
Introduction
Type 1 diabetes mellitus (T1D) is the most common endocrinological disease in the paediatric population, with an incidence that has been increasing worldwide. According to the International Diabetes Federation, there were 201,000 estimated new cases in 2022 under the age of 20 years, and around 1.52 million children and adolescents are affected globally [1]. It is a multifactorial autoimmune disease, whose onset may be triggered by environmental stimuli, such as viral infections, in genetically predisposed individuals [2]. Diabetic ketoacidosis (DKA) is the most severe complication of T1D, which occurs due to the accumulation of ketone bodies, in the absence of insulin. It can be rapidly progressive and potentially fatal and therefore requires immediate medical treatment [3]. Factors such as delay in diagnosis, viral infections, younger ages (specially under 2 years), absence of direct family members with T1D and disadvantaged economic status with limited access to healthcare are known to be important risk factors for DKA [4].
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first reported in December 2019, and declared a global pandemic by the World Health Organization in March 2020 [5]. Strategies were implemented across the globe to mitigate this threat, such as hygiene measures, testing, isolation, quarantine and lockdown of public services [5, 6].
The pandemic period has been associated with an increase in frequency and severity of DKA in new-onset T1D [4, 7, 8], probably due to a delay in diagnosis and treatment as a result of parental avoidance of hospital visits and travel restrictions during lockdown periods. COVID-19 infection has also been reported to increase the risk for DKA due to an increase in insulin resistance [9]. After this period of constraint, the population and health institutions slowly returned to their usual activity.
Aim of the study
The aim of this study was to report and characterize the severity at presentation of new-onset T1D cases diagnosed in a single tertiary paediatric hospital, after the COVID-19 pandemic, and compare them to cases diagnosed during and before the pandemic.
Material and methods
An observational and retrospective cohort study was performed, with a review of digital clinical records of all patients diagnosed with new-onset T1D admitted to the emergency department of a single paediatric centre, between March 2016 and March 2024. Patients transferred to this hospital for clinical stabilization only, without subsequent follow-up in this centre, were excluded.
Demographic (age), clinical (duration of symptoms, percentage of weight loss), and laboratory (venous blood gas, glycaemia, HbA1c, ketonaemia and bicarbonate level) variables on admission were evaluated. Autoantibody positivity for islet cell antibodies (ICA), insulin auto-antibodies (IAA) and anti-glutamic acid decarboxylase antibodies (GADA) at diagnosis, was also documented.
DKA was defined according to the International Society for Paediatric and Adolescent Diabetes 2022 criteria as hyper- glycaemia (blood glucose > 200 mg/dl), acidosis (venous pH < 7.3 or serum bicarbonate < 18 mmol/l), and ketonaemia (ß-hydroxybutyrate ≥ 3 mmol/l). Mild DKA was defined as venous pH < 7.3 or serum bicarbonate < 18 mmol/l, moderate DKA as pH < 7.2 or serum bicarbonate < 10 mmol/l, and severe DKA as pH < 7.1 or serum bicarbonate < 5 mmol/l [10].
The sample was divided into three groups according to the year of diagnosis: pre-pandemic from March 2016 to March 2020, pandemic from March 2020 to March 2021 and post-pandemic from March 2021 to March 2024.
Statistical analysis was performed using SPSS Statistics version 28 software. The Kolmogorov–Smirnov test was used to evaluate the normal distribution of variables. Differences between the pre-pandemic, pandemic, and post-pandemic groups were tested using Poisson regression analysis for incidence, the ANOVA test for numeric variables that followed a normal distribution, the Kruskal–Wallis test for numeric variables that did not follow a normal distribution, and the χ2 test for nominal variables, p < 0.05 was considered significant.
The study was approved by the Ethics Committee of Unidade Local de Saúde de Coimbra, process number: PI 2025-ESI.SF-85, and the ethical recommendations established by the Declaration of Helsinki of the World Medical Association were followed.
Results
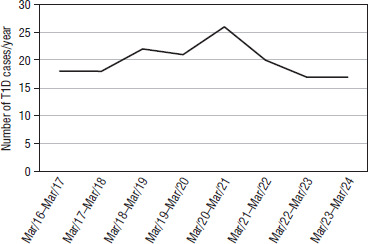
A total of 159 cases of new-onset T1D were diagnosed: 79 in the pre-pandemic group, with 19.8 cases/year, 26 in the pandemic year, and 54 in the post-pandemic group, with 18.0 cases/year. When comparing incidence rates between groups, no statistically significant differences were found (Table I).
