
Air observed under the right dome of the diaphragm on a plain X-ray of the abdominal cavity is most often the result of perforation of the gastrointestinal tract, and thus the indication for urgent surgical intervention. However, it should be remembered that such a symptom may also have a different aetiology, not necessarily requiring surgery. More than 100 years ago, the Greek radiologist Demetrius Chilaiditi described the incidental X-ray finding of transposition of the colon between the liver and the diaphragm, which may resemble free air in the peritoneal cavity [1, 2].
A 62-year-old male patient was admitted to the Emergency Department due to severe abdominal pain which had lasted for 3 days. Moreover, he reported nausea and lack of both flatulence and stool. He was treated for hypertension. He denied other diseases and prior surgical procedures. During physical examination, the abdomen was rigid in the epigastric area and painful in palpation; the Blumberg sign was negative. Auscultation of the bowel revealed hypoactivity. In the abdominal X-ray, air was visible under the right dome of the diaphragm (Figure 1). The radiologist suggested that it could be a loop of the large intestine. Laboratory tests revealed high levels of serum amylase (3111 U/l) and leukocytosis (12.5 × 103/µl). The level of C-reactive protein was not elevated. The remaining laboratory test results were within normal limits. Due to the ambiguous clinical picture, a computed tomography (CT) of the abdomen was performed. It revealed infiltration around the tail of the pancreas and partially organised inflammatory changes between the back wall of the stomach and the body of the pancreas. A hepatic flexure of the colon was seen anteriorly to the right lobe of the liver (Figure 2). No free air was revealed in the peritoneal cavity. The patient was admitted to the surgical ward due to acute pancreatitis. An ultrasound examination of the abdomen excluded gallstones as the aetiology of the pancreatitis. Conservative treatment was administered, resulting in improvement of the general condition and relief of symptoms. The patient was discharged after 6 days of hospitalisation.
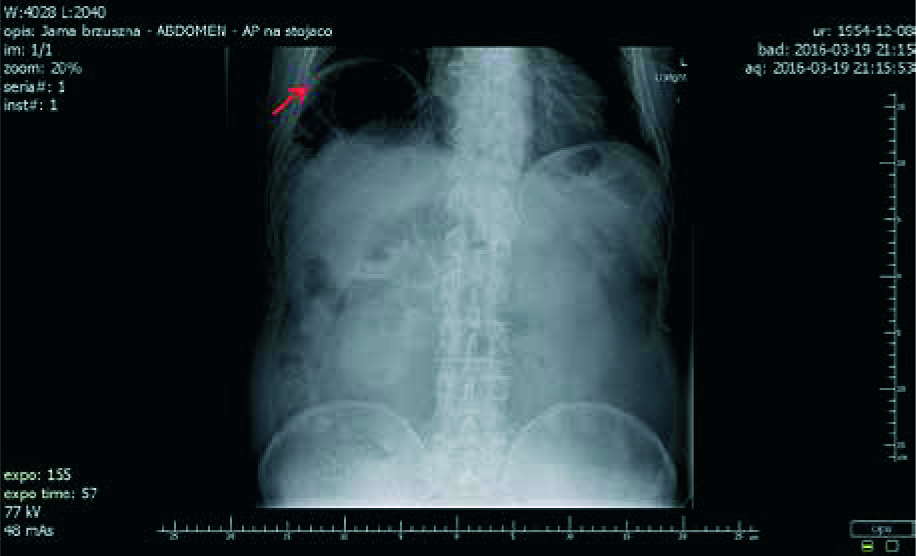
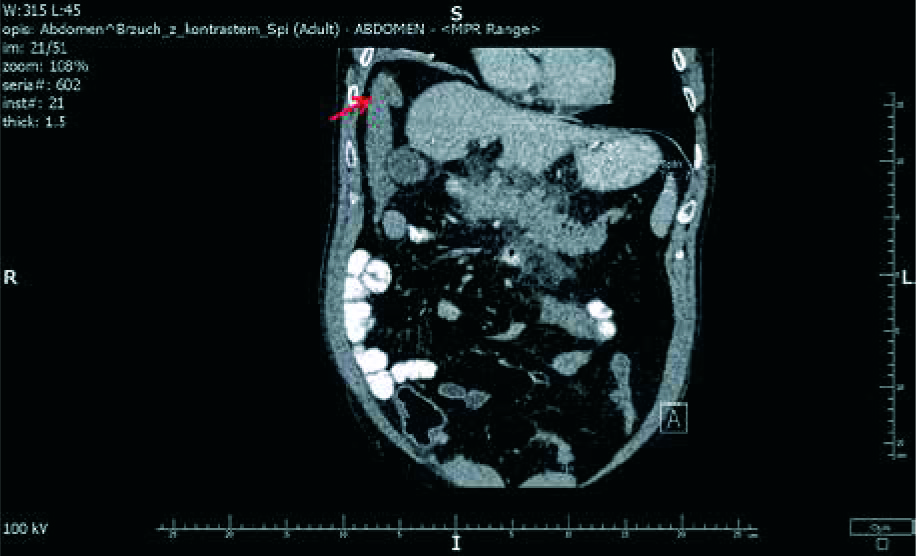
Figure 2
A hepatic flexure of the colon (red arrow) visible anteriorly to the right lobe of the liver on abdominal CT (frontal plane)
Chilaiditi sign in a plain X-ray of the abdomen is defined as the presence of air under the right hemidiaphragm. It is a result of a transposition of the colonic hepatic flexure between the liver surface and the dome of the diaphragm. In a few cases, approximately 3–5%, the small intestine is dislocated. This abnormality is usually asymptomatic, but if clinical symptoms like abdominal pain, bloating, vomiting, or constipation are present, it is termed Chilaiditi syndrome. The frequency of this sign in abdominal or chest X-rays is estimated at 0.025–0.28% [3] and increases with age, with a male predominance observed [4, 5].
