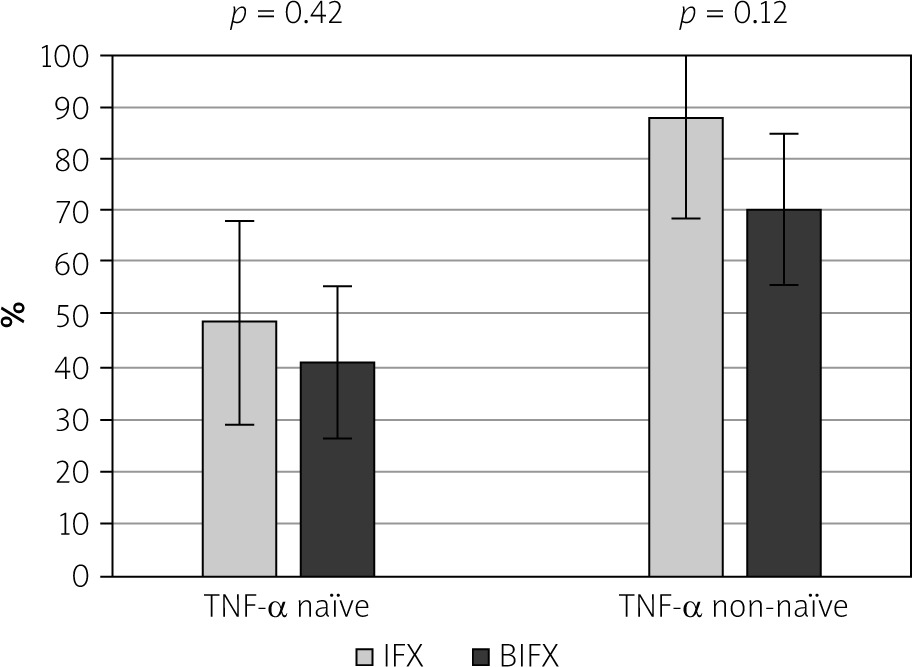
Relapse occurred in 44% of TNF-α naïve patients and 77.8% of non-naïve patients (p < 0.001) (Figure 2); however, with no significant differences between IFX and BIFX groups (anti-TNF-α naïve: IFX-48.8% vs. BIFX-40.9%, p = 0.42; anti-TNF α non-naïve: IFX-88% vs. BIFX-70.4%, p = 0.12) (Figure 3).
Figure 2
Relapse after 12-months of follow-up (24 months since beginning of treatment): differences between anti-TNF-α naïve and non-naïve patients
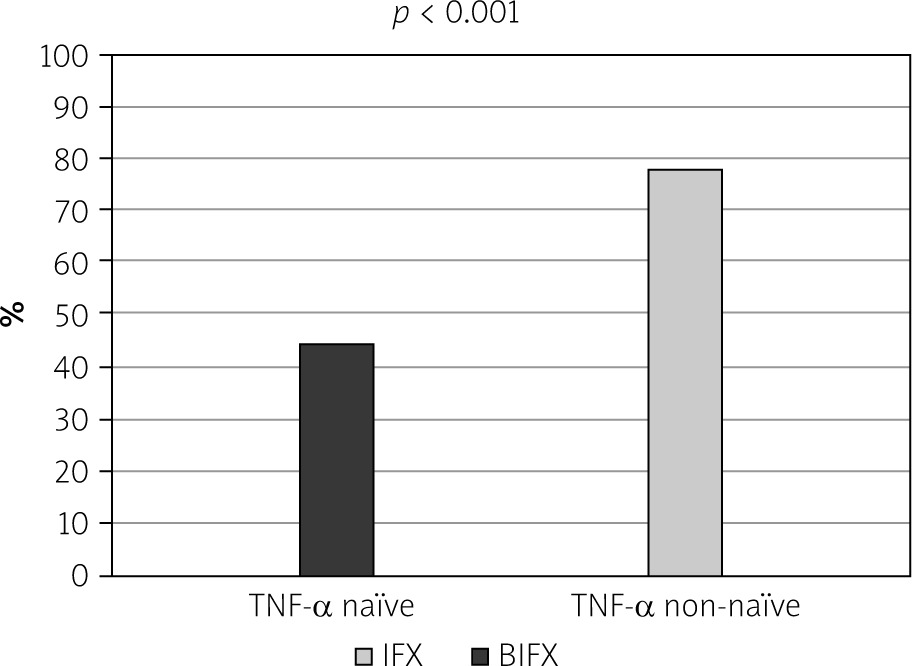
Figure 3
Relapse after 12-months of follow-up (24 months since beginning of treatment): differences between infliximab and biosimilar patients
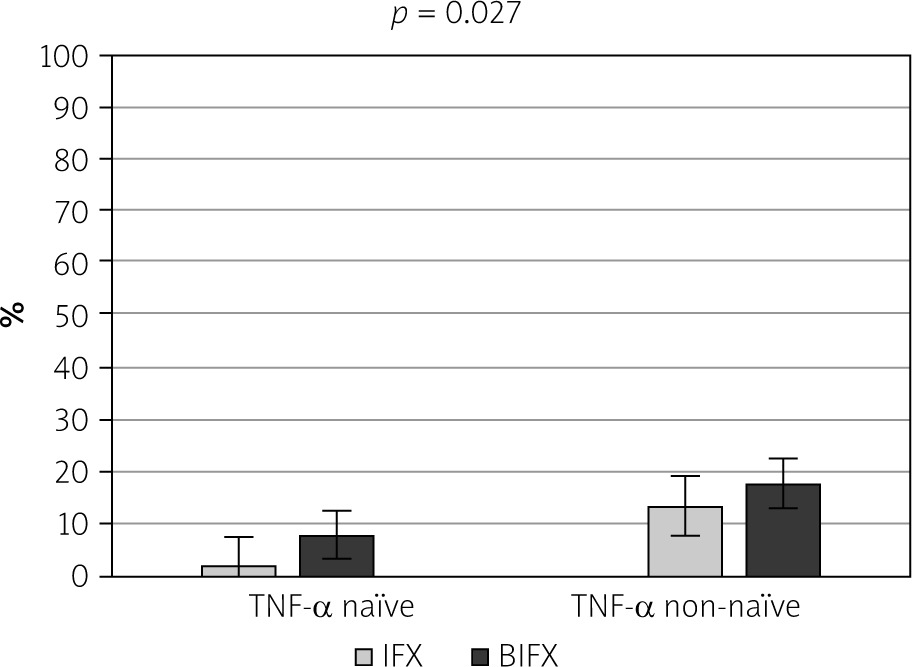
Treatment emergent adverse events (TEAEs) were mostly mild to moderate in severity and occurred more often in anti-TNF-α non-naïve patients, with no difference between the IFX and BIFX group (13.3% vs. 17.6%). Most often we observed the following: an allergic reaction, serum sickness, psoriasis, and non-viral skin reactions. Surprisingly, in anti-TNF-α naïve patients we observed a higher rate of TEAEs in the IFX group in comparison to BIFX (8.1% vs. 1.9%); however, this difference did not reach statistical significance (p = 0.14) (Figure 4).
Discussion
Anti-TNF-α agents are widely used in the treatment of patients with moderate to severe CD, especially when glucocorticoids and other immunosuppressive therapy have failed. They were introduced first in rheumatoid diseases, and for several years now they have been used by gastroenterologists in the treatment of inflammatory bowel diseases.
During the last few years many studies have compared BIFX and IFX in patients with IBD. A landmark paper was published in Lancet in 2017 reporting on the Nor-Switch Study [5]. It was a randomised, non-inferiority, double-blind, phase 4 trial. A total of 482 patients, suffering not only from CD and UC but also spondyloarthritis, rheumatoid arthritis, psoriatic arthritis, and chronic plaque psoriasis, were enrolled. Disease worsening occurred in 26% of patients in the IFX group and in 30% of patients in the BIFX group; occurrence of adverse events did not differ between all groups. The trial showed that switching from IFX was not inferior to continued treatment with it according to a pre-specified non-inferiority margin of 15%. The study did not include TNF-α-naïve patients.
