
Introduction
Crohn’s disease (CD) is a chronic transmural gastrointestinal inflammatory disorder. Although inflammatory bowel diseases (IBD) are usually diagnosed in young adults aged 18 to 35 years, the rate of paediatric diagnosis has been steadily increasing in recent years [1]. Ileocolonoscopy remains a gold standard in assessing mucosal healing (MH); however, the use of ileocolonoscopy in paediatric patients is fraught with several limitations such as invasiveness, costs, need for hospitalization, and risks connected with general sedation. Studies have demonstrated a lack of correlation between clinical symptoms and disease activity [2]; therefore, achieving MH and transmural healing (TH) is nowadays the most eligible therapeutic goal. The Mucosal Inflammation Noninvasive Index (MINI) is a new clinimetric tool for assessing mucosal healing and inflammation in paediatric patients, which has recently been developed by Cozijnsen et al. [3]. The MINI index evaluates the following categories: stool pattern, faecal calprotectin (FC), erythrocyte sedimentation rate (ESR), and C-reactive protein. This score could help to improve the selection of patients with CD, who require a follow-up ileocolonoscopy.
Aim
The aim of this study was to assess the clinical importance of the MINI index in newly diagnosed paediatric CD patients.
Material and methods
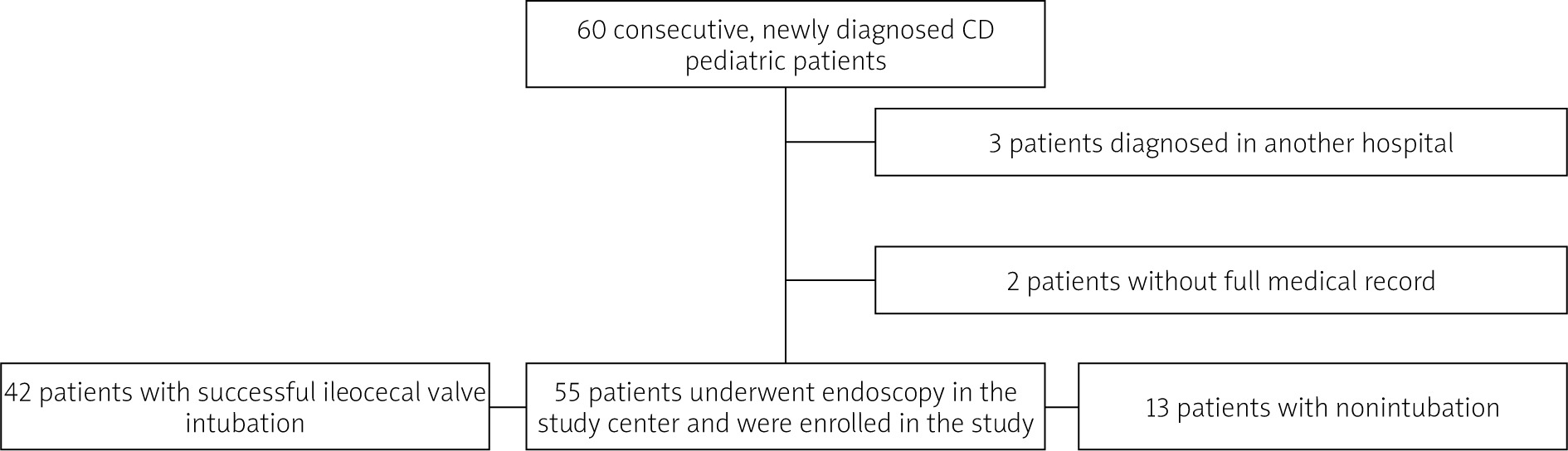
This observational, single-centre research involved 60 consecutive newly diagnosed (between March 2015 and September 2016) paediatric CD patients. Fifty-five patients who met all inclusion and exclusion criteria were enrolled in the study. The diagnosis was based on endoscopy examination, clinical presentation, and histopathology, according to the accepted diagnostic criteria for CD [4]. Children who were diagnosed in another hospital or those with incomplete medical records were excluded. In 13 out of 55 patients who underwent ileocolonoscopy, ileal intubation was not achieved (Figure 1). The groups with successful intubation and non-intubation were analysed separately. Demographic and clinical data were collected prospectively. The MINI index was calculated retrospectively.