Under normal conditions, the fixation of the colon prevents its translocation. However, some anatomical variations may facilitate its pathologic interposition. These include absence, laxity, or elongation of the suspensory ligaments of the transverse colon or the falciform ligament, dolichocolon (an excessively long colon), as well as congenital malposition of the intestines. This anatomic distortion can also result from functional disorders, such as constipation, which lead to elongation of the large intestine; aerophagia, which causes its distension; or liver atrophy as a result of cirrhosis or hepatectomy. Diaphragmatic paralysis, chronic chest disease, obesity, multiple pregnancies, and ascites are also associated with Chilaiditi syndrome [5, 6].
As mentioned previously, colonic interposition rarely produces clinical symptoms, and when they are present, they usually do not require surgical treatment. Intravenous fluid therapy, bowel decompression, and enemas are recommended. If the patient responds to initial conservative management, disappearance of Chilaiditi sign and the reposition of the colon to the normal anatomical position are often observed in a subsequent abdominal X-ray. In very rare cases, if the discomfort persists, this condition may lead to bowel obstruction or ischaemia, requiring surgery [7].
It is worth mentioning that in the case of very severe clinical signs, it is necessary to first consider more serious causes of the air under the right diaphragm, such as perforation or subphrenic abscesses. On the other hand, as in the case of our patient, severe pain may not be due to gastrointestinal perforation, and misinterpreted Chilaiditi sign may encourage an inexperienced surgeon to perform unnecessary laparotomy.
A characteristic feature of air accumulated in the large intestine is the presence of haustral folds. If the small intestine is dislocated, the circular folds (folds of Kerckring) are visible. When in doubt, a second X-ray image should be taken after repositioning the patient (for example, with the patient lying on their left side), which will change the location of the air if it has accumulated in the peritoneal cavity. In unclear cases, computed tomography should establish a definitive diagnosis [8].
It is very important to identify Chilaiditi sign before some invasive diagnostic procedures within the abdominal cavity. An excellent example is liver biopsy in patients with cirrhosis, who are predisposed to intestine transposition. Similarly, colonoscopy should be performed with great caution. Firstly, it may be difficult to insert an endoscope into the interposed colon. Secondly, the intestine can then be easily angulated and distended, which may lead to perforation [7, 9].
Every surgeon should be aware of Chilaiditi sign. This is particularly important when the clinical picture (including plain abdominal X-ray) of the patient is not compatible with the suspicion of perforation. In doubtful cases, it is necessary to extend the diagnosis. Failure to recognise transposition of the intestine between the liver and the diaphragm can expose the patient to unnecessary laparotomy and all the consequences associated with it.











