
A 42-year-old male patient with chronic pancreatitis secondary to alcohol consumption was admitted to our department with complaints of severe abdominal pain and weight loss of about 25 kg within the last 2 months. Abdominal contrast-enhanced computed tomography was performed, revealing a pseudocyst (43 × 45 mm) in the pancreatic head (Figures 1 A, B), which caused duodenal stenosis and communicated with the dilated main pancreatic duct (MPD). The patient was qualified for endoscopic treatment; however, endoscopic ultrasound (EUS) imaging revealed that the pancreatic pseudocyst was surrounded by extensive inflammatory infiltration involving the duodenal wall. EUS-guided transmural drainage of the pseudocyst was not suitable because the distance between the lumen of the gastrointestinal tract and the lumen of the pseudocyst exceeded 30 mm, as shown in EUS imaging. During the endoscopic examination, inflammatory infiltration of the duodenal wall that narrowed the lumen of the gastrointestinal tract lumen was detected. It was also impossible to introduce the endoscope into the descending duodenum in order to localize the major duodenal papilla during endoscopic retrograde cholangiopancreatography (ERCP) for subsequent endoscopic transpapillary drainage of the pancreatic pseudocyst. Therefore, we decided to perform the EUS-guided rendezvous manoeuvre. A 19G needle was used to perform an EUS-guided puncture of the dilated MPD across the posterior wall of the gastric antrum. Contrast was administered via the needle, and this filled the MPD along its entire length (antegrade pancreatography), revealing partial disruption of the MPD within the pancreatic head, which resulted to leakage of contrast agent into the lumen of the pancreatic pseudocyst (Figure 1 C). The needle was used for transmural/transgastric introduction of a guidewire into the MPD, and the distal tip of the guidewire was placed within the duodenal bulb after passing it through the major duodenal papilla (Figures 1 D, E). The echoendoscope was then switched to a duodenoscope with the guidewire remaining in the transmural position within the lumen of the MPD and the