Table I
Glycemic means and hypoglycemia frequencies in both groups under the insulin tolerance test
| Rate ratio | 95% confidence interval | p-value | |
|---|---|---|---|
| Pandemic vs. pre-pandemic | 1.27 | 0.82–1.97 | 0.27 |
| Post-pandemic vs. pandemic | 0.71 | 0.42–1.21 | 0.21 |
| Post-pandemic vs. pre-pandemic | 0.90 | 0.66–1.22 | 0.54 |
The number of new-onset T1D cases diagnosed each year are presented in Figure 1. All analysed parameters are presented in detail in the relevant tables.
The proportion of patients who presented with DKA was 31.6% in the pre-pandemic group, 57.7% in the pandemic group, and 37.0% in the post-pandemic group (p = 0.059). Severe DKA was present in 10.1% of patients in the pre-pandemic group, 23.1% in the pandemic group and 13.0% in the post-pandemic group (p = 0.239). When grouping moderate and severe DKA, it was present in 16.4% of patients in the pre-pandemic group, 46.2% in the pandemic group and 20.4% in the post-pandemic group (p pre-pandemic vs. pandemic = 0.006, p pandemic vs. post-pandemic = 0.051, p pre-pandemic vs. post-pandemic = 0.564). The severity of DKA at presentation is reported in Table II. Although not statistically significant, there was an improvement in the rate of DKA in the post-pandemic period, after an increase in the pandemic year.
Table II
Presentation by severity across the three groups
Regarding clinical presentation (Table III), mean weight loss was 6.5% in the pre-pandemic period, 10.2% in the pandemic period and 7.4% in the post-pandemic group. There was a significantly greater weight loss in the pandemic year, compared with the pre-pandemic period (p = 0.020). There was no difference across the three groups regarding mean age at diagnosis and duration of symptoms.
Table III
Demographic data and clinical presentation
When considering the initial analytical investigation (Table IV), mean ketonaemia was significantly higher in the pandemic period (5.1 mmol/l vs. 3.0 and 3.1 in pre-pandemic and post-pandemic groups, p < 0.001 and p < 0.001). There was a significantly lower mean pH in the pandemic group (7.19 vs. 7.31 and 7.32 in pre-pandemic and post-pandemic groups, p < 0.001 and p = 0.002) and lower HCO3 (14.2 mmol/l vs. 19.3 and 20.5 mmol/l in pre-pandemic and post-pandemic groups, p < 0.001 and p = 0.011). Mean glucose and HbA1c values at diagnosis were stable in all three groups, with no statistically significant difference. There were no significant differences in any variable when comparing values between the pre-pandemic and post-pandemic periods.
Table IV
Initial investigation
In our centre, all patients undergo autoantibody testing at diagnosis for ICA, IAA and GADA. No significant difference was found between the three periods. The number and percentage of patients with positive autoimmunity are presented in Table V.
Table V
Autoimmunity positivity at diagnosis across the groups
Discussion
Many studies on the incidence of newly diagnosed T1D during the pandemic period yield conflicting results: some suggest an increase in incidence, while others report a decrease or no change compared to pre-pandemic levels [4, 8, 11, 12]. In this study, no significant difference was found in the number of cases per year. Others have reported an increased incidence in new-onset T1D [4, 8, 13], with a more than usual annual rise (3–4% vs. 9.5%) in the incidence of T1D during the pandemic period compared to the pre-pandemic years [13]. In this study, a much larger increase in incidence was observed (31%), possibly due to the unicentric nature of the study and to the fact that our hospital is a reference centre for diabetes treatment. The lack of statistical significance may be attributed to the small sample size. Regarding severity at presentation, several studies have documented an increase in DKA at diagnosis [8, 14, 15], with an incidence of approximately 30% of patients presenting with DKA in the pre-pandemic period, compared to rates as high as 40–60% in the pandemic year [14, 16]. The DKA rates observed in this study (31.6% in the pre-pandemic group and 57.7% in the pandemic group) are in accordance with the previously described rates worldwide. This surge might be explained by a delay in diagnosis during the pandemic year due to parental avoidance of hospital visits in fear of acquiring COVID-19 infection, limited access to medical care, restriction of transportation during lockdown periods, and failure to recognize DKA symptoms [4, 9, 13].
