
Introduction
Dyspepsia denotes a constellation of chronic or recurrent symptoms related to the upper GI tract, manifested as epigastric discomfort or pain, postprandial fullness, early satiety, bloating, nausea, eructation or heartburn [1]. According to Rome IV criteria, functional dyspepsia (FD) is defined as one or more of the following symptoms: epigastric pain, epigastric burning, early satiety, and postprandial fullness, present for the last 3 months with symptom onset at least 6 months prior to diagnosis, in the absence of structural disease [2]. It is categorized into two syndromes, postprandial distress syndrome (PDS) (predominant postprandial fullness and early satiety), and epigastric pain syndrome (EPS) (predominant epigastric pain or epigastric burning). More practical criteria from the National Institute for Health and Care Excellence (NICE), American College of Gastroenterologists and Canadian Association of Gastroenterologists added nausea, vomiting, and heart burn to the range of dyspepsia symptoms in Rome IV, with symptoms duration of 1 month rather than 3 months [3]. The community prevalence of dyspepsia is in the range of 20–40% [4]. It has been estimated that FD cost for the health budget system of the United States was US$ 18.4 billion in the financial year 2009 due to costs of investigations, medications, and work loss [5]. The correlation between symptoms of dyspepsia and the underlying lesion is usually poor, thus, endoscopic findings might be normal or reveal only minor lesions in significant proportions of patients. What further complicates the issue is that symptoms of dyspepsia may overlap or coexist with symptoms of other GI disorders like gastroparesis, irritable bowel syndrome or gastroesophageal reflux disease (GERD) [4]. It is well established that H. pylori infection is associated with gastritis, peptic ulcers, and neoplastic growth of the stomach; all of which may present with dyspepsia. On the other hand, H. pylori is frequently encountered in dyspeptic patients with normal endoscopic findings, particularly in areas with a high prevalence of such infection [6]. The trend of sending too many patients with dyspepsia for endoscopy is not cost-effective and may cause some complications. On the other hand, performing endoscopy may satisfy the patient and the clinician when the final diagnosis is established. International criteria have been developed regarding indications of endoscopy in the case of dyspepsia, which relied on clinical history, patient age, and presence of alarm features (age > 50 years, anaemia, GI bleeding, weight loss, persistent vomiting, dysphagia, odynophagia, family history of malignancy, palpable mass, and lymphadenopathy) [1]. However, despite development of such guidelines, clinicians frequently manage patients on an individual basis. Treatment of dyspepsia is not always successful, particularly when no defined cause is found [7]. Dyspepsia due to organic causes responds more favourably to therapy compared to FD, particularly if the latter is associated with underlying psychiatric condition. In Mosul (a big town located in the north part of Iraq), primary care physicians are confronted with increasing numbers of patients suffering from dyspepsia and a proportion of such patients are sent to endoscopy based on low evidence-based indications. However, majority of dyspeptic patients are not seen by clinicians and take non-prescribed antacids, acid inhibiting drugs, antispasmodics, or even herbal remedies.
Aim
The aim of this study is to evaluate the role of endoscopy in dyspepsia, assess presenting complaints, demonstrate significance of patient age, alarm features, and drug use and relate it to final endoscopic diagnosis.
Material and methods
This is a single-centre, cross-sectional study involving 372 patients presented with dyspepsia in the endoscopy unit of Al-Salam General Hospital in Mosul, during a period of 2 years from Jan 2018 to Jan 2020. The source of patients is primary health care centres, hospital consultation clinics, inpatient hospital wards, and private clinics. Referred patients depended on clinician discretion and evaluation of dyspepsia. All patients (aged 18 years and above) having dyspepsia of more than 1 month duration were consecutively recruited and underwent upper GI endoscopy examination. Demographic information of patients was registered. Clinical face-to-face interview of patients included history taking and drug intake. A set of questions were answered by all patients which concerned complaints of dyspepsia symptoms (epigastric pain, epigastric burning, postprandial fullness, early satiety, bloating, belching, nausea, vomiting, food regurgitations, and heart burn). Alarm features were recorded (anaemia, weight loss, persistent vomiting). Exclusion criteria were dysphagia, odynophagia, overt upper GI bleeding, jaundice, surgical GI operations, past history of peptic ulcers, and major organ failure. Detailed endoscopic findings were documented. Biopsies of suspicious lesions were performed and subjected to histopathological examination. Five biopsies were taken from antrum, lesser and greater curves of the stomach to detect H. pylori infection. Endoscopic findings of duodenitis and or gastritis relied on presence of mucosal erythema, oedema, with or without erosions, were referred to as erosive and non-erosive GD. Esophagitis was categorized according to Los Angeles (LA) grading system (A, B, C, D) [8]. Endoscopic results of esophagitis LA grade A, non-erosive GD, and normal findings were regarded as non-significant findings, whereas esophagitis grade B, C, D, erosive GD, peptic ulcers, and neoplasms were regarded as significant findings [9].