In 2019 a randomised, multi-centre, double-blind, phase 3 non-inferiority crossover study was published, in which the authors included subjects with active CD who had not responded to, or were intolerant of, non-biological treatments [6]. In the intention-to-treat population the biosimilar was non-inferior to IFX in the achievement of a CDAI-70 response at week 6, 14, and 30. The proportion of patients with at least one TEAE was similar in all groups. In this study only TNF-α naïve patients were included.
Another important paper, published by Kennedy et al., analysed anti-TNF-α naïve patients only with active luminal CD, who were treated with ADA (n = 655), IFX (n = 753), and BIFX (n = 202). Patients who did not switch between drugs were included in the analysis comparing IFX to BIFX – at 14 weeks the biosimilar was non-inferior to the original drug for non-remission. The rate of adverse events and the proportion of patients with immunogenicity was similar in both groups [7].
The results of previous studies from our centre also confirm that a biosimilar product is as effective as IFX in achieving remission in both severe UC and CD [3, 4]. Clinical response in UC patients following three induction rescue doses of drug was noted in 81% of patients receiving IFX, compared to 77% receiving the biosimilar product, while clinical remission was observed in 42% receiving the originator drug and 32% receiving the biosimilar. The recurrence rate was similar in both groups. Side effects also occurred with similar frequency in the two groups [3]. In a study comparing IFX, a biosimilar product, and ADA in CD we showed that clinical response rates, clinical remission rate, and glucocorticoid-free remission rate were comparable in all observed groups. The relapse rate was similar in groups receiving infliximab biosimilar or ADA (54% vs. 61%), with relapses occurring more often in patients receiving the infliximab originator – in 83% of patients during 1 year of observation (p < 0.001) [4]. The limitation of both previous studies was that patients were not switched from infliximab originator to a biosimilar drug; they received one of them during all periods of treatment. Most of all, none of the above studies compared TNF-α naïve and non-naïve patients; therefore, we wanted to explore the possibility of differences arising in those two populations, data for which are still limited.