Little is still known about the trends in frequency and severity of new-onset T1D after the pandemic period. It would be expected that after the reduction in confinement bans, and easier access to medical care, there would be a return to the patterns observed in the pre-pandemic period. A study in Turkey reported higher frequency of moderate and severe acidosis during the pandemic period, compared to the pre-pandemic years, with improvement to its previous levels over time. However, a significant difference was still found when comparing DKA rates in the post-pandemic and pre-pandemic periods [6]. In our study, a significant improvement was noted with respect to the severity at presentation in the post-pandemic group. Although statistically we have returned to the pre-pandemic reality, with no difference found between the pre-pandemic and post-pandemic groups, consideration of the absolute values suggests that there is still room for improvement. Patient education on early recognition of T1D symptoms, prompt diagnosis, and timely initiation of treatment are essential to reduce the rates of DKA at onset of T1D.
However, the ketoacidosis rate remains high and a concerning matter, so focus must remain on implementing preventative measures. Screening for those at higher risk of T1D has been studied and implemented in various countries, both concerning relatives of patients and population-based screening [17–19]. In a research setting, screening might include the use of genetic risk factors such as human leukocyte antigen genotype or a polygenic risk score to identify which children will benefit from measurement of T1D-associated islet autoantibodies. Clinically, the only recommended tests to diagnose early stages of T1D are islet autoantibodies [18, 20]. The ideal age for screening is still under discussion. Pre-school age has shown good sensitivity and benefits from overlapping with vaccination health visits. However, it misses younger children, who typically present with greater severity, as well as older patients, who might seroconvert later in life [20].
T1D screening enables lower median HbA1c, lower median fasting glucose and higher median fasting C-peptide levels at diagnosis in those screened compared to children with no previous early diagnosis. Additionally, significantly lower rates of DKA at the time of T1D stage 3 diagnosis (decrease from 25–62% to 2.5–6%), as well as lower rates of hospitalisation and intensive care admissions, are reported in the former group [18, 21].
With the availability of new therapies to delay or prevent T1D, such as the recent approval of teplizumab for stage 2 T1D, the World Health Organization’s criteria for screening the general population have been satisfied for T1D. This presents a great opportunity to dramatically change the future of this disease, by identifying individuals who could benefit from these interventions [18, 20].
An earlier cost-benefit analysis of screening in the general population showed that the costs far outweighed the economic benefits. Nonetheless, more recent studies suggest cost-effectiveness with DKA reduction and delay therapies [21]. Individuals with positive screening will need monitoring for disease progression, which should include metabolic monitoring, patient education and psychological support [22].
A reported disadvantage is the risk of a negative psychological impact on those who achieve positive screening results, although this stress seems to decrease with time and be lower at the time of stage 3 T1D diagnosis than in parents whose children have not been screened [18, 23].
The optimal screening design – regarding age, screening setting and strategies to overcome recruitment challenges – remains to be determined. Future studies should include larger and more diverse populations [19].
It is still debated whether SARS-CoV-2 might be responsible for the development of T1D by direct mechanisms of damage to pancreatic β-cells or by triggering autoimmune processes similarly to other viral infections [13, 24]. In this study, no definite conclusions can be drawn on this topic, as there were only two cases of concomitant SARS-CoV-2 infection at the time of T1D diagnosis, and serological studies were not available. Regarding antibody development, no difference was found before, during and after the pandemic periods. A study reported a higher percentage of detectable insulinoma-associated antigen-2 antibodies (IA-2A) and triple autoantibody positivity (GADA, ICA, and IA-2A) in the group of patients with positive SARS-CoV-2 serology [11].
The retrospective nature and single-centre design of the present study, as well as the lack of population data, may constitute limitations. More multi-centric, larger scale studies are needed to establish the improvement in incidence and severity of T1D after the pandemic period, as well as the possible role of SARS-CoV-2 in autoimmunity and disease development.
Conclusions
There was a lower severity of DKA presentation in new-onset T1D in the post-pandemic period, compared to the pandemic year, with analytical values similar to those observed in the period before the COVID-19 pandemic. This improvement was expected due to the improved access to healthcare. However, it is important to continue to implement measures to reduce the rate of DKA.