Statistical analysis
Statistical analysis was performed by using the statistical package for social sciences (SPSS version 20, USA). Descriptive statistics were used to calculate the mean, median, range, percentage, standard deviation (SD), and p-value. The level of significance for p-value (two-tailed test) was set at 0.05. Tables and pie chart were applied to clarify the demonstration. This study was approved by the Ninevah Health Directorate and Medical Ethical Committee of Ninevah University (license number 78, of 24 August 2020). All patients agreed to sign a written document prior to endoscopic examination.
Results
The sample included 372 patients (198 females, 174 males). Female/male ratio was 1.1 : 1 (p = 0.007). Mean age was 35.7 ±13.5 years (age range: 18–80 years). Age group of 50 years and above comprised 18.8% (70/372, p = 0.001). Patients presented mainly with EPS comprised 61.6% (229/372), while PDS 19.1% (71/372, p = 0.001) (Table I).
Table I
Main symptoms of patients with dyspepsia (n = 372)
Non-significant endoscopic findings (non-erosive GD, esophagitis LA grade A, and normal results) comprised 70.2% (261/372, p = 0.001), whereas significant endoscopic findings (erosive GD, peptic ulcers, esophagitis LA grade B, C, D, and neoplasms) 29.8% (111/362) (Table II).
Table II
Endoscopic findings in patients with dyspepsia related to age groups
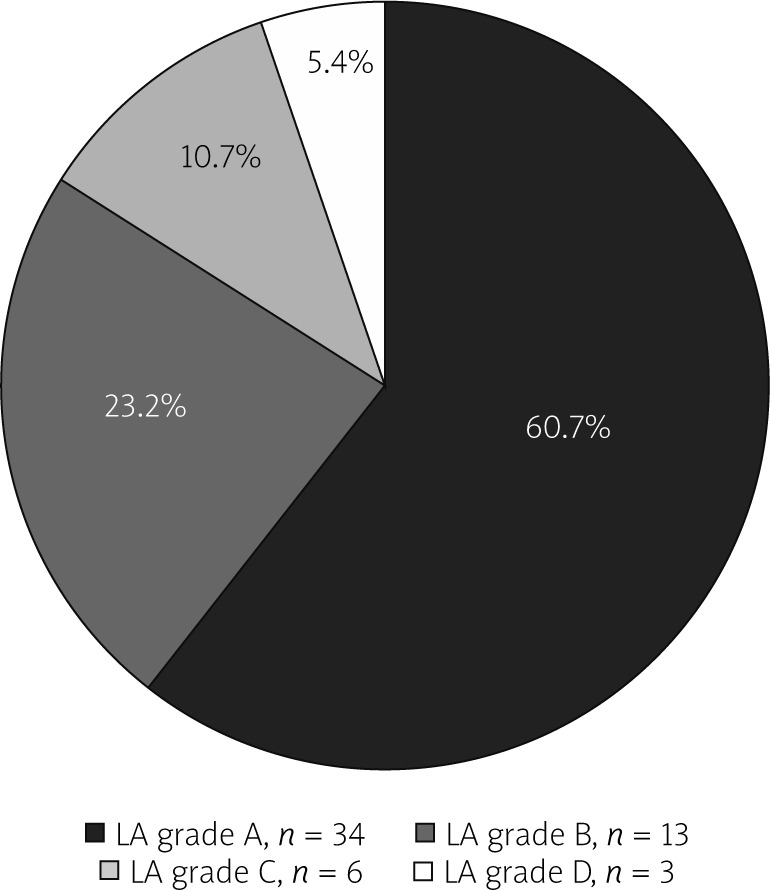
The most common significant findings were erosive GD (57/372, 15.3%). Significant lesions in age group ≥ 50 years comprised 45.7% (32/70), and in age group < 50 years 26.2% (79/302, p < 0.001). Esophagitis LA grade A was the most frequently encountered among all grades of esophagitis (34/56, 60.7%, p < 0.001) (Figure 1).