Location and clinical manifestation were evaluated according to the Paris classification [5]. Laboratory data were collected prospectively up to 7 days before endoscopic evaluation. Endoscopic disease activity was captured using the Simple Endoscopic Score for Crohn’s Disease (SES-CD) [6]. Mucosal healing was defined as SESCD < 3 points, mild disease as 3–6 points, moderate 7–16 points, and severe >16 points. Clinical disease activity was evaluated using the Paediatric Crohn’s Disease Activity Index (PCDAI): remission < 10 points, mild 10–27.5 points, moderate 30–37.5 points, and severe 37.5–100 points [7]. Although the weighted Paediatric Crohn’s Disease Activity Index (wPCDAI) has been shown to better evaluate disease activity than PCDAI [8], due to the observational characteristics of the study, we chose not to calculate wPCDAI retrospectively. The MINI index is a weighted categorized index that discriminates MH from mucosal inflammation in children with CD. The key items of the MINI index are stool pattern during the preceding week, faecal calprotectin concentration, erythrocyte sedimentation rate, and C-reactive protein concentration. The maximum score for the MINI index is 25 points, and the minimum score is –3 points (Table I).
Table I
The MINI index [3]
[i] CRP – C-reactive protein, ESR – erythrocyte sedimentation rate. *The stool item interpretation was performed as indicated in the user guide of the MINI index: 0 points – formed stool or up to 1 loose stool daily, 4 points – 2–5 liquid/very loose stools on ≥ 1 days or small amounts of blood, 8 points – ≥ 6 liquid/very loose stools on ≥ 1 days or nocturnal diarrhoea and/or any gross bleeding.
The study was approved by the Bioethics Committee of the Jagiellonian University, Krakow (No. 122.6120.52.2015).
Statistical analysis
Categorical data were reported as the number of patients and the percentage of the respective group. Quantitative data were summarized as mean ± standard deviation (SD) or median and lower; upper quartile (Q1; Q3), depending on the distribution. The variables' distribution was assessed for normality using the Kolmogorov-Smirnov test. Minimum (min.) and maximum (max.) values were reported where indicated. The data were compared between groups using the Pearson χ2 test (categorical variables), t-test (normally distributed quantitative variables), or the Mann-Whitney test (non-normally distributed quantitative variables). The Kruskal-Wallis test was used to compare MINI scores when more than 2 groups were compared. The Spearman correlation coefficient was used to assess the correlations of the MINI score, which was non-normally distributed. The receiver operating characteristic (ROC) curve analysis was used to assess the diagnostic accuracy of MINI score to detect severe Crohn’s disease defined as SES-CD ≥ 16 points. The cut-off was selected at maximum Youden index. All the statistical tests were 2-tailed. The results were considered statistically significant at p-value < 0.05. The computations were done using Statistica 13.0 software (TIBCO, Tulsa, OK, USA).
Results
A total of 55 paediatric patients participated in the study. In 42 patients ileocolonoscopy was successful (52.4% males and 47.6% females at the average age of 12.0 ±3.8 years). There were 13 (23%) patients in whom ileal intubation was not achieved (53.8% males and 46.2% females with mean age of 12.6 ±3.3 years at diagnosis). Baseline characteristics of both groups are presented in Table II.
Table II
Patients’ characteristics and Paris classification
In the studied group of 42 patients with complete ileocolonoscopy, there were no statistically significant associations between MINI and disease phenotype (localization, growth retardation, disease behaviour). Mean SES-CD was 15.5 ±6.8 points, and mean PCDAI was 28.6 ±15.4 points. A positive correlation between PCDAI and SES-CD scores (R = 0.35; p = 0.025) was observed. There was no significant relationship between disease phenotype and FC concentrations. The correlations between FC and SES-CD and between FC and PCDAI were R = 0.37; p = 0.016 and R = 0.52; p = 0.0004, respectively. The median MINI score was 19 (Q1: 15; Q3: 22). Further analysis showed a strong positive correlation between MINI and PCDAI (R = 0.61; p < 0.001) and a moderate positive correlation between MINI and SES-CD (R = 0.39; p = 0.011) (Figure 2). The MINI score according to SES-CD categories is presented in Figure 3. In our study, a MINI score of 17 points or more indicated severe CD (defined as SES-CD ≥ 16 points) with a diagnostic sensitivity of 90% but with a low specificity of 50%. Additionally, the MINI score correlated positively with white blood cell count (WBC) (R = 0.47; p = 0.002) and platelet count (PLT) (R = 0.41; p = 0.007) but negatively with albumin concentration (R = –0.35; p = 0.022).