There are few articles comparing the use of infliximab and ADA (unfortunately not IFX and BIFX) in anti-TNF-α naïve and experienced patients. In 2016 a trial comparing results in 362 naïve patients with CD treated with ADA and infliximab was published [8]. At week 12, there was no difference between IFX and ADA patients in clinical remission (IFX 62.7% vs. ADA 63.6%, p = 0.47), clinical response (IFX 75.5% vs. ADA 76.6%, p = 0.82), and glucocorticoid-free remission (IFX 53.9% vs. ADA 57%, p = 0.60). At 12 months a similar number of patients were still in clinical remission (IFX 50.4% vs. ADA 57.3%, p = 0.48) and glucocorticoid-free remission (IFX 44.3% vs. ADA 53.7%, p = 0.16) [8].
In another paper from New Zealand researchers demonstrated that both infliximab and ADA had similar response rates in anti-TNF-α naïve and anti-TNF-α experienced groups. However, they also reported that infliximab required a concomitant immunomodulatory drug to achieve optimal maintenance of response when compared to ADA monotherapy [9].
In 2019 in JCC a propensity score-matched analysis of infliximab and ADA in TNF-naïve and experienced patients was published [10]. Among naïve patients, a clinical benefit was achieved in 81.8% of patients treated with ADA and in 77.6% of patients treated with IFX (p = 0.55) at 12 weeks; after 1 year it was still apparent in 69.2% of patients treated with ADA and 64.5% patients treated with IFX (p = 0.77). Among non-naïve patients, clinical benefit was achieved in 61.7% of patients treated with ADA and in 68.1% of patients treated with IFX (p = 0.6) at 12 weeks; after 1 year it was still present in 48.9% of patients treated with ADA and 40.4% of patients treated with IFX (p = 0.62). The studies cited above show a similar remission rate for both compared drugs, as does our study, but they compared two originator medications: infliximab and ADA.
A few studies examined the effect of biosimilar infliximab in naïve and non-naïve CD patients. The 1-year outcomes of a Hungarian nationwide cohort of CD and CU patients were also published [11], reporting the efficacy, safety, and immunogenicity of a biosimilar infliximab. Unfortunately, there was no comparator IFX in this study. Clinical efficacy was influenced by previous anti-TNF-α agent exposure in patients not taking the drug for over 1 year. Antidrug antibody positivity rates were significantly higher for subjects with previous anti-TNF-α exposure; concomitant AZA use prevented antidrug antibody formation in anti-TNF-α naive patients with CD. The remission rate in TNF-α naïve and experienced patients was similar in our study, contrary to the above cited study – this may have been caused by the fact that around 90% of the patients in our centre from both groups received thiopurines in addition to infliximab.
Another small study from Italy included 53 switched patients and only 13 naïve patients with both CD and UC treated with a biosimilar only (also no comparator), proving its safety and efficacy [12].
To treat more patients with anti-TNF-α drugs, their cheaper counterparts are needed. Therefore, studies comparing head-to-head originator and biosimilar drugs, such as those conducted by our centre, are essential. To date, only a few papers have focused on this problem. A recent Korean study compared IFX and BIFX in patients with CD and UC, both TNF-α naïve and the ones who switched therapy. The clinical response and remission at 1 year did not differ between the two drugs, and neither did the rate of adverse events. The study differed from ours in that the population was different, it was a multi-centre study (16 centres were included – due to a retrospective nature different protocols might have been used) and excluded patients that discontinued the drug early due to insufficient clinical response [13]. Therefore, one of the undisputable strengths of our study is its design comparing originator and biosimilar drugs in naïve and non-naïve subjects, and its fairly large number of patients: 168 – all treated in the same experienced centre with the same protocol. The fact that the choice between the originator drug and a biosimilar depended on the time period only is a neutral or even positive factor in our opinion because it served as an unintentional randomisation of patients. The limitations of our study are that it was retrospective in nature, we did not measure drug levels or antidrug antibody levels (although it does not change the relevance of comparison between two groups), and we did not assess mucosal healing by endoscopy (we tried to focus on clinical remission; both groups were evaluated in the same way).
The results of this study show positive treatment outcomes with both infliximab originator and biosimilar in CD patients regardless of whether they had received prior infliximab or not. BIFX was well tolerated and effective in both groups. The relapse rate during the follow-up period was significantly higher in anti-TNF-α non-naïve patients in comparison to naïve, but with no significant differences between IFX and BIFX groups.
Conclusions
Our study adds extensively to the field of drug interchangeability in the treatment of patients with IBD – an approach that helps achieve better cost-effectiveness. Further studies on immunogenicity and interchangeability with long-term follow-up periods are needed for us to be able to fully include biosimilars as an option in IBD treatment.