More severe forms of esophagitis occurred mainly in age group ≥ 50 years (15/56, 26.8%) versus age group < 50 years (7/56, 12.5%, p < 0.001). Duodenal ulcers occurred more often in age group < 50 years (21/25, 84%) versus age group > 50 years (4/25, 16%), p < 0.001. Two patients presented with gastric ulcer and three with gastric cancer, all occurred in age > 50 years. Anaemia, weight loss, and drug use (NSAIDs, aspirin, and clopidogrel) were more common in age group ≥ 50 years (Table III).
Table III
Age groups in relation to alarm features and drug use
| Variable, number | Age < 50 years | Age ≥ 50 years | P-value | ||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Weight loss, 14 | 3 | 21.4 | 11 | 78.6 | 0.001 |
| Anaemia, 19 | 6 | 31.6 | 13 | 68.4 | 0.001 |
| Vomiting, 55 | 45 | 81.8 | 10 | 18.2 | 0.001 |
| Drugs, 24 | 9 | 37.5 | 15 | 62.5 | 0.001 |
Vomiting occurred mainly in age group < 50 years (45/55, 81.8%). Significant lesions with vomiting was manifested only in 32.7% (18/55, p < 0.001) of patients (Table IV).
Table IV
Distribution of lesions among patients with alarm features and drug use
Weight loss and anaemia were associated with significant lesions in 85.7% (12/14, p < 0.001) and 84.2% (16/19, p < 0.001), respectively. Lesions associated with drug use (NSAIDs, aspirin, and clopidogrel) are depicted in Table IV). Among patients with normal endoscopic findings with no apparent organic lesion (FD), H. pylori infection prevalence was 47.7% (51/107), affecting 29 females and 22 males.
Discussion
Worldwide endoscopy for dyspepsia is performed for inappropriate indications [10]. To limit this high influx of referred patients, certain strategies need to be considered. In the current study, the majority of affected patients were below 50 years age (302/372, 81.2%) with a mean of 36 years. In developed nations, due to a higher prevalence of elderly populations, the affected patients are elderly [11]. Females predominated. Female gender has been reported as a risk factor for FD and a meta-analytical study by Kim and Kim reported a higher prevalence in female gender in different regions of the world [12]. Of all the patients, 61.6% presented with epigastric pain. Three studies from the USA, Brazil, and Iran reported similar findings of epigastric pain as the main presenting complaint of dyspepsia of 76.6%, 68%, and 67%, respectively [9, 13, 14]. Talley reported that, of patients with FD, approximately 38% manifested PDS, 27% EPS, and 35% have criteria for both [15]. When dyspepsia is investigated by endoscopy, a significant proportion of patients display negative findings, whereas the positive findings are mainly GD, esophagitis, peptic ulcers and neoplasms with variable rates. Harer and Hasler reported that 70% of patients with dyspepsia have negative endoscopic findings and 50% to 60% are later classified as FD [4]. A study of 650 patients by Abdeljawad et al. from Atlanta (USA) revealed the following endoscopic findings: normal and minor findings 49.4%, non-erosive GD 36.9%, erosive GD 7.4%, esophagitis 7.9%, peptic ulcers 4.3%, and malignancy 0.8% [9]. Another study of 1400 patients from Egypt by Gado et al. found normal and minor findings in 65%, peptic ulcers 18%, esophagitis 14%, erosive GD 8%, and gastric malignancy 1% [16]. We reported a higher frequency of significant endoscopic lesions in age groups ≥ 50 years (45.7%) versus groups below 50 years (26.2%, p < 0.001). It is well known that the aging process is associated with a higher frequency of significant GI lesions [17]. Endoscopy has a limited sensitivity in diagnosis of GERD, whereas 24-hour ambulatory PH monitoring with impedance has higher accuracy in diagnosis [18]. Frequently patients with reflux symptoms manifest normal or mild oesophageal mucosal lesions and even such symptoms might be functional in origin [19]. We reported a higher frequency and more severe lesions of esophagitis in age group ≥ 50 years. It has been observed that GERD is more common in the elderly and the mucosal lesions are more severe [20]. In our series, duodenal ulcers afflicted mainly younger age groups. In Europe, the United States, and many other industrialized countries, duodenal ulcers affect older age groups [21]. Weight loss and anaemia were more common in patients ≥ 50 years, with a rate of 11/14 (78.6%) and 13/19 (68.4%) respectively. This is likely due to association of more serious and severe lesions with older age groups [17]. Unlike vomiting, the majority of patients