Figure 2
The correlations between MINI and PCDAI (A), SES-CD (B) in the studied group of 42 patients with full endoscopy. Spearman’s rank correlation coefficients (R) and p-values are reported
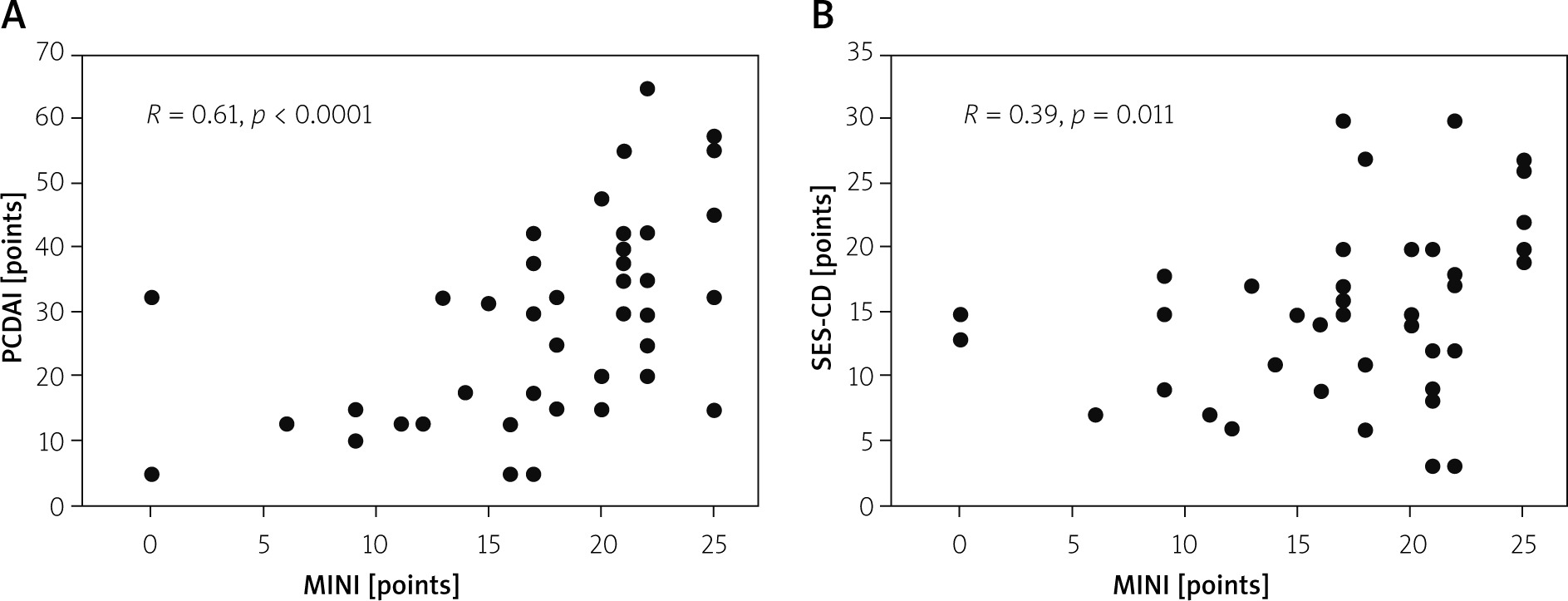
Figure 3
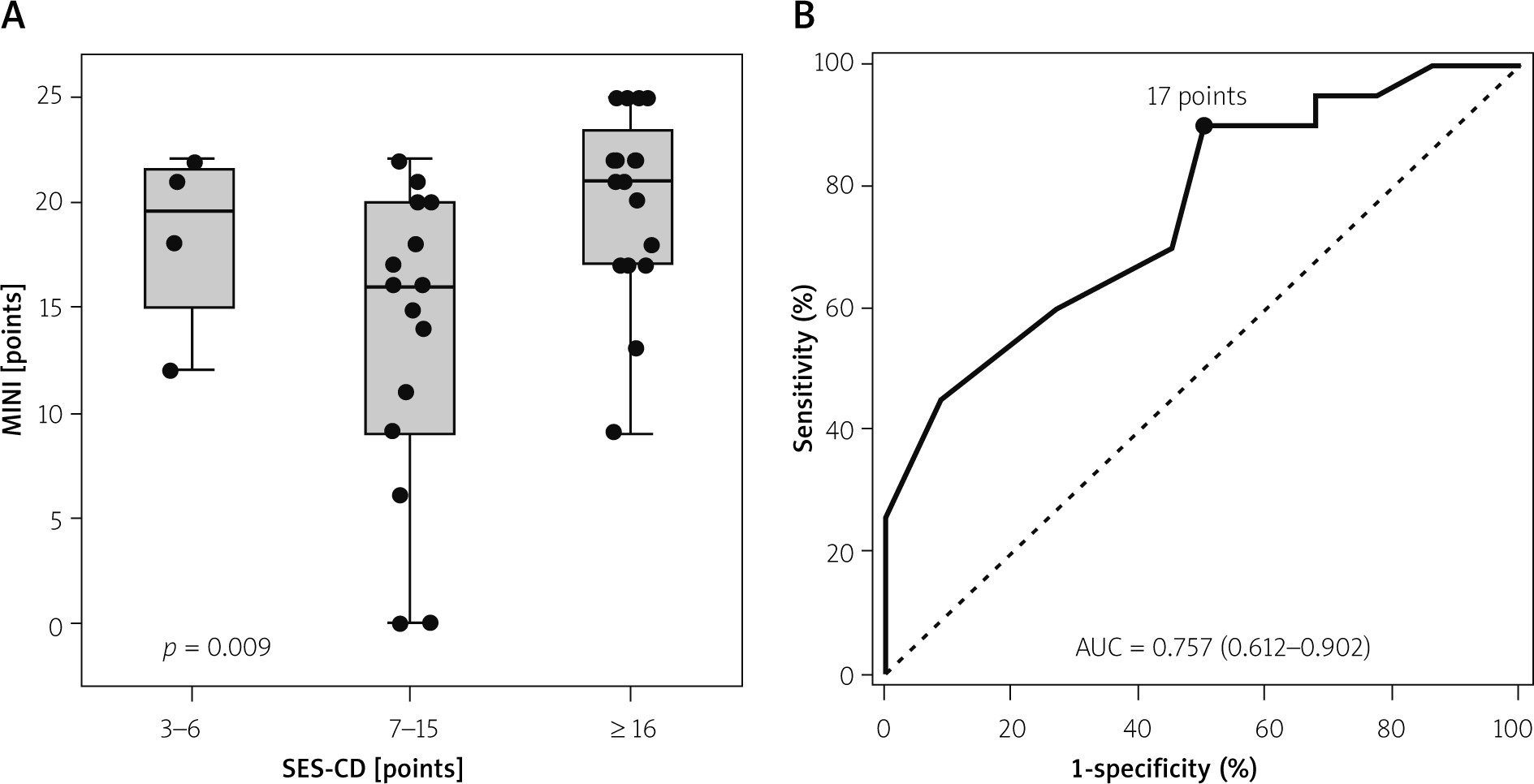
The MINI score according to SES-CD categories (A) and the ROC curve illustrating the accuracy of the MINI score in detecting severe disease according to SES-CD (i.e. SES-CD ≥ 16 points) (B) in the studied group of 42 patients with full endoscopy. The p-value in the Kruskal-Wallis test is reported in panel A. The cut-off point selected using maximum Youden index and the area under the ROC curve (AUC) with 95% confidence interval are reported in panel B
Non-intubation occurred in 13 (23%) patients. Out of these 13 children, in 7 patients the ileocecal valve was reached but not intubated. In 3 patients the cecum was reached, in 1 patient hepatic flexure was examined, and in 2 transverse colon was evaluated. The difficulties in performing full endoscopy were related to advanced disease changes. There were no statistically significant differences between groups with successful ileal intubation and with non-intubation apart from disease behaviour (stricturing or non-stricturing) (Table II). The correlation between MINI and PCDAI in the non-intubation group was strong (R = 0.66; p = 0.014).