duodenum. The duodenoscope was introduced into the duodenal bulb and the guidewire was grasped using endoscopic forceps. The MPD was catheterized selectively via the duodenal papilla (Figure 1 F). A 12-cm, 7-Fr pancreatic stent was then introduced along the guidewire, and its distal end was placed within the pancreatic tail so as to bridge the disruption’s site of the duct within the pancreatic head (Figures 1 G, H). The patient’s complaints were completely resolved during the postoperative period, and he was discharged home in good general condition with a recommendation to present for elective hospitalization in order to continue pancreatic endotherapy after 3 months.
Figure 1
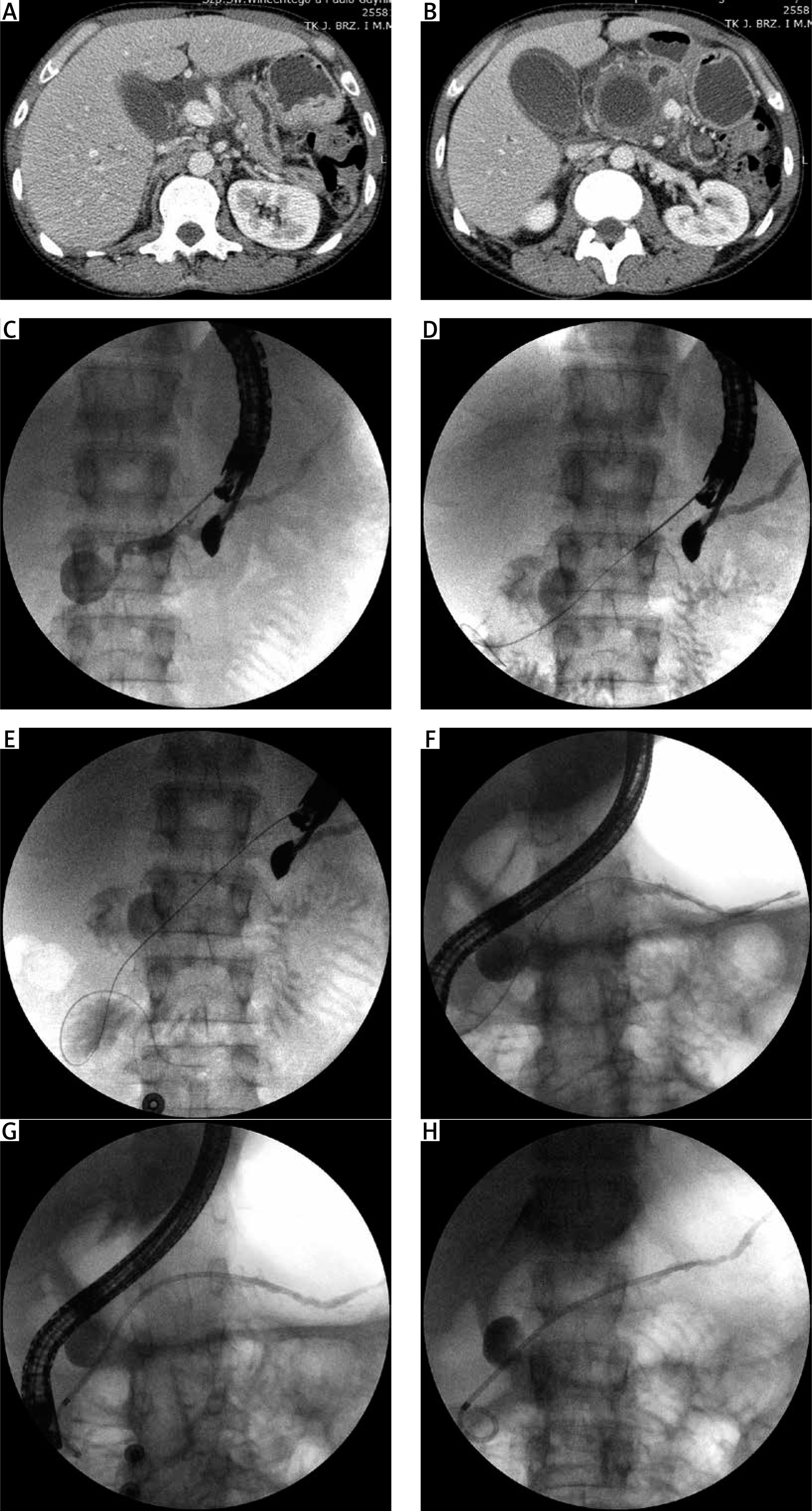
Abdominal contrast-enhanced computed tomography scans (A, B) showing a pancreatic pseudocyst communicating with the dilated MPD. Fluoroscopic images showing the subsequent steps of EUS-guided rendezvous manoeuvre (C–H) at the MPD. C – Partial disruption of MPD and pancreatic pseudocyst are visible during antegrade pancreatography. D, E – A guidewire was introduced into the MPD, and the distal tip of the guidewire was placed within the duodenal bulb after passing it through the major duodenal papilla. F – The MPD was catheterized selectively through the major duodenal papilla. G, H – A 7-Fr pancreatic stent was introduced along the guidewire, and its distal end was placed within the pancreatic tail so as to bridge the disruption’s site of the MPD within the pancreatic head
EUS-guided pancreatic duct interventions are challenging for endoscopists and remain a casuistic concept in pancreatic disease treatment [1–3]. In this case, the use of EUS-guided rendezvous technique facilitated introduction of a pancreatic stent to MPD with transpapillary drainage of the pancreatic pseudocyst. This led to decompression of the pancreatic ducts and complete resolution of symptoms related to elevated pressure within the MPD in a patient with a complicated history of chronic pancreatitis. Despite the inefficiency of ERCP, open surgery was avoided due to the use of advanced endoscopic techniques for pancreatic treatment.