who displayed weight loss and anaemia showed significant and serious endoscopic findings with a rate of (12/14, 85.7%) and (16/19, 84.2%) respectively. Though persistent or recurrent vomiting is regarded as an alarm feature, in 67.3% (37/55) of patients the endoscopic findings were non-significant and occurred mainly in age group < 50 years (45/55, 81.8%). Vomiting might be functional in origin without underlying organic disorder, and according to Rome IV criteria, two such syndromes are recognized, i.e. chronic nausea and vomiting syndrome and cyclic vomiting syndrome [22]. Vomiting would be a more serious symptom if it occurs in the elderly, and is associated with other alarm features. Not all cases of dyspepsia with alarm features are associated with serious underlying lesions. It was reported that alarm features predict cancer in 11% of patients [1]. NSAIDs are regarded as a risk factor for dyspepsia [4]. Such drugs are implicated in different types of GI lesions of variable severity, ranging from mild mucosal erythema, erosions and ulcerations, to bleeding, perforation, and obstruction [23]. NSAIDs are commonly used by the elderly. In our study, 62.5% of patients aged ≥ 50 years (15/24, p < 0.001) used drugs, and it was associated in 58.3% (14/24, p = 0.04) with significant GI lesions. Of our patients (261/372) 70.2% displayed non-significant and normal findings. Uninvestigated dyspepsia is commonly encountered in the outpatient setting and frequently clinicians refer patients to endoscopy without consideration of guideline criteria. Both the patient and the clinician harbour a sense of fear that there might be a significant or serious lesion underlying dyspepsia, so clinicians frequently request endoscopy regardless of age and alarm features. According to the American College of Gastroenterology (ACG) and Canadian Association of Gastroenterology (CAG), (endoscopy is recommended for patients with dyspepsia-aged ≥ 60 years), and could be offered to younger patients if risk factors for malignancy exist [24]. The United European Gastroenterology (UEG) (2021) recommends endoscopy for FD to establish diagnosis and exclude organic diseases, at the age of 45–60, and in the presence of alarm features regardless of age [25]. In Korea, the age of requesting endoscopy is ≥ 40 years [26], due to a higher prevalence of gastric cancer in younger age groups. Iraq is a Middle Eastern country with a high prevalence of H. pylori infection. A review article by Khedmat et al. found the prevalence of H. pylori infection in the general population of several Middle Eastern countries to be in the range of 50–80% [27]. Majority of infected patients are asymptomatic [28]. According to recommendations of the European Helicobacter Study Group (EHSG), H. pylori eradication is indicated in infected patients with investigated non-ulcer dyspepsia and requested a test and treat policy for those with uninvestigated dyspepsia [29]. Eradication of H. pylori infection does not guarantee resolution of FD-related symptoms [30]. In areas with a low H. pylori prevalence, a test and treat policy might be beneficial, whereas in Iraq with a high H. pylori prevalence, this trend is not always true and practical. Majority of patients with dyspepsia can be treated in outpatient clinics by dietary modifications, pharmacotherapy (antacids, proton pump inhibitors, prokinetics, antispasmodics, and tricyclic antidepressants) or psychotherapy, and if symptoms persist, H. pylori testing is requested and treated accordingly. Overall, endoscopy for dyspepsia is recommended for selected cases according to clinical guidelines that includes, older age groups, presence of alarm features regardless of age, persistent or recurrent symptoms, and failure of therapy.
This study is limited by being a single hospital-based study with a relatively small sample of patients. Larger studies from multiple national centres are needed to accurately assess proper use of endoscopy in dyspepsia, aiming to limit waste of health resources.
Conclusions
Upper GI endoscopy in the case of uninvestigated dyspepsia revealed normal and non-significant findings in two thirds of patients. Significant lesions occurred mainly in the age group ≥ 50 years, along with presence of alarm features, and use of NSAIDs. Clinicians should adopt the international guidelines for performing endoscopy in patients presenting with dyspepsia. Unnecessary procedures consume financial health resources and are not always safe.