Discussion
Mucosal healing has become a therapeutic goal in CD, but its frequent evaluation in endoscopic examination is fraught with several limitations. There is an increasing demand to replace invasive procedures with noninvasive markers of CD. The commonly used clinical disease activity index (PCDAI) correlates poorly to moderately with activity assessment during endoscopic examination (R = 0.33–0.59) [3, 9]. Correlations between concentration of FC and SES-CD are usually higher; therefore, this biochemical marker is used increasingly to monitor patients with CD. However, treatment modification based only on FC results is currently not recommended [10]. The newly reported Mucosal Inflammation Noninvasive Index (MINI), which was developed to assess mucosal inflammation in children with CD, is a promising tool. Recent studies have shown that the MINI index can be more accurate than calprotectin alone in detecting endoscopic healing [3]. In our study we aimed to assess if the MINI index correlates with endoscopic changes at the onset of paediatric Crohn’s disease. Our study group consisted of newly diagnosed patients who mostly had moderate to severe activity of CD. Mean SES-CD and PCDAI, and median MINI index were higher than those reported by Cozijnsen et al. [3] and by Perez et al. [11], which is related to a different patient selection process and may also be associated with a less numerous group of participants in our study. Similarly to the previously mentioned studies, in our research we observed a positive correlation between MINI and SES-CD, which was comparable to the correlation between PCDAI and SES-CD and between FC and SES-CD. There was also a high correlation between MINI and PCDAI. Martinus A. Conzijnsen et al. reported that MINI < 8 points could assess MH with a sensitivity of 88% and specificity of 85%. According to this study [3], a MINI score < 8 points indicates MH, MINI 8–11 points reflects mild inflammation, and MINI > 11 points detects moderate to severe disease. In our study, a MINI score of 17 points or more corresponded to severe Crohn’s disease (defined as SES-CD ≥ 16 points) with a diagnostic sensitivity of 90% and a low specificity of 50%. There were only 4 patients with SES-CD < 7 points, and there were no patients with SES-CD < 3 points, which is related to the study design (the inclusion of newly diagnosed patients). In fact, the 4 patients with SES-CD 3-6 points were characterized by relatively high MINI (Figure 3).
Ileal non-intubation occurs in 20–25% of colonoscopies in paediatric CD patients [12]. When diagnosed with CD, most children represent an inflammatory phenotype of the disease (non-stricturing and non-penetrating), but there is a subgroup with complicated disease behaviour [13]. In the EUROKIDS study, the stricturing phenotype (B2) was observed in 12.2% of the cases, the penetrating phenotype in 4.7%, and both stricturing and penetrating disease (B2B3) in 1.6% [14]. Therefore, in contrast to Cozijnsen et al. and Perez et al., we decided not to exclude those patients but to analyse them separately. In our study there were 13 (23%) patients in whom ileocecal valve intubation was not achieved. Fourteen (25%) patients had stricturing phenotype of the disease. Out of those 14 patients, 5 had successful ileocolonoscopy. We found a high positive correlation between MINI and PCDAI in patients with unsuccessful ileocolonoscopy. Further investigation is necessary to assess the clinical importance of the MINI index in those patients. Our study was limited by relatively small numbers of patients and retrospective calculation of the MINI index, although individual MINI components (stool pattern, FC, ESR, and C-reactive protein) were collected prospectively.
Conclusions
The MINI index has several advantages. It positively correlates with SES-CD and PCDAI. Due to its non-invasiveness and simplicity, the MINI index can be considered an intuitive and useful tool in assessing mucosal inflammation in newly diagnosed paediatric CD patients, possibly also in those with unsuccessful colonoscopy.











